• A 45-year-old man with a history of an operation on the meniscus of the left knee, consulted for loss of full range of motion, tenderness along the joint line and discomfort while walking regarding the left knee.
• An anterior cruciate ligament rupture is suspected and an MRI has been performed.
MRI showed poorly limited soft tissue nodule in the intercodylar notch near the tibial insertion of the anterior cruciate ligament (ACL) (Figure 1) and extended to hoffa's fat bundle. This lesion showed predominantly heterogeneous signal intensity on T2-weighted and proton-density images.
 Figure 1: Sagittal proton-density fat-suppressed image shows poorly limited soft tissue nodule in the intercodylar notch near the tibial insertion of the anterior cruciate ligament (ACL) and extended to hoffa's fat bundle (black arrow), she also shows the absence of lateral meniscus (red arrow).
View Figure 1
Figure 1: Sagittal proton-density fat-suppressed image shows poorly limited soft tissue nodule in the intercodylar notch near the tibial insertion of the anterior cruciate ligament (ACL) and extended to hoffa's fat bundle (black arrow), she also shows the absence of lateral meniscus (red arrow).
View Figure 1
Absence of lateral meniscus probably related to meniscectomy (Figure 1).
Abnormal anterior cruciate ligament orientation relative to intercondylar (Blumensaat's) line evocative of complete tear of anterior cruciate ligament (Figure 2, Figure 3 and Figure 4).
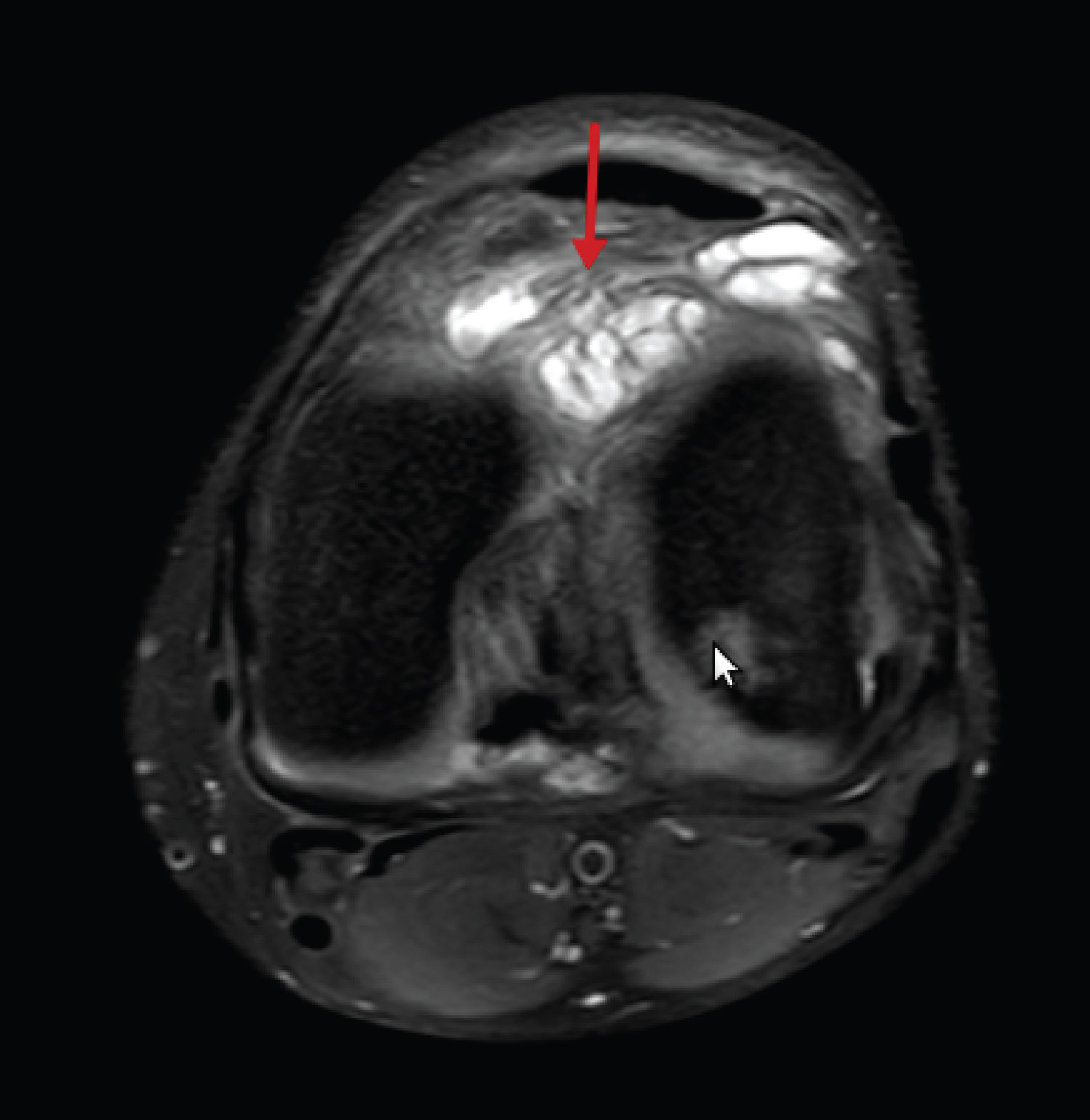 Figure 2: Axial proton-density fat-suppressed image shows heterogeneous cyclops nodule (arrow) in the intercondylar notch.
View Figure 2
Figure 2: Axial proton-density fat-suppressed image shows heterogeneous cyclops nodule (arrow) in the intercondylar notch.
View Figure 2
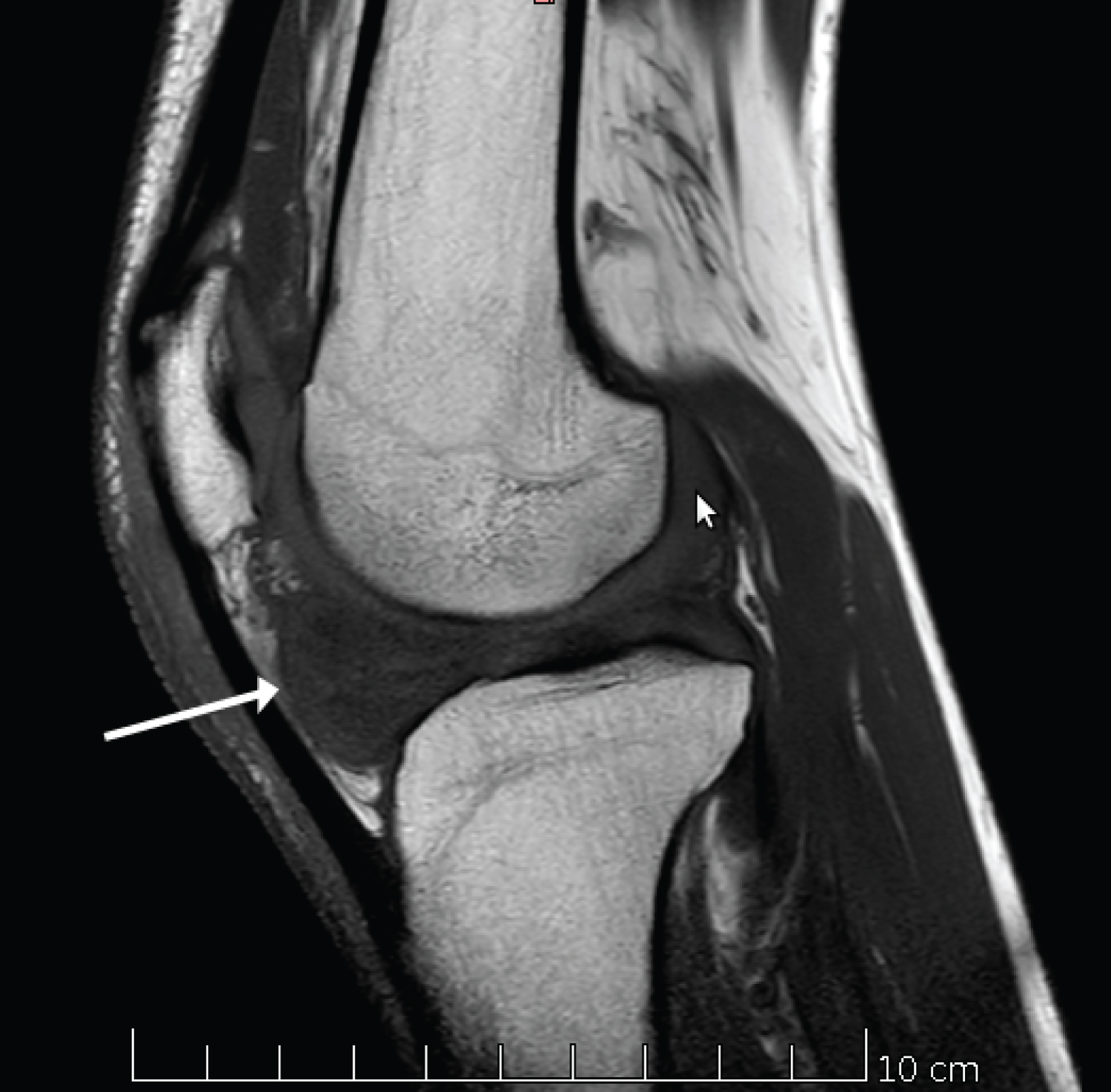 Figure 3: Sagittal T1-weighted image through the intercondylar notch shows a cyclops nodule (arrow) with isosignal intensity to skeletal muscle.
View Figure 3
Figure 3: Sagittal T1-weighted image through the intercondylar notch shows a cyclops nodule (arrow) with isosignal intensity to skeletal muscle.
View Figure 3
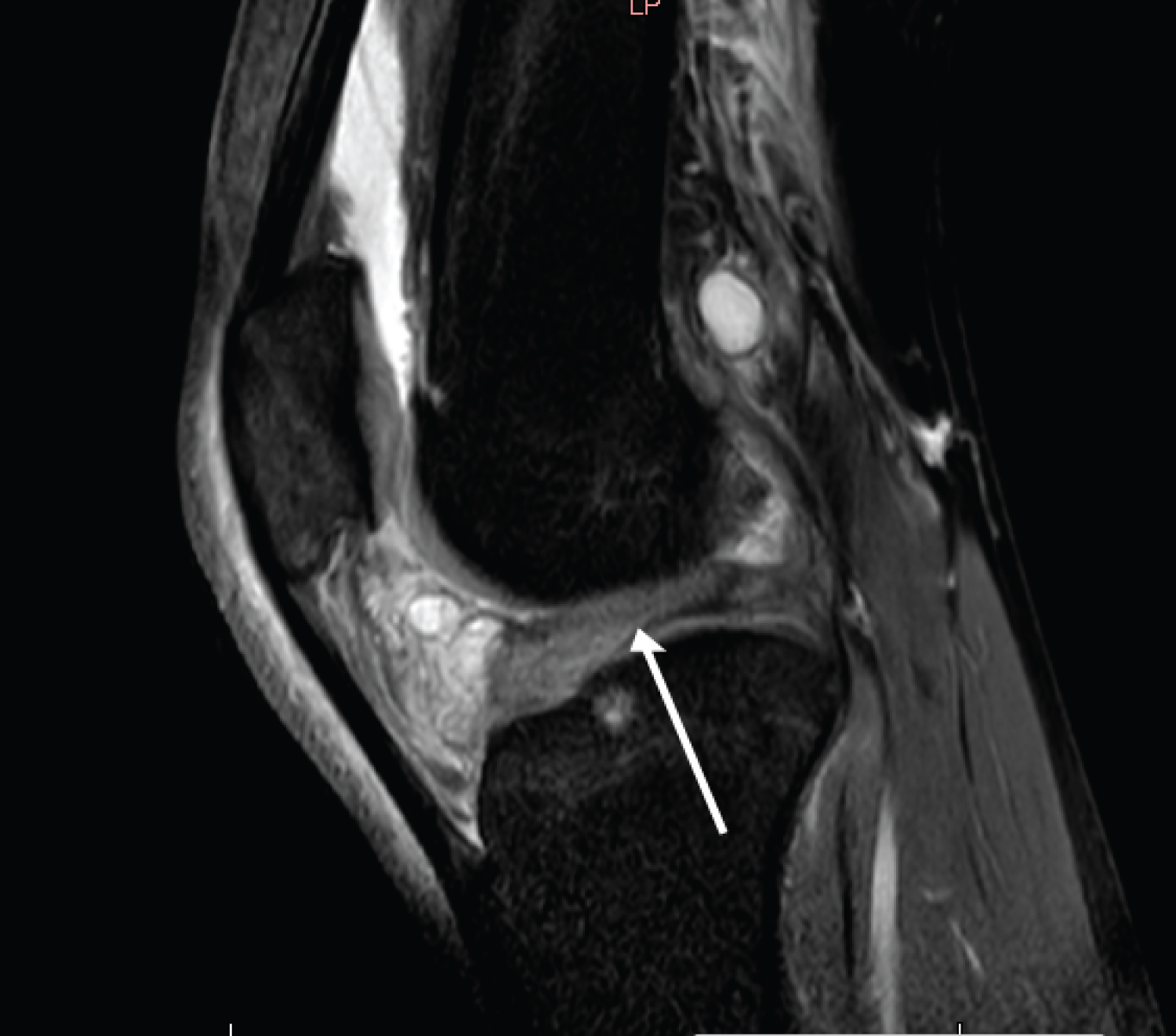 Figure 4: Sagittal proton-density fat-suppressed image shows complete tear of the ACL (arrow) with abnormal anterior cruciate ligament orientation (arrow) relative to intercondylar (Blumensaat's) line.
View Figure 4
Figure 4: Sagittal proton-density fat-suppressed image shows complete tear of the ACL (arrow) with abnormal anterior cruciate ligament orientation (arrow) relative to intercondylar (Blumensaat's) line.
View Figure 4
A. Localized anterior fibrosis (cyclops lesion) is a known cause of extension loss of the knee after anterior cruciate ligament (ACL) reconstruction [1], Although the original description of cyclops syndrome was in patients who had undergone ACL reconstruction, more recent reports have documented its occurrence after ACL injury or meniscectomy in the absence of ACL reconstruction [2]. The exact etiology is uncertain and may be related to gradual fraying and bunching up of remnant ACL or graft fibers, excessive fibrosis.
B. Patients often present with loss of terminal extension of the knee, discomfort on walking or running or when lying supine, and an audible or palpable clunk during terminal extension [3]. MRI has sensitivity, specificity, and accuracy of 85.0%, 84.6%, and 84.8%, respectively, for diagnosing cyclops lesions [1].
C. The imaging morphology of a soft-tissue mass in the intercondylar notch (Figure 3) near the tibial insertion of the anterior cruciate ligament that causes loss of extension is, by definition, a cyclops nodule and is similar in subsets of patient who have undergone ACL reconstruction and those who have not [2].
D. The general consensus is to leave asymptomatic cyclops lesions undisturbed, whereas cyclops syndrome requires intervention to recover the normal biomechanics of the knee [3]. The prognosis is good with these lesions after excision. The symptoms completely resolve within a few weeks after excision of the lesion [4].
E. Localized anterior arthrofibrosis should be suspected in any patient in whom an ACL nodule is identified at MR imaging, and surgical excision is the management of choice for symptomatic lesions.
Localized anterior arthrofibrosis of the knee.
Nodular synovitis, Cyclopoid scars, localized intraarticular giant cell tumor of the tendon sheath.