Background: The aim of this study was to retrospectively evaluate epidemiology, distribution and radiological features of newly diagnosed benign bone tumors and tumor like lesions in our radiology department.
Methods: Computed tomography (CT) and/or magnetic resonance imaging (MRI) examinations performed between January 2018 and December 2019 in musculoskeletal radiology section were retrospectively re-evaluated by an experienced radiologist according to age, gender, radiological classification and location.
Results: There were 247 patients (106 females, 141 males) aged between 8 and 64 years (mean age 30.65 ± 15.7 years) with benign bone lesions diagnosed for the first time. Most common diagnosis was osteochondroma seen in 37% of the patients (n: 91). Mean age was 30.18 ± 17.7. There were a male dominance with 57 males (62.6%) and 34 females (37.4%). Respective mean ages for both sexes were 23.92 ± 12 and 39.22 ± 21.2. Lesions were most commonly located around knee joint. 35% of patients (n: 86; 47 female, 39 male) were diagnosed as enchondroma. Mean age was 34.9 ± 13.4. Most common location was femur.
Fibrous cortical defects and non-ossifying fibromas, collectively known as fibroxanthoma or metaphyseal fibrous defect, were the third common seen benign bone lesion with a percentage of 18 (n: 45). There were no sex predilection with 21 females and 24 males. Mean age was 25.66 ± 13.7, 51% of cases were seen in femur. Osteoid osteomas were comprised 10% of the cases (n: 25). There was a male predilection (21 males and 4 females) and long tubular bones were most common locations. Other rare lesions were not included into the study for statistical purposes.
Conclusion: Knowledge of the properties of benign bone tumors is important. Because they are rarely seen, the diagnosis may be delayed. Benign bone tumours are most frequent in children and young adults, although they may also present in later stages of life. The incidence of benign bone tumours varies depending on the type. The most common type is osteochondroma. Although plain radiography is essential for diagnosis, CT and MRI examinations provide additional information. Treatment is indicated for symptomatic patients and for the patients with a risk of pathological fracture or deformity. In conclusion our findings were overall consistent with the literature.
Benign, Bone, Tumor, Radiology, Epidemiology
CT: Computed Tomography; MRI: Magnetic Resonance Imaging
Primary bone tumors are rare, accounting for 0.2-0.5% of all malignancies, and most are benign in nature [1]. The actual incidence of benign bone tumors is controversial because most of the patients are asymptomatic and their presentations are unspecific thus these tumors remain largely undiagnosed [2-7].
The diagnoses of benign bone tumors are made mostly when radiological examinations are done for other conditions. Since many bone tumors have a predilection for age, sex and anatomic locations these information's may establish a first step in the diagnosis [8,9]. Data about epidemiology of musculoskeletal tumors is not profound and according to some researches distribution of primary bone tumors has variation in different regions around the globe [10-13]. Therefore, knowledge of the epidemiology in each region can be useful for early diagnose. In the diagnosis of benign bone tumors radiological examination is the most important step providing information in extent and nature of bone tumors and also in differential diagnosis. In addition to radiography, CT and MRI are very helpful in the diagnosis of solitary bone lesions [14]. The aim of this study was to retrospectively evaluate epidemiology, distribution and radiological features of newly diagnosed benign bone tumors in our radiology department.
This study was designed as a retrospective study. Computed tomography (CT) and/or magnetic resonance imaging (MRI) examinations performed between January 2018 and December 2019 in musculoskeletal radiology section of the radiology department were re-evaluated by an experienced radiologist. Benign bone lesions of the axial skeleton are not included into the study. Obtained data was analyzed according to age, gender, anatomic location and radiological diagnosis.
There were 247 patients (106 females, 141 males) aged between 8 and 64 years (mean age 30.65 ± 15.7 years) with benign bone tumors and tumor-like lesions diagnosed for the first time. Patients were grouped according to radiological diagnosis, age, gender, and anatomic location (Table 1).
Table 1: Distribution of benign bone tumors diagnosed in our radiology department between January 2018 and December 2019. View Table 1
Most common diagnosis was osteochondroma seen in 37% of the patients (n: 91). Mean age was 30.18 ± 17.7. There were a male dominance with 57 males (62.6%) and 34 females (37.4%). Respective mean ages for both sexes were 23.92 ± 12 and 39.22 ± 21.2. Lesions were most commonly located around knee joint especially at tibia (Figure 1). Other lesions were seen at humerus, scapula, phalanges of hand and iliac bone in decending order. In 8 patients lesions were multiple indicating osteochondromatosis. Cartilage cap thickness was measured in MRI examinations and being under 1.5 cm there was no malignant degeneration suspicion in the study population.
 Figure 1: Osteochondroma: (a) X-ray showing an osteochondroma arising from proximal metaphyseal region of right tibia in a 14-years-old female, (b) Axial CT image of left tibia of a 20-years-old male. Apedunculated osteochondroma can be seen on posteromedial aspect of tibia, (c) Axial T2W MRI image demonstrating an osteochondrome projecting from left femur of a 20-years-old male. Note the high signal of the cartilage cap.
View Figure 1
Figure 1: Osteochondroma: (a) X-ray showing an osteochondroma arising from proximal metaphyseal region of right tibia in a 14-years-old female, (b) Axial CT image of left tibia of a 20-years-old male. Apedunculated osteochondroma can be seen on posteromedial aspect of tibia, (c) Axial T2W MRI image demonstrating an osteochondrome projecting from left femur of a 20-years-old male. Note the high signal of the cartilage cap.
View Figure 1
86 patients, 35% of study population, were diagnosed as enchondroma. 47 patients were female where as 39 patients were male. Mean age was 34.9 ± 13.4. Most common location was femur (Figure 2), followed by tubular bones of hand (Figure 3a). Rare locations such as iliac bone were also encountered (Figure 3b).
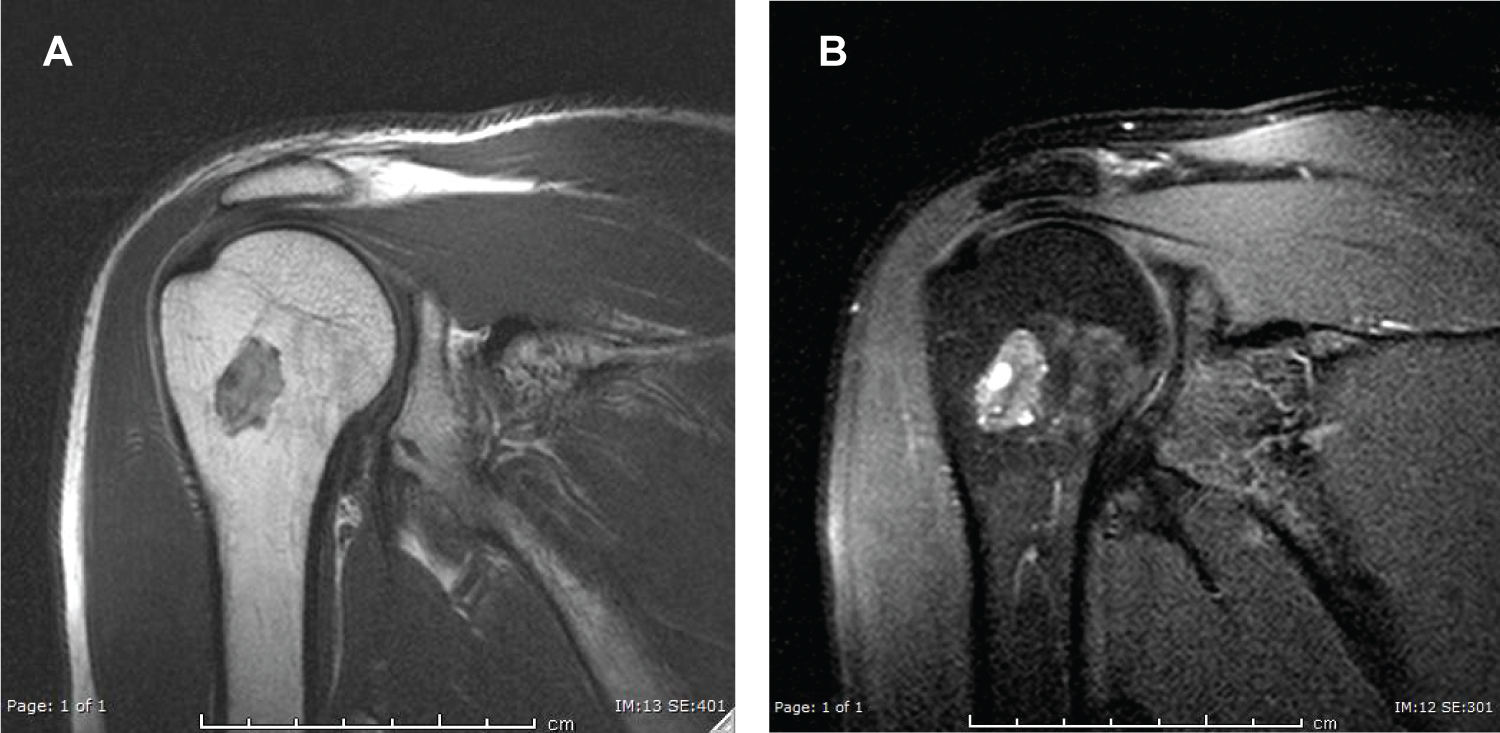 Figure 2: Enchondroma in 40-years-old male: (a) T1W and (b) T2W coronal MRI images of right humerus showing intramedullary located lesion at proximal metaphyseal region.
View Figure 2
Figure 2: Enchondroma in 40-years-old male: (a) T1W and (b) T2W coronal MRI images of right humerus showing intramedullary located lesion at proximal metaphyseal region.
View Figure 2
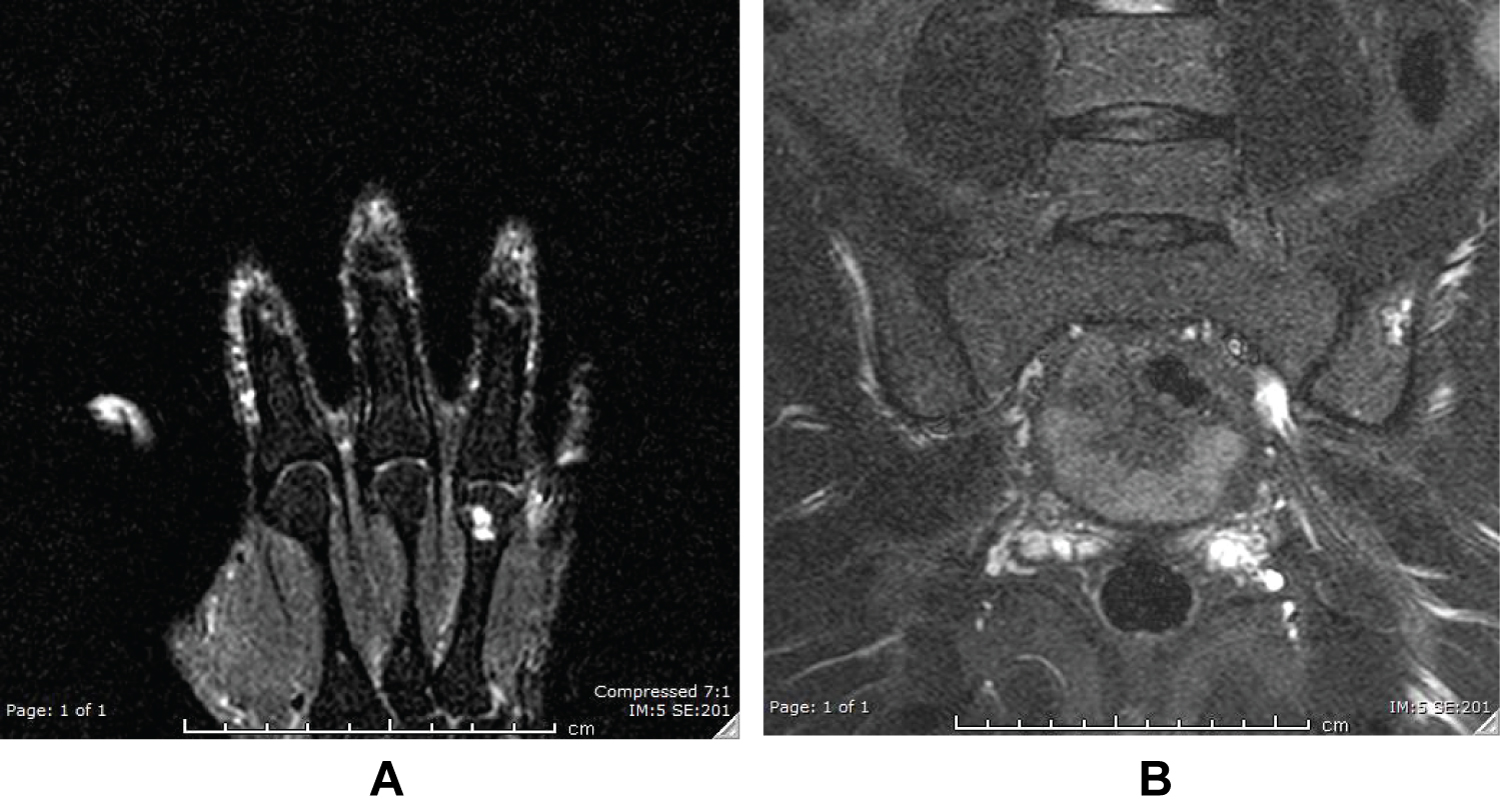 Figure 3: Enchondroma: (a) located at 4th metacarpal bone in a 68-years-old male which is a common location for enchondroma; (b) located at left iliac bone in 34-years-old male which is a rare location for enchondroma. On both T2W coronal MRI images typical background high signal is noted.
View Figure 3
Figure 3: Enchondroma: (a) located at 4th metacarpal bone in a 68-years-old male which is a common location for enchondroma; (b) located at left iliac bone in 34-years-old male which is a rare location for enchondroma. On both T2W coronal MRI images typical background high signal is noted.
View Figure 3
Fibrous cortical defects and non-ossifying fibromas, collectively known as fibroxanthoma or metaphyseal fibrous defect, were the third common seen benign bone lesion in the study population with a percentage of 18 (n: 45). There were no sex predilection with 21 females and 24 males. Mean age was 25.66 ± 13.7. %51 of cases were seen in femur (Figure 4).
 Figure 4: Metaphyseal fibrous defect in left femur of a 20-years-old female: (a) X-ray and (b) coronal T2W MRI image showing non-neoplastic fibrous bone lesion in distal metaphysis-diaphysis.
View Figure 4
Figure 4: Metaphyseal fibrous defect in left femur of a 20-years-old female: (a) X-ray and (b) coronal T2W MRI image showing non-neoplastic fibrous bone lesion in distal metaphysis-diaphysis.
View Figure 4
Osteoid osteomas were comprised 10% of the cases (n: 25). There was a male predilection (21 males and 4 females) and long tubular bones were most common locations (Figure 5).
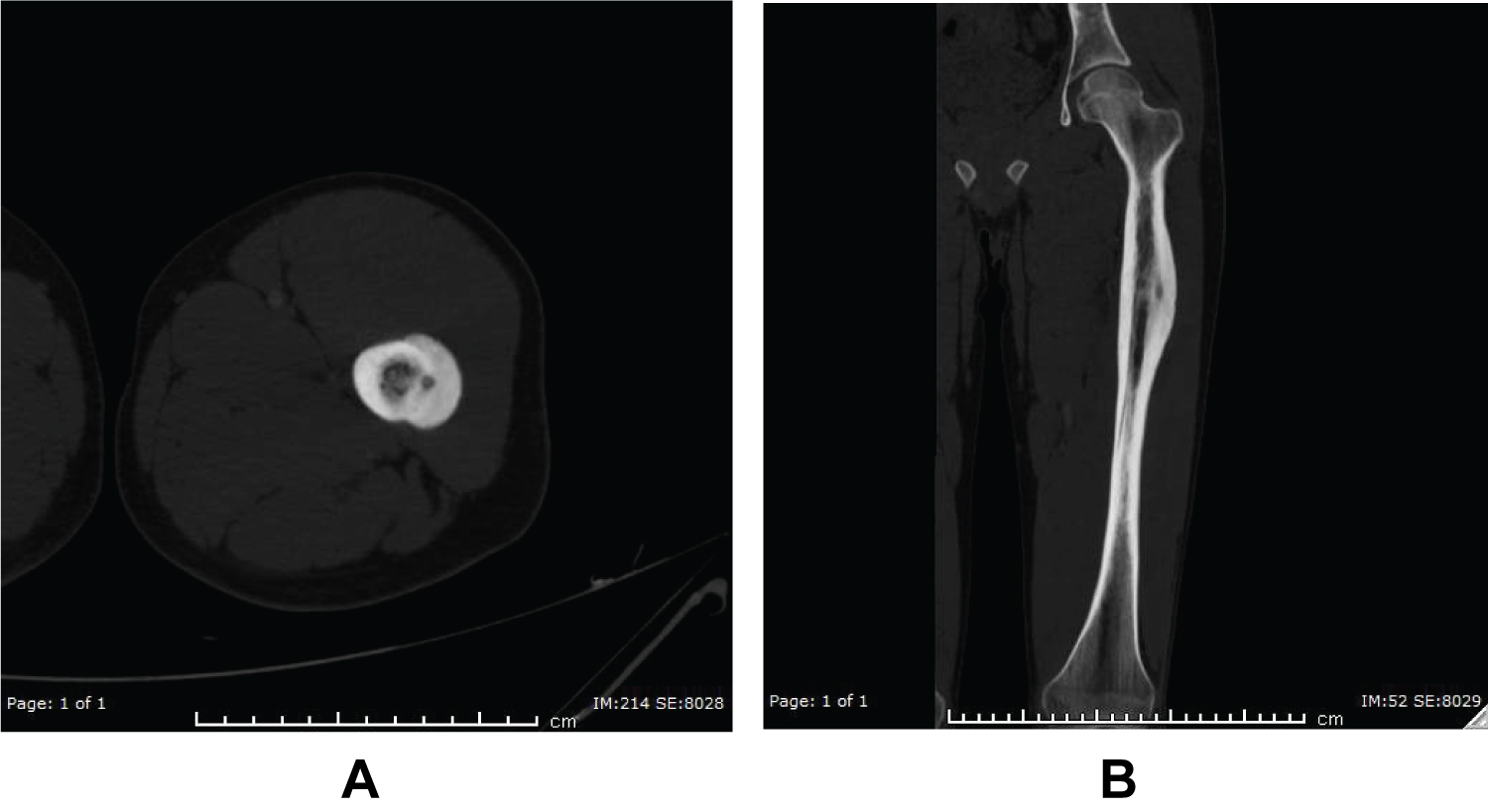 Figure 5: Osteoid osteoma in a 19-years-old male: (a) axial and (b) coronal CT images showing cortical sclerotic lesion with lucent nidus located at left femur.
View Figure 5
Figure 5: Osteoid osteoma in a 19-years-old male: (a) axial and (b) coronal CT images showing cortical sclerotic lesion with lucent nidus located at left femur.
View Figure 5
Lesions like aneurysmal bone cyst and fibrous dysplasia were rarely encountered and were not included into the study for statistical purposes.
Knowledge of the properties of benign bone lesions is important. Because they are rarely seen, the diagnosis may be delayed. The incidence of benign bone tumors and tumor-like lesions varies depending on the type.
Benign bone tumours and tumor-like lesions are most frequently seen in children and young adults, although they may also present in later stages of life [7]. The mean ages of the patients in this study also had shown that benign bone tumors are more frequent in the younger population.
Common benign bone tumors include osteochondroma, endochondroma and osteoid osteoma where as common tumor-like lesions include non-ossified fibroma, simple bone cyst, and fibrous dysplasia [15]. The most common benign bone tumor is osteochondroma [16]. In this study, the most frequent lesion was found as osteochondroma consisted with literature.
Although plain radiography is essential for diagnosis, CT and MRI examinations provide additional information [17]. Epidemiologic studies also have contribution in differential diagnosis and management of benign bone lesions. Treatment is indicated for symptomatic patients and for the patients with a risk of pathological fracture or deformity [18].
In conclusion our findings were overall consistent with the literature.