To evaluate the solid focal liver lesions by Shear Wave Sonoelastography (SWE) and correlate Shear Wave Sonoelastography findings with that of FNAC.
50 patients who were diagnosed to have solid focal liver lesions on sonography during the period August 2017 to September 2019 at JSS Medical College and Hospital, Mysuru underwent Shear Wave Sonoelastography [SWE], following which patient underwent ultrasound guided FNAC for histological evaluation.
Benign vs. malignant hepatic lesions could be differentiated using a cut off value of 25 kPa. The overall sensitivity & specificity of SWE was found to be 66% and 30% respectively as a standalone technique, however the predicative accuracy of SWE in conjunction with gray scale sonographic findings was 91.4%.
Shear wave elastography can be used as an adjunct in routine sonological practice to evaluate solid focal lesions of the liver. It can help to categorize benign versus malignant lesions.
Shear Wave Sonoelastography (SWE), Kilopascals (kPa), Solid focal liver lesions (FLL), Fine needle aspiration cytology (FNAC)
The liver is the largest solid organ in the body and the only organ to perform functions of detoxification, metabolism of various substances and synthesis [1,2]. Focal liver lesions are commonly encountered in regular practice. As differentials for the same ranges from benign to malignant lesions, non-invasive characterization of the same is the need of the hour. Subjecting all patients with FLL to biopsy and histological examination has significant phase [3]. Ultrasonography of the abdomen is a very comprehensively reachable, reasonably priced, non-invasive, portable and convenient method of imaging [4]. Focal liver lesions for the most part comprise of abscess of the liver, the cystic lesions of the liver, primary malignant neoplasm, metastases, focal fatty infiltrations and hematomas [5-10].
Ultrasonography of the abdomen also has a very important task in the identification and the following up of the focal lesions of the liver [11-15]. Shear wave sono-elastography is a developing concept in the imaging modality of ultrasonography. As an adjunct to real time B-Mode ultrasound, 2D-SWE adds value in triage of focal liver lesions as benign or malignant based on intrinsic tissue parameters like tissue stiffness and tissue deformability.
SWE based sonography techniques are non-invasive, reproducible and cost effective. Various pathologies alter the normal tissue elasticity, evaluation of the same in correlation with normal qualitative and quantitative tissue elasticity aids in differentiation of the pathologies and categorizing them as benign or malignant thus obviating the need for biopsy.
Measurements acquired in SWE detect and quantify tissue stiffness in response to an applied mechanical force (compression or shear wave). SWE can also be used as a potential application to guide the exact site that needs FNAC in liver lesions [16-18]. There are currently few studies in the literature that have examined the role of this technique in the characterization of FLL.
The important advantages of SWE in imaging of the FLL are the non-invasiveness, no requirement of contrast material and lack of exposure to ionizing radiation and reproducibility. Studies evaluating SWE in hepatic pathologies have shown promising results, however those focusing on FLL are a small subset and the data for a definitive cut off kPa is inconclusive. The present study is aims to evaluate the accuracy of SWE in differentiation of solid hepatic focal lesions as benign or malignant lesions.
50 patients who were diagnosed to have solid focal liver lesions on sonography at Department of Radiodiagnosis, JSS Medical College and Hospital, Mysuru during the period August 2017 to September 2019 were enrolled for the study. All scans including SWE evaluation was done in Philips iu22, broadband convex 1-5 MHz probe configured for SWE.
Sonomethodology: Patient is positioned in right lateral position with the same side arm raised above in order to provide better visibility to the liver and the liver substance is visualized in the intercostal spaces to enable a good view of the liver parenchyma.
Focal lesions of the liver were evaluated by grey scale ultrasound for their size, echogenicity, and distance for the liver surface. SWE was performed with the region of interest (ROI) box (fixed dimension, 10 mm × 5 mm) placed within the lesion. Absolute stiffness measurements in the region of interest were obtained, minimum of 3 measurements was taken from the lesion, kPa of the lesion was the sum average of the 3 measurements. Elasticity of the lesions expressed in kilo-Pascal (kPa) and the stiffness score was given for each focal lesion.
Based on the scores the lesions were classified as benign and malignant lesions.
• Normal liver stiffness: up to 7.0 kPa (Normal hepatic parenchyma).
• Stiffness range for benign lesions: 7.1-25 kPa.
• Stiffness range for malignant lesion: > 25 kPa.
SWE values were documented. All patients underwent ultrasound guided FNAC (informed consent obtained), following histological diagnosis, the sonoelastography values were correlated with histopathological diagnosis. All patients with solid focal lesions of the liver like Hemangioma, Focal nodular hyperplasia (FNH), Hepatic adenoma, Focal fatty infiltration, Hepatic cellular carcinoma (HCC), Lymphoma, Kaposi's sarcoma, Hepatoblastoma and Metastasis were included in the study. Eight patients with FLL were excluded from the study owing to co-existence of diffuse liver disease or poor breath hold two with abnormal coagulation profile could not undergo FNAC, were also excluded from the study.
Data collected was entered in a Microsoft excel sheet and statistical analysis was done using software SPSS version 21, IBM for windows by Descriptive statistics, Chi-square test, and Unpaired t' test statistical methods with two sided p-value (significant with p value < 0.05).
In this study, predictive accuracy of the SWE in differentiating benign vs. malignant FLL was observed to be 50% as a stand-alone imaging technique, however in conjunction with gray-scale sonographic features, the predictive accuracy was found to be 91.4%.
Of the 50 patients enrolled in this study, 42% were in the age group of 31-50 years and the mean age was 58.64 years SD + 4.35 years. The average age of the benign lesions was 53.35 years, the average age of the malignant lesions was 61.67 years, the difference of age between the benign and malignant lesions was 0.002, and this difference was statistically significant, indicating that benign lesions tend to occur in the younger age group. A definite male predominance was noted, 72% of the patients enrolled were males, of these, 31% had benign lesions and 69% had malignant lesions, this sex distribution and occurrence of malignant lesions is male was statistically significant with p value < 0.05 (Graph 1).
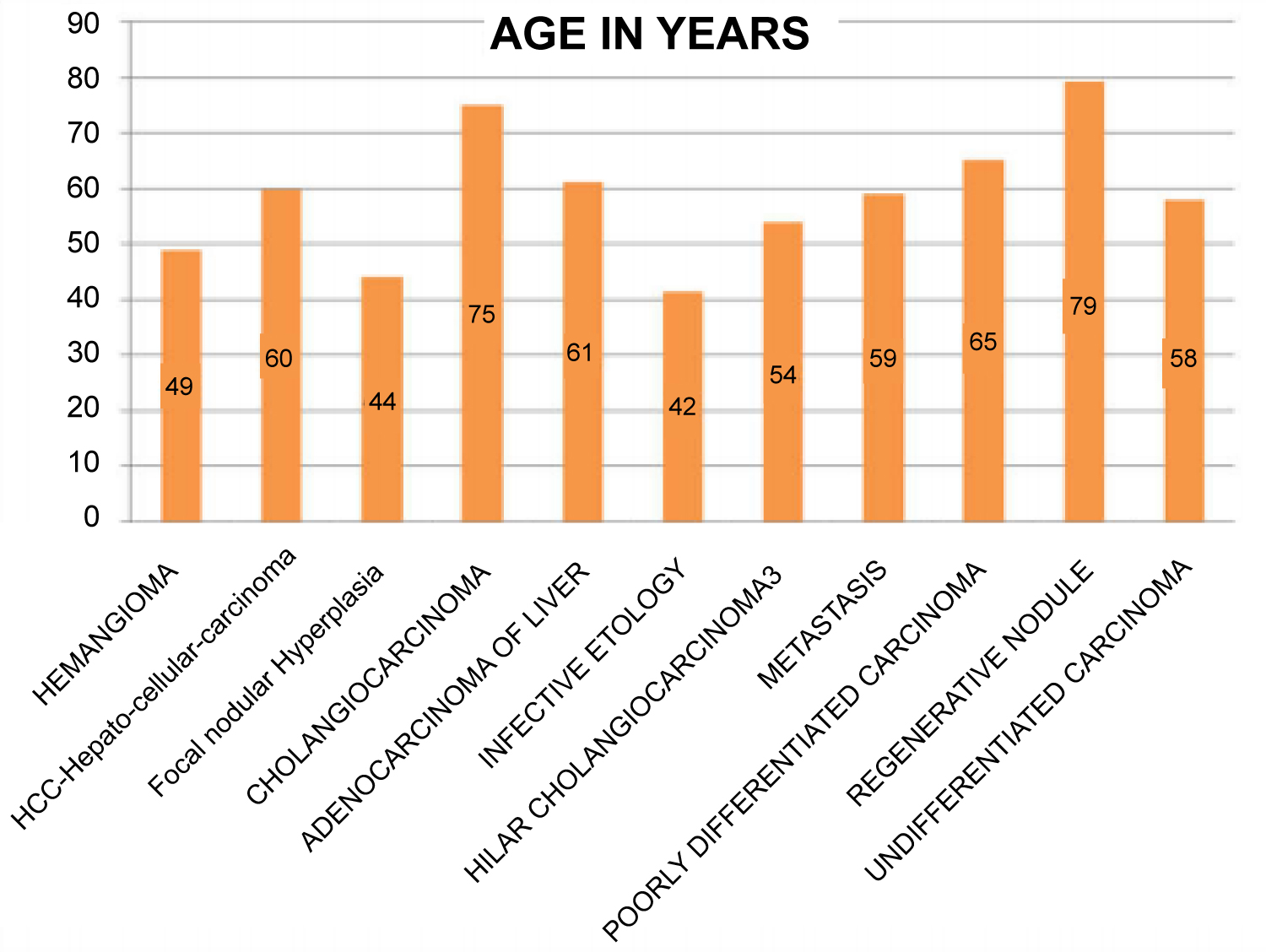 Graph 1: Age vs. Focal liver lesions.
View Graph 1
Graph 1: Age vs. Focal liver lesions.
View Graph 1
50 patients had solid focal lesions of the liver on ultrasound and were evaluated with shear wave elastography. A cut off value of 25 kPa was set to differentiate between malignant and benign lesions. Grgurevic, et al. in their study, found lesion stiffness < 14 kPa had NPV of 96%, while values > 32.5 kPa had PPV of 96% for malignancy [18]. Range for kPa for indeterminate lesions was wide, an arbitrary value of 25 kPa was used in this study.
Of the 50 patients, 17 had values > 25 kPa and 33 had values < 25 kPa (Figure 1a and Figure 1b). FNAC categorized 11 were benign and 36 were malignant and 3 were infective. 3 patients had infective lesions which sonographically appeared solid with SWE values up to 12 kPa with an average of 7.9 kPa with comparison to the normal average of 6 kPa.
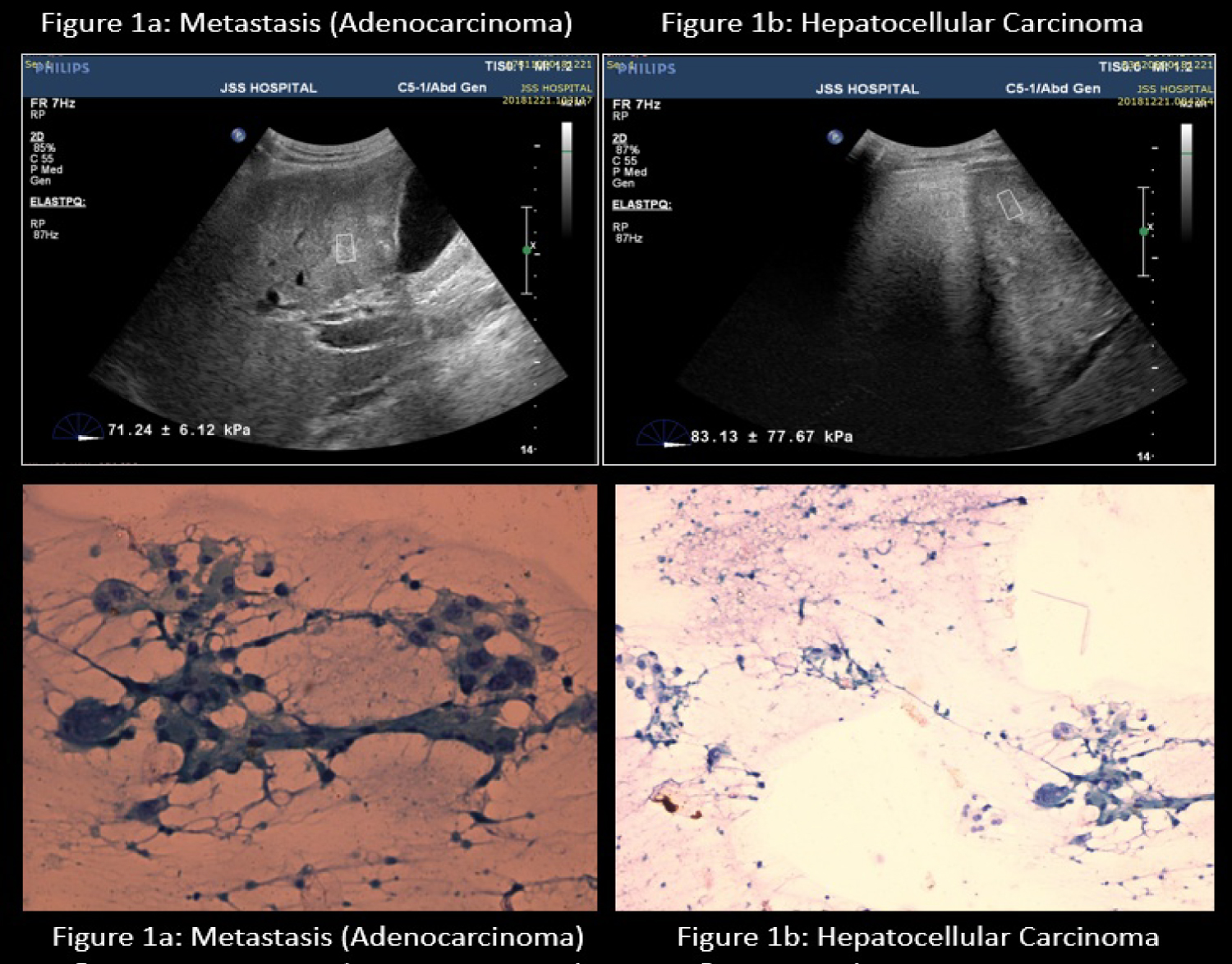 Figure 1 (a & b): Shear wave Sonoelastography of Malignant lesions & Correlative histopathology.
View Figure 1
Figure 1 (a & b): Shear wave Sonoelastography of Malignant lesions & Correlative histopathology.
View Figure 1
Overall the highest kPa values were encountered in hepatocellular carcinoma, followed by cholangiocarcinoma and metastatic adenocarcinoma. The highest SWE value was 46 kPa and 43 kPa respectively.
Of the 19 cases with hepatocellular carcinoma, 15 were male and 4 females with an average age of 54 years. The highest SWE value was 46 kpa with an average of 25.4 kpa with comparison to the normal average of 9 kpa.
SWE values for Benign lesions like Focal Nodular Hyperplasia, the highest SWE value was 18 kpa with an average of 10.4 kpa with comparison to the normal average of 3.4 kpa. In case of hepatic hemangiomas, the highest SWE value was 15 kpa with an average of 9.68 kpa with comparison to the normal average of 4.2 kpa (Graph 2).
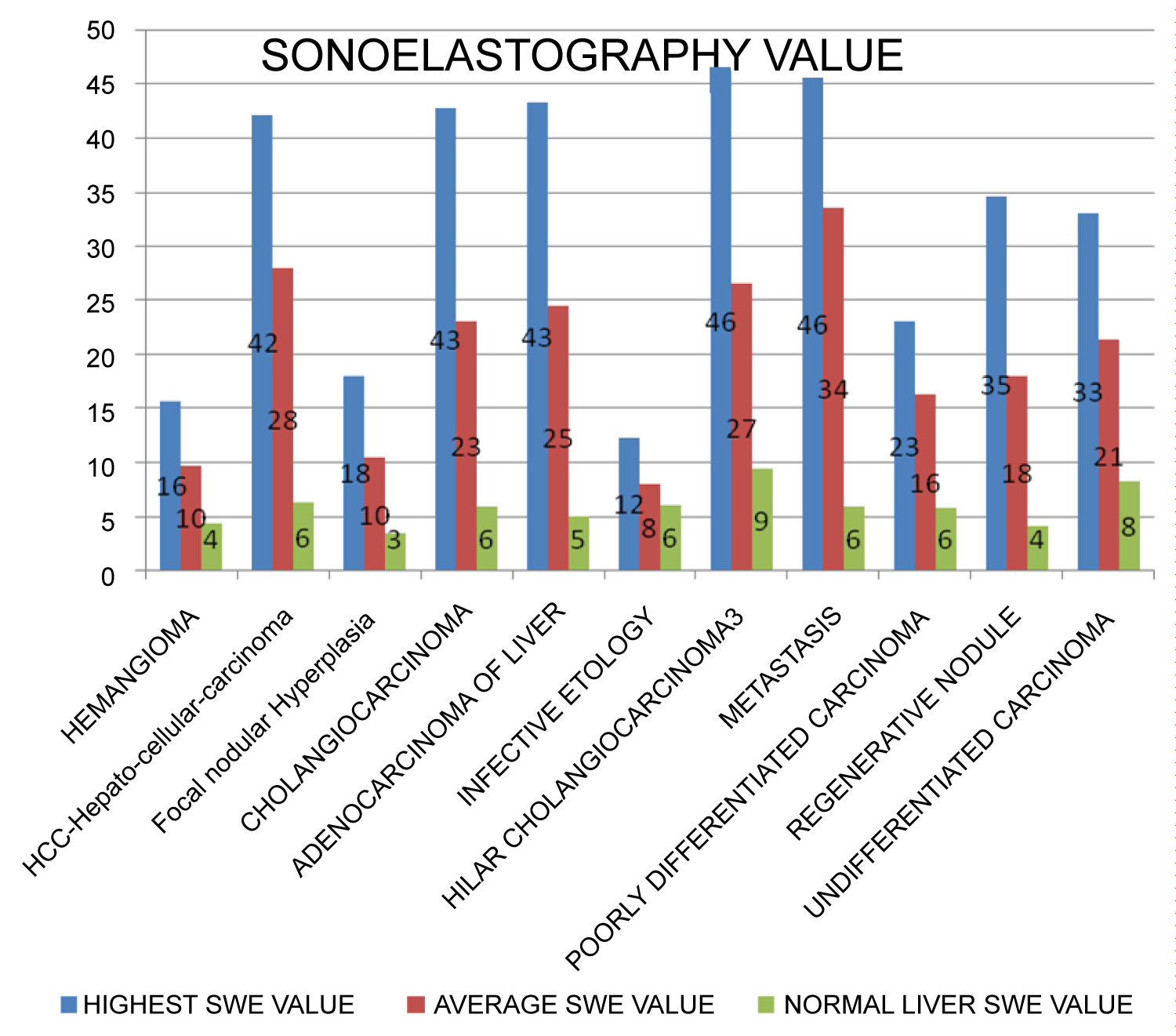 Graph 2: Comparison of Sonoelastography value of the lesion.
View Graph 2
Graph 2: Comparison of Sonoelastography value of the lesion.
View Graph 2
Differentiating malignant from benign liver lesions is imperative, however owing to the varied imaging appearances of FLLs, this can be daunting. Invasive procedures for histological diagnosis can be deferred if non-invasive imaging clues can be as accurate as histology. Recent years have witnessed significant advances in hepatobiliary imaging, one such technique that has evolved is Elastography.
Shear wave elastography is a quantitative radiation free non-invasive method that can help to clearly differentiate benign and malignant hepatic lesions. Park HS, et al. evaluated 136 FLLs in 118 patients with SWE for quantitative and qualitative assessment of stiffness. Stiffness values of malignant lesions (n = 85, 60.41 [47.81] kPa) were significantly higher than those of benign lesions (n = 51, 22.05 [17.24] kPa, P < 0.0001). Mean stiffness of hepatocellular carcinoma (45.72 [35.65] kPa) was significantly lower than that of metastasis (67.43 [43.39] kPa) and was significantly higher than benign FLLs (22.05 [17.24] kPa) [16]. Another study done by Valentina Cesario, et al. also concluded that percutaneous sonoelastography can differentiate benign versus malignant focal lesions of the liver, metastases, with good diagnostic performance [17]. Findings as observed in our study concurs with published literature till date pertaining to the accuracy observed [15,18]. As a corroborative imaging technique to B-Mode ultrasound, SWE in our study had a predictive accuracy of 91.43% [95% CI: 80.77%-97.78%].
Few limitations were observed, the limitations being the size of the lesion and the depth at which the lesion is located, as the maximum detection depth of SWE is limited. The transmission of an acoustic radiation impulse is allowed only up to 10 cm from the skin in SWE, owing to safety concerns. Heterogeneity and size of the lesions also were confounding variables. Nevertheless, in clinical practice, one criterion of cut-off value would be required for differentiating liver malignant lesions and our study we found the accuracy increased with a cut off of 25 kPa.
Shear wave elastography is a useful adjunct in routine 2D B-mode ultrasound in characterization of solid focal lesions of the liver. Incorporation of the same in routine evaluation of focal hepatic lesions will tailor the need for cross sectional imaging or histological examination.