Trochlear dysplasia is characterized by abnormal trochlear morphology and a shallow groove and is known to be a major risk factor for patellofemoral instability. About 96% of patients with a history of a true patellar dislocation had evidence of trochlear dysplasia.
This study included 100 patients, their ages range between 12-60 years. All presented with anterior knee pain and had MRI examination after orthopedic consultation.
In this study, trochlear dysplasia is diagnosed in 16 patients among other knee disorders. Trochlear dysplasia type A is found in 6 patients, type B in 6 patients, and type C in 4 patients. Trochlear groove depth by (mm), trochlear facet asymmetry by (%) and lateral inclination angle by degree (°) were calculated for all trochlear dysplasia cases.
Different parameters can be used for MRI evaluation of the trochlear dysplasia, lateral trochlea inclination as the highest rated measurement. Trochlear depth and trochlear facet asymmetry were also used.
Trochlear dysplasia, Knee MRI, Patellar instability
Trochlear dysplasia is characterized by abnormal trochlear morphology and a shallow groove and is known to be a major risk factor for patellofemoral instability. Trochlear dysplasia typically is referred to as an unstable kneecap, the trochlea is not shaped normally, and the patella does not have the normal bony constraints to provide stability. About 96% of patients with a history of a true patellar dislocation had evidence of trochlear dysplasia [1]. Many measurements describing trochlear dysplasia have been developed and presented, and there is no consensus concerning which measurements should be used to diagnose trochlear dysplasia or guide its treatment. Some authors characterize trochlear dysplasia using the following measurements: lateral condyle index, lateral trochlear inclination and trochlear facet asymmetry [2]. Others use only the Dejour classification or a modified. Dejour classification to describe trochlear dysplasia, and some use the lateral trochlear inclination as the only measure to discriminate dysplastic knees from healthy knees [3,4].
This study included 100 patients, their ages range between 12-60 years. All presented with anterior knee pain and had MRI examination after orthopedic consultation. Plain X-ray of the affected knee joint was also performed. The study excluded patients with absolute contraindications to MRI examination. Present and past medical histories were taken. Patients were positioned supine with the affected knee completely or nearly completely extended in the knee coil. MRI was performed by using knee coil for all patients. Patients had MRI examination of the affected knee joints on high field-strength scanners using Philips Scannres Achieva or Intera (1.5 T). Matrix size 256/192 or 512/224. Field of view ranged from 12 to 16 cm. Slice thickness 4 mm. Slice gap 4 mm. The average duration time of the examination ranged from 25-30 minutes.
This study included 100 patients complaining of anterior knee pain, with their ages ranged between 12-60 years. The descriptive statistics for age of the patients are 26.76 ± 10.00.
In this study, trochlear dysplasia is diagnosed in 16 patients among other knee disorders (Table 1).
Table 1: Demonstrates the prevalence of trochlear dysplasia among the patients in the study sample. View Table 1
In this study, trochlear dysplasia type A is found in 6 patients, type B in 6 patients, and type C in 4 patients (Figure 1). Trochlear groove depth by (mm), trochlear facet asymmetry (Figure 2) by percentage (%) and lateral inclination angle by degree (°) were calculated for all trochlear dysplasia cases as shown in Table 2.
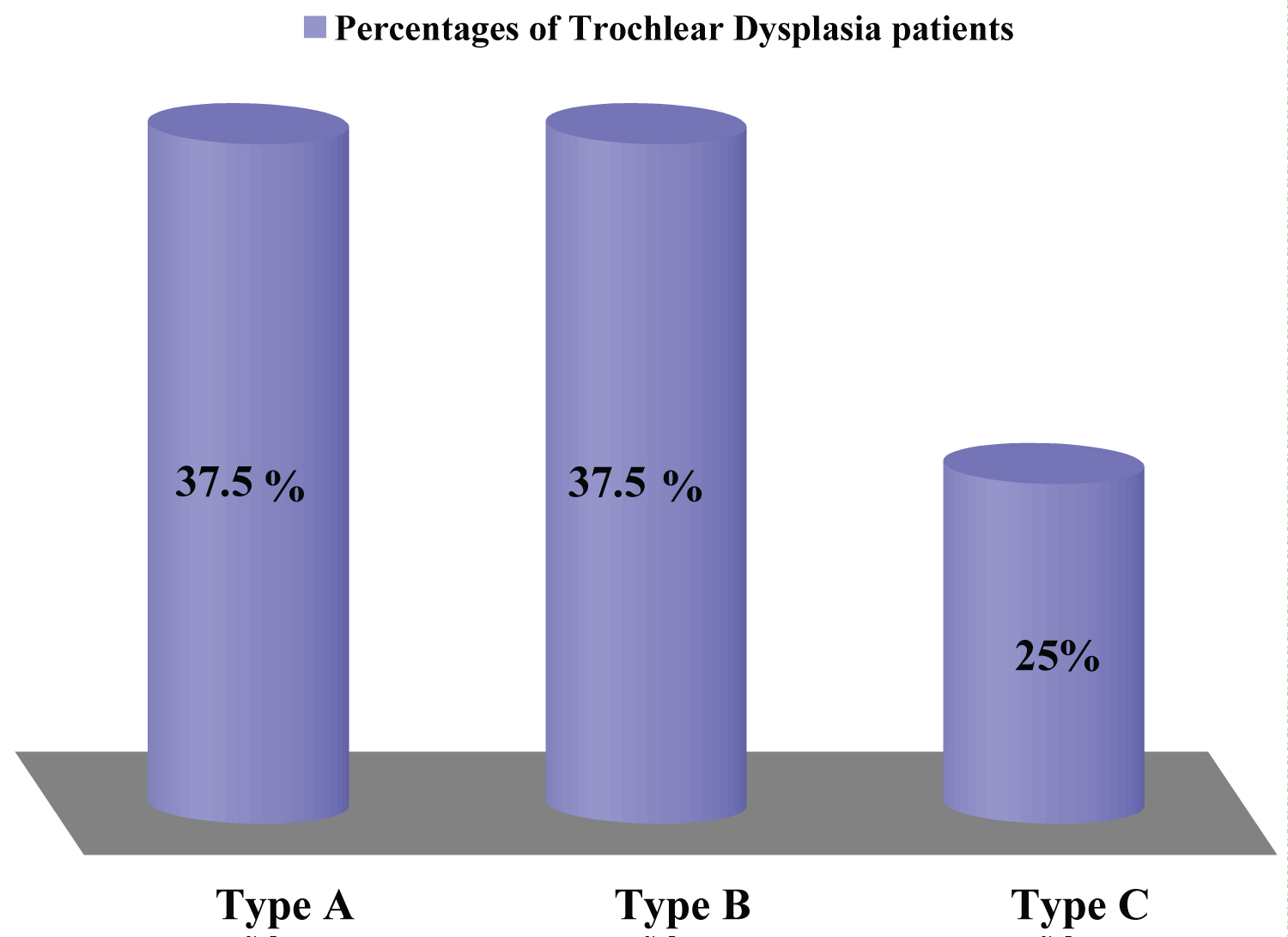 Figure 1: Demonstrates percentages of different grades of Trochlear dysplasia among the patients with patellar instability.
View Figure 1
Figure 1: Demonstrates percentages of different grades of Trochlear dysplasia among the patients with patellar instability.
View Figure 1
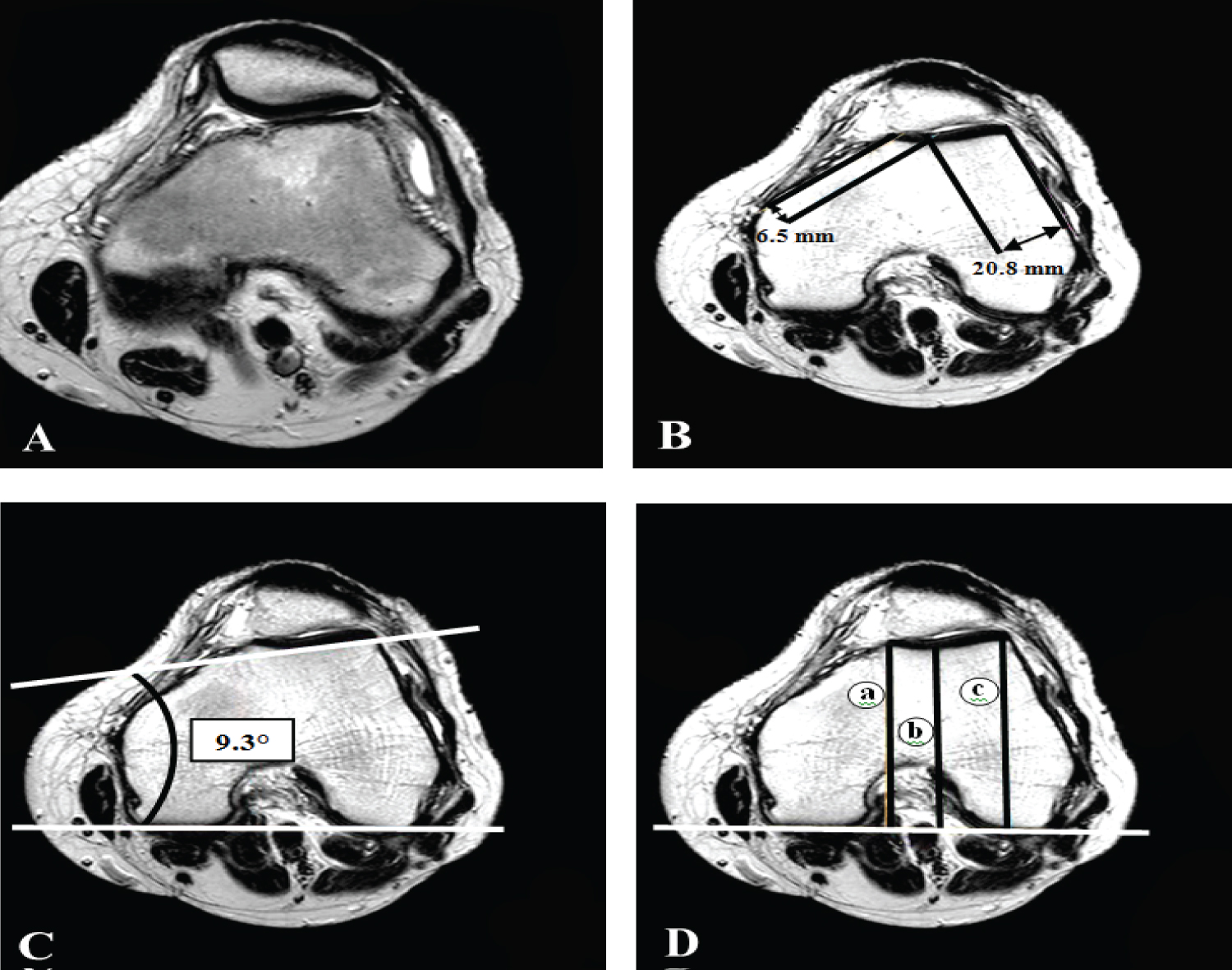 Figure 2: Axial T2 weighted images shows, A) Loss of contact between the patellofemoral joint surfaces laterally. B) Trochlear facet asymmetry 32% (normally not less than 40%), C) Lateral inclination angle 9.3° (normally not less than 11°), and D) Trochlear depth 1.7 mm (normally up to 3 mm), where a = 66.1 mm, b = 65.3 mm and c = 67.9 mm.
View Figure 2
Figure 2: Axial T2 weighted images shows, A) Loss of contact between the patellofemoral joint surfaces laterally. B) Trochlear facet asymmetry 32% (normally not less than 40%), C) Lateral inclination angle 9.3° (normally not less than 11°), and D) Trochlear depth 1.7 mm (normally up to 3 mm), where a = 66.1 mm, b = 65.3 mm and c = 67.9 mm.
View Figure 2
Table 2: Demonstrates the statistically calculated minimum, maximum, median and mean values of trochlear groove depth by (mm), trochlear facet asymmetry by (%) and lateral inclination angle by (°). View Table 2
In individuals with Trochlear Dysplasia, D Dejour's classification is used which include four types: Normal shape of the trochlea preserved but a shallow trochlear groove refer to Type A. Markedly flattened or even convex trochlea refer to Type B. Asymmetric trochlear facets, with the lateral facet being too high and the medial facet being hypoplastic, which results in the flattened joint surface forming an oblique plane refers to Type C. In addition to the features of type C, a vertical link between medial and lateral facets (cliff pattern on parasagittal images) refers to Type D.
In case of patellar maltracking, we measure the following different parameters for the evaluation of the trochlear dysplasia:
a) Lateral trochlear inclination (LTI), on the MR-slices at about 3 cm above the femorotibial joint space by measuring the angle between a line tangential to the subchondral bone of the posterior aspects of the femoral condyles and a line tangential to the subchondral bone of the lateral trochlear facet (Figure 3). An angle of < 11° is considered abnormal [5].
 Figure 3: Lateral trochlear inclination assessed on axial fat-saturated T2-weighted MR images. A line (arrow) is drawn along the subchondral bone of the lateral trochlear facet, and a second line (arrow head) is drawn along the posterior aspect of the femoral condyles. The angle between the two lines is the inclination angle (dashed line). An inclination angle of less than 11° indicates trochlear dysplasia.
View Figure 3
Figure 3: Lateral trochlear inclination assessed on axial fat-saturated T2-weighted MR images. A line (arrow) is drawn along the subchondral bone of the lateral trochlear facet, and a second line (arrow head) is drawn along the posterior aspect of the femoral condyles. The angle between the two lines is the inclination angle (dashed line). An inclination angle of less than 11° indicates trochlear dysplasia.
View Figure 3
b) Trochlear facet asymmetry, MRI slices at about 3 cm above the tibiofemoral joint space were use. Trochlear facet asymmetry was expressed with the relation of medial trochlear facet width (e) to lateral trochlear facet width e/f × 100%. A ratio of less than 0.4 is considered abnormal which means that the medial facet is less than 40% the width of the lateral one (Figure 4) [6].
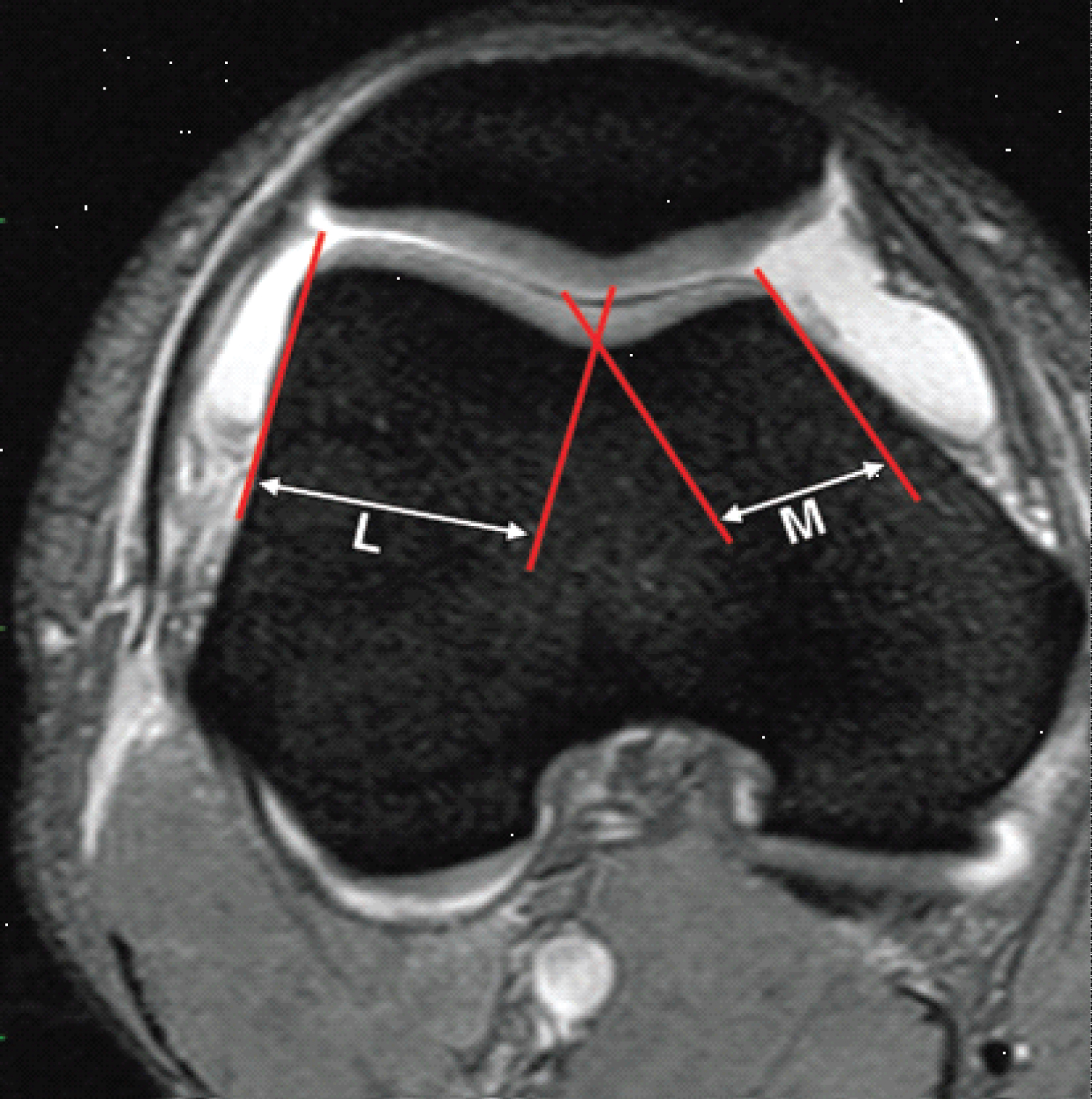 Figure 4: Trochlear facet asymmetry assessed on axial fat-saturated T2-weighted MR images. Asymmetry of the medial facet length (M) and the lateral facet length (L) is calculated as the ratio of the medial facet length divided by the lateral facet length expressed as a percentage (M/L × 100%). A trochlear facet ratio of less than 40% indicates dysplasia.
View Figure 4
Figure 4: Trochlear facet asymmetry assessed on axial fat-saturated T2-weighted MR images. Asymmetry of the medial facet length (M) and the lateral facet length (L) is calculated as the ratio of the medial facet length divided by the lateral facet length expressed as a percentage (M/L × 100%). A trochlear facet ratio of less than 40% indicates dysplasia.
View Figure 4
c) Depth of the trochlear groove, MRI slices at about 3 cm above the tibio-femoral joint space were used for the assessment of the trochlear depth by measuring the maximal antero-posterior distance of the medial femoral condyle (distance a) and lateral femoral condyle (distance b), and the minimal antero-posterior distance between the deepest point of the trochlear groove and the line paralleling the posterior outlines of the femoral condyles (distance c) (Figure 5). Trochlear depth was calculated by the formula ([a + b]/2)-c). Trochlear dysplasia is assumed if the trochlear depth is 3 mm or less [7].
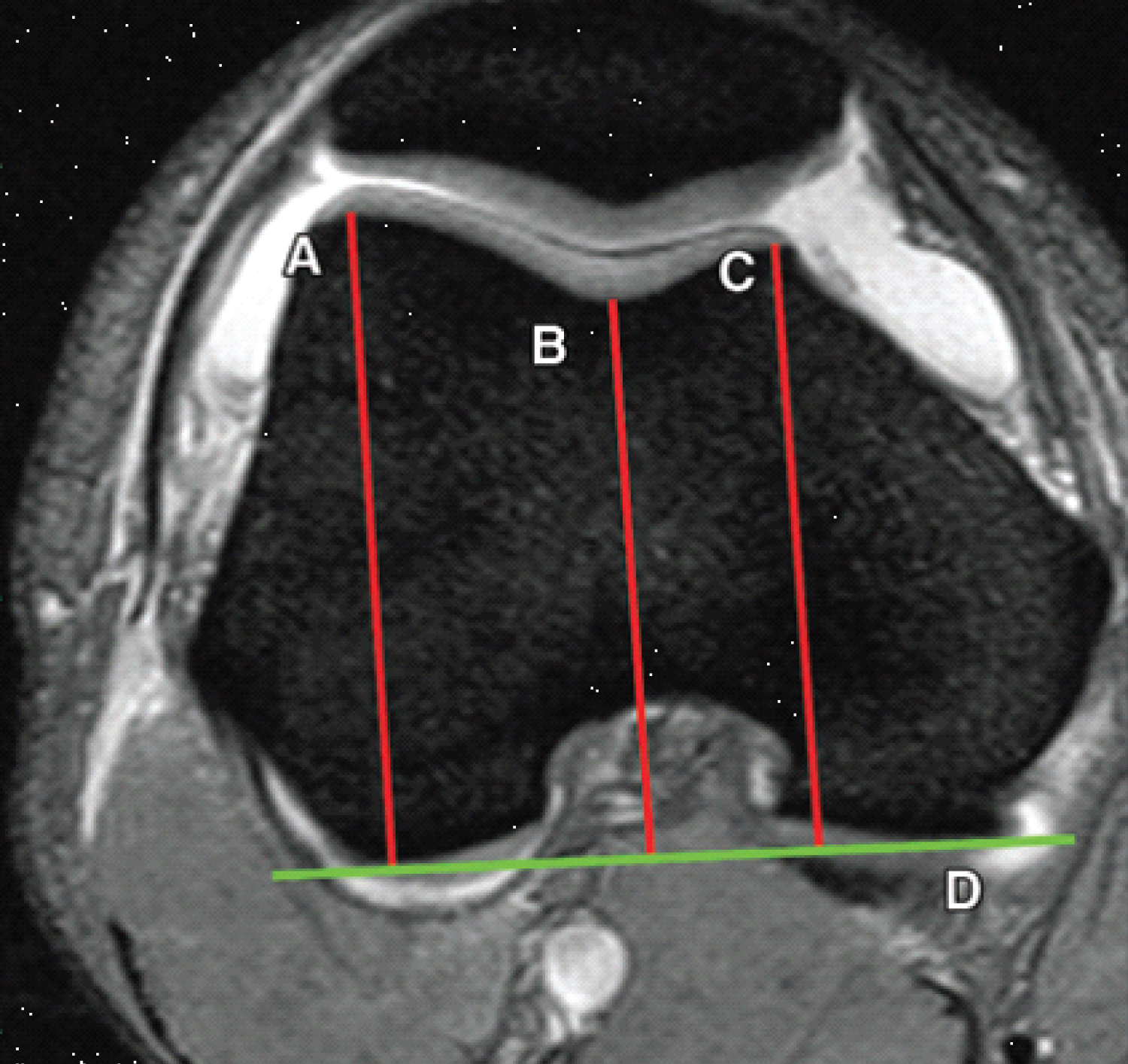 Figure 5: Trochlear depth assessed on axial fat-saturated T2-weighted MR images. A line drawn parallel to the posterior aspect of the femoral condyles serves as a reference line (line D). The lines drawn perpendicular to the reference line indicates the largest anteroposterior diameters of the lateral (line A) and medial (line C) trochlear facets and the deepest point of the sulcus (line B). Trochlear depth is calculated as follows: (A + C/2) - B). A trochlear depth of 3 mm or less is assumed to indicate dysplasia.
View Figure 5
Figure 5: Trochlear depth assessed on axial fat-saturated T2-weighted MR images. A line drawn parallel to the posterior aspect of the femoral condyles serves as a reference line (line D). The lines drawn perpendicular to the reference line indicates the largest anteroposterior diameters of the lateral (line A) and medial (line C) trochlear facets and the deepest point of the sulcus (line B). Trochlear depth is calculated as follows: (A + C/2) - B). A trochlear depth of 3 mm or less is assumed to indicate dysplasia.
View Figure 5
The study establishes that 16% of the patients had patellofemoral pain with misalignment showing MRI evidence of trochlear dysplasia. 40% categorized as type A, 40% as type B, and 20% as type C according to Dejour, et al. classification. Dejour and Le Coultre (2007) reported that the trochlear dysplasia type A represent 54%, type B 17%, and type C 9% [8].
Diederichs, Issever and Scheffler (2010) [7] mentioned that techniques for quantifying the degree of dysplasia have been standardized for MR imaging. Trochlear dyspla¬sia can be evaluated at MR imaging by determin¬ing lateral trochlear inclination, trochlear facet asymmetry, or trochlear depth. Diederichs, Issever and Scheffler (2010) [7] reported that the threshold for trochlear dysplasia is an inclina¬tion angle of 11°, with an inclination angle of less than 11° indicating trochlear dysplasia. Pfirrmann, et al. [6] calculated the depth of the trochlear groove and trochlear facet asymmetry 3 cm above the femorotibial joint. They found that trochlear groove depth less than 3 mm and facet asymmetry of less than 40% are diagnostic value for trochlear dysplasia. The study establish that all patients with trochlear dysplasia, 50% had lateral trochlear inclination of less than 11°, 25% had trochlear groove depth of less than 3 mm and 25% had facet asymmetry of less than 40%.
Different parameters can be used for MRI evaluation of the trochlear dysplasia, lateral trochlea inclination as the highest rated measurement. Trochlear depth and trochlear facet asymmetry were also used.
All patients included in this research gave written informed consent to publish the data contained within this study.
The authors declare that they have no competing interests.
Not applicable.
RHM collected, analyzed and interpreted the patient images and patient's information as well as pathological results; HAS suggest the idea, shares in collection, analysis and interpretation of the patient images; MJM supervises and manuscript preparation. All authors read and approved the final manuscript.
Not applicable.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
All study procedures were carried out in accordance with the Declaration of Helsinki regarding research involving human subjects. The committee's reference number is not available at this time. All patients included in this research gave written consent to participate in this research.