Rupture of the urinary collecting system is an unusual condition caused by a variety of causes, with obstructive ureteric calculi being the most common cause. The diagnosis is often delayed due to fact that it is rarely seen in daily practice and patients exhibit non-specific symptomatology at the time of presentation. Contrast-enhanced computed tomography usually confirms the diagnosis when contrast extravasations are seen in the excretory phase. Establishing an early diagnosis is crucial to avoid several serious complications such as urinoma, abscess formation, urosepsis, and renal impairment. Herein, we report a case of spontaneous renal calyceal rupture secondary to ureteric stricture.
Kidney, Calyceal rupture, Computed tomography, Radiology, Urography
Rupture of the collecting system can be due to traumatic or non-traumatic causes. It can occur anywhere along the urinary tract; however, the commonest site is at the renal calyces [1]. Non-traumatic calyceal rupture is also known as spontaneous calyceal rupture and is an unusual complication of obstructive uropathy that is much more common than the traumatic subtype. The most frequent obstructive causes include ureteric calculi, stricture, or tumor [2]. An obstructive ureteric calculus is considered the most common cause. Other reported rare etiologies include benign or malignant extrinsic ureteric compression, pregnancy, posterior urethral valve, pelvic-ureteric junction obstruction, and vascular extrinsic compression, iatrogenic and intravenous fluid administration [3]. Obstruction increases ureteric intraluminal pressure with subsequent forniceal or calyceal rupture and urine extravasations into the perirenal space and retro-peritoneum.
The diagnosis is often delayed as it is rarely seen in daily practice, in addition to the non-specific symptoms and clinical presentation. The diagnosis can be easily made using computed tomography [CT] when contrast extravasations are seen on the delayed excretory phase, which confirms the rupture [4]. Establishing an early diagnosis is crucial to avoid several serious complications such as urinoma, abscess formation, urosepsis, and renal impairment [4]. Here, we aimed to present a rare case of spontaneous calyceal rupture secondary to a proximal ureteric stricture in a patient with no clinical history of renal stones. Review of literature, diagnostic, and therapeutic approaches are further discussed.
A 56-year-old female patient with a clinical history of diabetes mellitus, hypertension, and dyslipidemia presented to the emergency department in our hospital with a 1-day history of abdominal pain at the left lower quadrant. She had sudden, continuous and non-radiating pain with seven episodes of non-bilious vomiting and watery diarrhea. She denied any history of trauma, renal colic, or passage of urinary stones. Upon physical examination, she was drowsy, tachycardia, and febrile. Her abdomen was tender on palpation at the left lower quadrant. Per-rectum examination was unremarkable. Laboratory investigation confirmed the diagnosis of urosepsis as the patient had raised white blood cell [WBC] count, inflammatory markers, metabolic acidosis, and positive urine analysis.
CT of the abdomen and pelvis with IV and rectal contrast was obtained to rule out left colonic diverticulitis, pyelonephritis, or urinary system calculi. The CT findings revealed a focal area of reduced parenchymal enhancement involving the posterolateral part of the middle zone of the left kidney, suggesting focal pyelonephritis with mild dilatation of the left pelvicalyceal system and proximal ureter (Figure 1). There were no obstructing ureteric stones; however, there was abnormal focal wall thickening, and enhancement of the middle 1/3 of the left ureter. The distal part of the left ureter was normal in caliber. There was also moderate amount of left-sided retroperitoneal non-loculated fluid collection associated with marked left perinephric fat stranding and thickening of the peri-renal fascia (Figure 1). The aforementioned findings raised the suspicion of a urinary collecting system or ureteric rupture with a subsequent retroperitoneal collection.
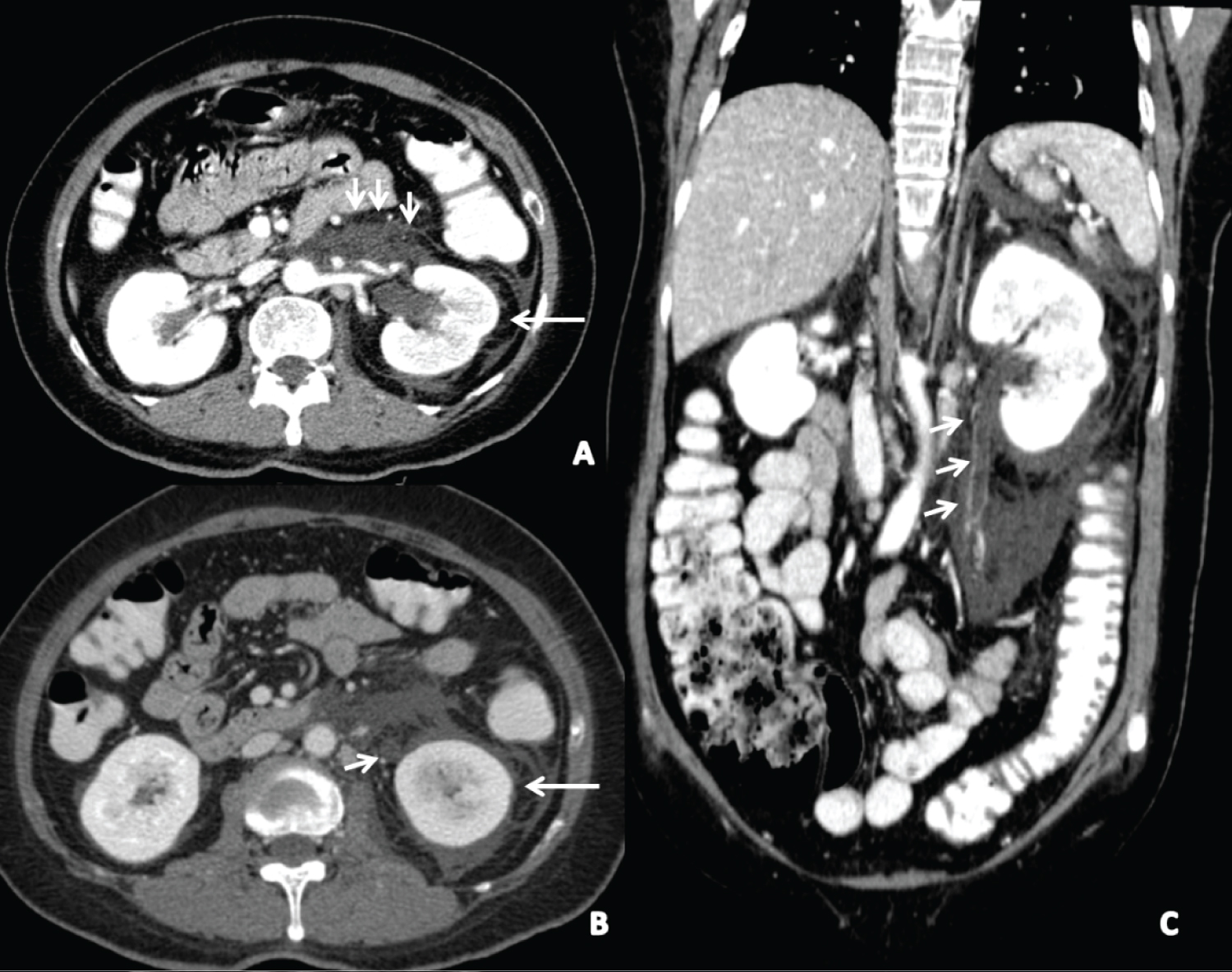 Figure 1: Axial (a,b) and coronal (c) multi-planner reconstruction (MPR) CT images showed a focal area of reduced left renal parenchymal enhancement with mild dilatation of the left pelvicalyceal system (arrows) and proximal ureter (short arrow, b). Noted mid ureteric stricture (arrows, c) and left perirenal fluid (arrows, a), without evidence of a stone.
View Figure 1
Figure 1: Axial (a,b) and coronal (c) multi-planner reconstruction (MPR) CT images showed a focal area of reduced left renal parenchymal enhancement with mild dilatation of the left pelvicalyceal system (arrows) and proximal ureter (short arrow, b). Noted mid ureteric stricture (arrows, c) and left perirenal fluid (arrows, a), without evidence of a stone.
View Figure 1
The case was discussed between the surgical and urology team who agreed to do a follow-up CT urography to further evaluate the urinary system in the excretory phase. Meanwhile, the patient was admitted to the intensive care unit (ICU) and managed conservatively until a second CT urography was performed 4 days later after the suppression of patient's sepsis with systemic antibiotic therapy. This showed bilateral pleural effusion, increased left retroperitoneal fluid, contrast extravasations from the anterior mid-pole of the left kidney during the excretory phase with mild hydronephrosis and proximal hydroureter down to the middle third of the left ureter where a focal segment of abnormal wall enhancement and small intraluminal non enhanced filling defect was seen (Figure 2). CT features confirmed the diagnosis of left renal calyceal rupture with focal acute pyelonephritis.
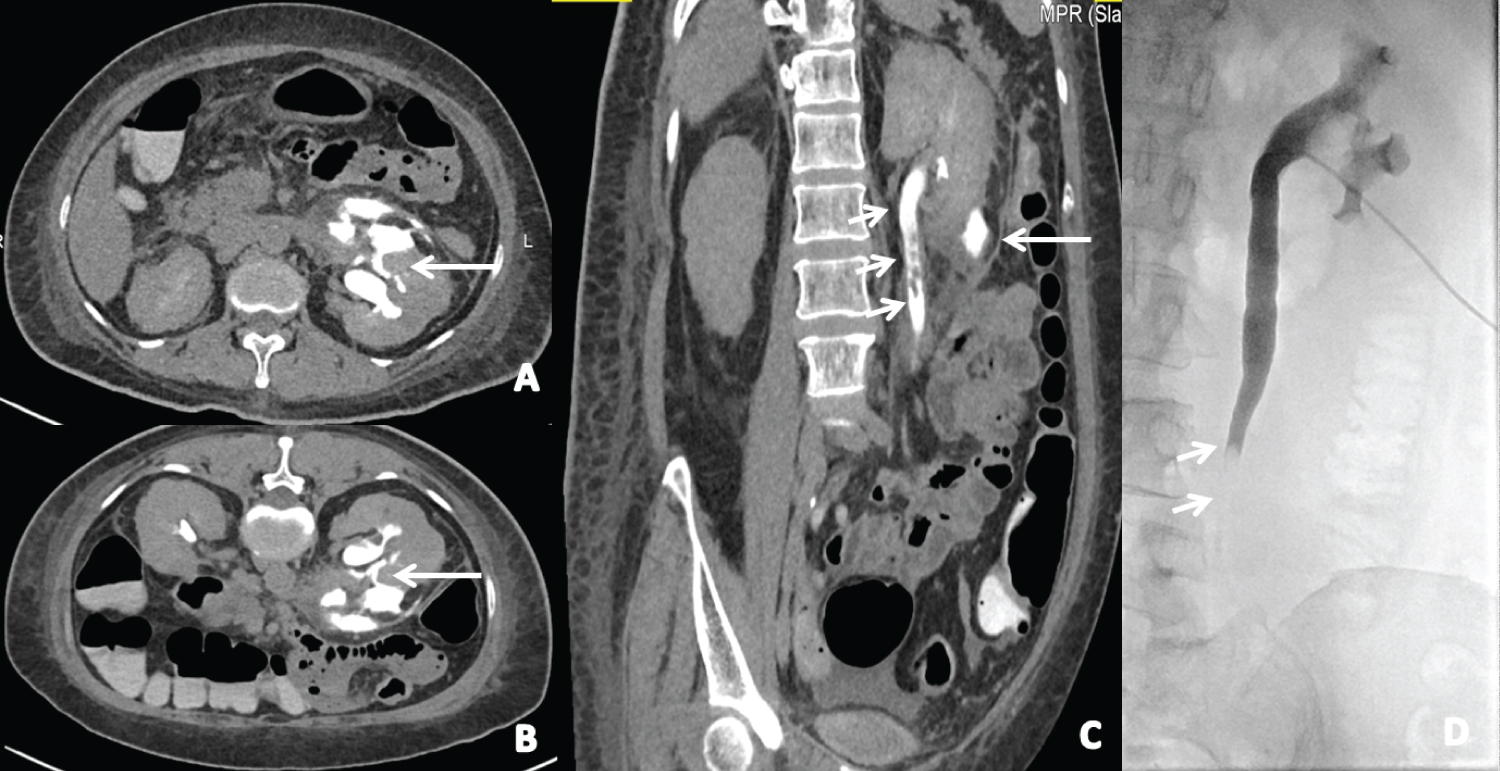 Figure 2: Axial supine (a) and prone (b), coronal multi-planner reconstruction (MPR) (c) delayed phase images show contrast extravasation from the anterior mid pole of the left kidney (arrows in a,b,c). Again noted mild hydroureteronephrosis down to the middle third left ureter with small intraluminal non-enhanced filling defects (short arrows in c). Antegrade pyelography (d) confirmed the mid-ureteric stricture with the related filling defect (arrows in d).
View Figure 2
Figure 2: Axial supine (a) and prone (b), coronal multi-planner reconstruction (MPR) (c) delayed phase images show contrast extravasation from the anterior mid pole of the left kidney (arrows in a,b,c). Again noted mild hydroureteronephrosis down to the middle third left ureter with small intraluminal non-enhanced filling defects (short arrows in c). Antegrade pyelography (d) confirmed the mid-ureteric stricture with the related filling defect (arrows in d).
View Figure 2
A percutaneous nephrostomy tube and double J ureteric stent were inserted. During the procedure, an ante grade pyelography was done and confirmed the mid-ureteric stricture with related filling defect (Figure 2d). Following nephrostomy insertion and medical treatment of sepsis, the patient improved clinically and was shifted from the ICU to the regular ward. One-week later, the nephrostomy tube was removed and the patient responded well to the treatment plan. A follow-up ultrasound showed marked regression of retroperitoneal fluid collection and regression of left-sided backpressure changes. The patient was discharged two weeks later in a stable condition with the ureteric stent in place under urology follow-up.
The clinical presentation of spontaneous calyceal rupture is diverse, ranging from mild flank pain to unremitting abdominal pain that is seen in patients with acute abdomen. The symptoms are often indistinguishable from simple renal colic [5].
In unilateral ureteric obstruction, the intra-renal collecting system pressure increases and leads to urine backflow as a compensatory mechanism. Furthermore, the obstruction reduces renal blood flow due to increased renovascular resistance with a subsequent reduction in diastolic blood flow velocity and elevation of the renal resistive index. The result would be decreased urine production in case of chronic ureteric obstruction. However, in acute ureteric obstruction, there will be further production of urine that adds more to the intra-renal collecting system resulting in calyceal rupture. This phenomenon is mainly seen in cases of obstructing ureteric stones due to the sudden increase in intra-renal collecting pressure before it accommodates this sharp alteration in intra-pelvis pressure [6].
According to most of the literature, the management of calyceal rupture is conservative and involves the administration of antibiotics to prevent urinary tract infection [4,6]. However, the treatment depends mainly upon the underlying cause of urinary tract rupture. A ureteric stent is used for calyceal rupture caused by an obstructive stone in the ureteropelvic junction or proximal ureter. Middle or distal obstructive ureteric stones can also provoke calyceal rupture and may be treated by ureteroscopic lithotripsy along with a ureteric stent [4,7,8].
Diagnostic imaging modalities for calyceal rupture such as ultrasound can detect hydronephrosis and fluid extravasations. Intravenous urography is found to be very sensitive and specific to confirm the diagnosis of urinary tract rupture. However, it can provoke urine extravasations due to the diuretic effect of the injected contrast media. Therefore, it is proposed to eliminate it as a first line diagnostic investigation. Contrast-enhanced CT of the abdomen and pelvis with delayed excretory imaging is found to be the best imaging modality in such patients as it can make the differential diagnosis of acute abdomen and obtain more information about the site of rupture, size, and location of the urinoma. In our case, the diagnosis is initiated by ultrasound and confirmed by contrast-enhanced CT with excretory phase. Since we didn't include the delayed phase imaging in the first CT scan, we were delayed in reaching the final diagnosis. Therefore, delayed excretory phase imaging of CT abdomen should be included in all cases with retroperitoneal collection to confirm or exclude the diagnosis of urinary tract rupture.
Spontaneous urinary tract rupture should always be considered in the differential diagnosis in a patient with vague abdominal symptoms and retroperitoneal fluid. The diagnosis can be easily made by CT urography which confirms the rupture decisively. Conservative treatment or minimally invasive procedures usually yield the best outcomes.
The authors declare that they have no conflict of interest.
This case report received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.