Our attention is focused on infants whose body image does not reflect signs of bad eating habits and thus escape pediatrician detection. Previously, in an experimental model under potentially atherogenic diet intake, despite no significant zoometric differences, we evidenced an inverse correlation between bone mineral density (BMD) by multi slice-quantitative computed tomography (MS-QCT) and serum total cholesterol (T-cho) after 3 weeks diet. In order to focus on long bone growth and development, our aim was set on endochondral ossification.
Determine if MS-QCT BMD loss triggered by an unhealthy high fat diet (HFD) intake established in infancy is related to bone growth in length, mediated by endochondral ossification.
Weanling male Wistar rats (n = 12), were divided in two groups, Control (C) and Experimental (E), with no differences in initial body weight (p > 0.05). Food and water offered in free demand and followed for 7 weeks (7w): C with rodent stock diet (RSD) and E with HFD: RSD with saturated fat and cholesterol added. During 7w zoometry, diet and water intake were monitored. Histomorphometry on digital microphotographs of tibiae longitudinal sections, H & E stained, included: bone volume (BV/TV%), divided in primary (BVA/TVA%) and secondary (BVB/TVB%) cancellous bone, and growth plate cartilage's thickness (GPC.Th) with hyperthrophic zone (HpZ.Th). Tibiae BMD by MS-QCT (Philips-64CT, HOROS/McIntosh) in Hounsfield Units (HU) of four tibial zones (TZ1-4): From plate towards metaphysis. Statistics: Student's t test and Pearson's correlation between BMD of TZ1-4 and T-cho. 5% probability considered significant.
There were no zoometric nor intake differences (p > 0.05) and serum lipid profile evidenced HFD's content (experimental model). Between E and C no significant histomorphometry differences (p > 0.05) encountered in bone volume nor in cartilage plate. BMD and T-cho correlation (r) was significantly relevant (p < 0.05) in all zones studied: TZ1: -0.8121; TZ2: -0.4691; TZ3: -0.6814; TZ4: -0.8175.
These endochondral ossification findings, taken together with BMD loss by MS-QCT, lead to think that the difference would be in the degree of mineralization of cancellous bone and not in its volume. From the present we can deduce that chronic intake of excess fat and cholesterol in diet during infancy may provoke a vulnerable bone in young adulthood that could be promptly detected by MS-QCT.
Bone mineral density, Quantitative computed tomography, Endochondral ossification, High fat diet
BMD: Bone Mineral Density; MS-QCT: Multi Slice-Quantitative Computed Tomography; HU: Hounsfield Units; HFD: High Fat Diet; RSD: Rodent Stock Diet; T-cho: Serum Total Cholesterol; H&E: Hematoxiline & Eosine; BV/TV%: Bone Volume as % of Total Volume; BVA/TVA%: Primary Cancellous Bone Volume as % of Total Primary Volume; BVB/TVB%: Secondary Cancellous Bone Volume as % of Total Secondary Volume GPC.Th: Growth Plate Cartilage'S Thickness; HpZ.Th: Hyperthrophic Zone of Growth Plate Cartilage
Diet is a main determinant of clinical manifestations that involve cardiovascular disease, increased blood pressure, cholesterol and overweight-obesity [1,2]. Cholesterol and fatty acid intake are still an important factor pointed out as reference in prevention and treatment of dyslipidemias. Saturated fatty acids are found in food of animal source, also in tropical oil, and are considered the principal component of diet that correlates well with cholesterol bound to low density lipoprotein (LDL-cho) levels. The amount of saturated fat depends on food origin [3].
Our attention is focused on those children that do not reveal body image signs of bad food intake habits, and hence escape pediatric detection. We knowledge that some fat types favor bone formation, as does vitamin E [4]; while others inhibit it, like LDL-minimally oxidized and other bioactive oxidized lipids [5]. This provides reason of interest to measure body fat composition and bone mineral content (BMC) during growth in order to determine future risk of osteoporosis and bone fracture.
Dual-energy X-ray absorptiometry (DXA) is actually the method mostly used to acquire bone mass in infants [6-8]. On the other hand, Quantitative Computed Tomography (QCT) can discriminate cancellous from cortical bone density in a real volume (3D), not as DXA that estimates it on a surface (2D). Actually, technology provides multi slice (MS) detectors that are precise evaluating changes in bone structure and density with low radiation dose [9].
The importance to evaluate bone mineral density (BMD) in different parts of human body during growth phases resides in biomechanics that influences each bone and deserves an individual and specific study; from formation to ossification in infancy, as also in devolvement and progressive ageing [9]. We have demonstrated that MS-QCT is an imaging diagnostic method that allows the early detection of mandible bone architecture alterations induced by a potentially atherogenic high fat diet (HFD) [10].
Taking into account the recommendations of the International Commission on Radiological Protection [11], exposure to radiation in population of our interest would not be pediatrician's choice as a routine check-up study. These ethical reasons make the use of a growing rat experimental model that parallels humans of particular importance, as previously reported by our group [12-14].
In preceding work, focused on mandible, in an experimental growing rat model fed with a potentially atherogenic HFD, despite no significant zoometric differences, we evidenced an inverse correlation between BMD by MS-QCT and serum total cholesterol (T-cho) after 3 weeks diet [10,15,16]. These findings, capture our group's interest on endochondral ossification under this diet. The present study was carried out to determine if MS-QCT BMD loss triggered by an unhealthy HFD intake established in infancy is related to bone growth in length, mediated by endochondral ossification. In order to do so, endochondral ossification was analyzed by two different procedures: MS-QCT for BMD and histomorphometry for bone volume and growth plate cartilage.
Twelve male weanling Wistar rats (age 21 ± 2 days), were randomly divided into two groups of 6 rats each: Control (C) and Experimental (E). Body weight (g) and length (cm) at initial time (t0) had no significant differences between groups (p > 0.05). They were fed ad-libitum during a 7 week (7w) experimental period. C received rodent stock diet (RSD) and E, a HFD. Water intake, at demand, was controlled at all times during the 7w of experiment. Animals were housed in galvanized cages with meshed floors to maintain hygienic conditions. They were exposed to a 12-h light, 12-h dark cycle. Room temperature was maintained at 21 ± 1 ℃ with a humidity of 50% to 60%. The protocols for these experiments follow the NIH (Res. 8023) guide-lines for care and keeping of experimental animals, stated in Ethics Code of our establishment that were approved by the University of Buenos Aires, Argentina (Res. CS 4081/04).
Control diet (C): RSD (Product SENASA N°:04-288/A. Manufactured by Asociación de Cooperativas Argentinas C.L. Nutrición Animal. San Nicolás, Buenos Aires, Argentina). Experimental diet (E): HFD pellets prepared with RSD adding saturated fat (16% gluten-free butter, Sancor®) and cholesterol (1% cholesterine, Parafarm®) as described in [10,15,16]. This diet was previously tested by our group, as we have developed an experimental growing rat model that parallels children and adolescents accustomed to a high saturated fat and cholesterol diet, but do not show signs of overweight or obesity [10,15,16]. The HFD has an additional metabolic energy (ME) of 915 K cal ME/kg diet, over C diet.
Measurements were performed after a fasting period of 2 to 4 hours. Body weight (Wt) determined in grams, every 3-4 days with a Mettler PC4000 scale of accuracy ± 1 mg. Body length at start (t0) and 7w, with a scaled ruler of accuracy ± 1 mm, from the nose tip to the hairline of the tail, were performed under general anesthesia by intraperitoneal injection of ketamine 40 mg/kg (Ketamina 50, Holliday-Scott S.A., Beccar, Buenos Aires, Argentina) and xylazine 5 mg/kg (Kensol König, Laboratorios König S.A., Avellaneda, Buenos Aires, Argentina).
Food cups were refilled 2 times each week, and food consumption was measured with a Mettler scale of accuracy ± 1 mg. Daily food intake was expressed as g of diet/100g of rat Wt/day. Water volume intake was controlled daily and also as percent of total rat Wt/day.
At 7w, blood was obtained by cardiac puncture for biochemical assays under general anesthesia (as described for zoometry), after which animals were euthanized by barbiturate overdose. Serum was removed and sent to determine lipid-lipoprotein profile (Faculty of Pharmacy & Biochemistry, INFIBIOC-UBA) (mg/dL): Total cholesterol (T- cho), triglycerides (TG), high density lipoprotein-cholesterol (HDL-cho), non-HDL-cholesterol (n-HDL-cho). By difference between T-cho and HDL-cho, n-HDL-cho is obtained and represents all atherogenic apo-B rich lipoproteins that are object of treatment in humans [17]. All methods were standardized and applied under strict internal and external quality controls. The evaluation was blind, since the technician did not know the experimental protocol. These serum results allowed to confirm that experimental diet was potentially atherogenic, being the basis of our experimental model [10,15,16].
Philips Brillance 64 CT equipment placed in "Sagrada Familia" Clinic (ENERI, Argentina) was used. Images obtained by Multi Slice-Quantitative Computed Tomography (MS-QCT) were analyzed with eFilm Workstation 2.1 program and measurements in Hounsfield units (HU) acquired bone density data based on QCT principles. The acquisition was made with the animal in prone position, locking of the legs and intraperitoneal anesthesia (0.5 mg Xylazine + 8.75 mg Ketamine/ 100 g rat Wt). At 7w an exploration of the whole body of each animal was achieved, using high resolution protocols adapted to small animals, standardized in preliminary studies [18]. Based on morphological and histological positioning that was to be compared [19] measurements were performed with the HOROS program under environment McIntosh, multiplanar review for drawings to display sagittal, coronal and axial positions, taking as reference tibial plate and placing a centered parallel to the cortical and a perpendicular intercondylar line as guides (Figure 1). In search for alignment of dishes, angles were used with a variation of ± 25°. Thickness was 0.45 mm and a ROI (Region of Interest) for the measurement of density of 0.5 mm2 area. In this way four tibial zones (TZ1-4) were defined, from the tibial plate towards the metaphysis (Figure 2). The tibial zones selected had to be standardized and aimed to survey from growth plate cartilage (TZ1) to the central area of subchondral bone, across primary and secondary cancellous bone (TZ2-4) to compare with histomorphometric parameters. Measurements were all carried out by one operator and verified by a second operator under the same environment HOROS. Each animal data resulted from the average of the measurements of both operators.
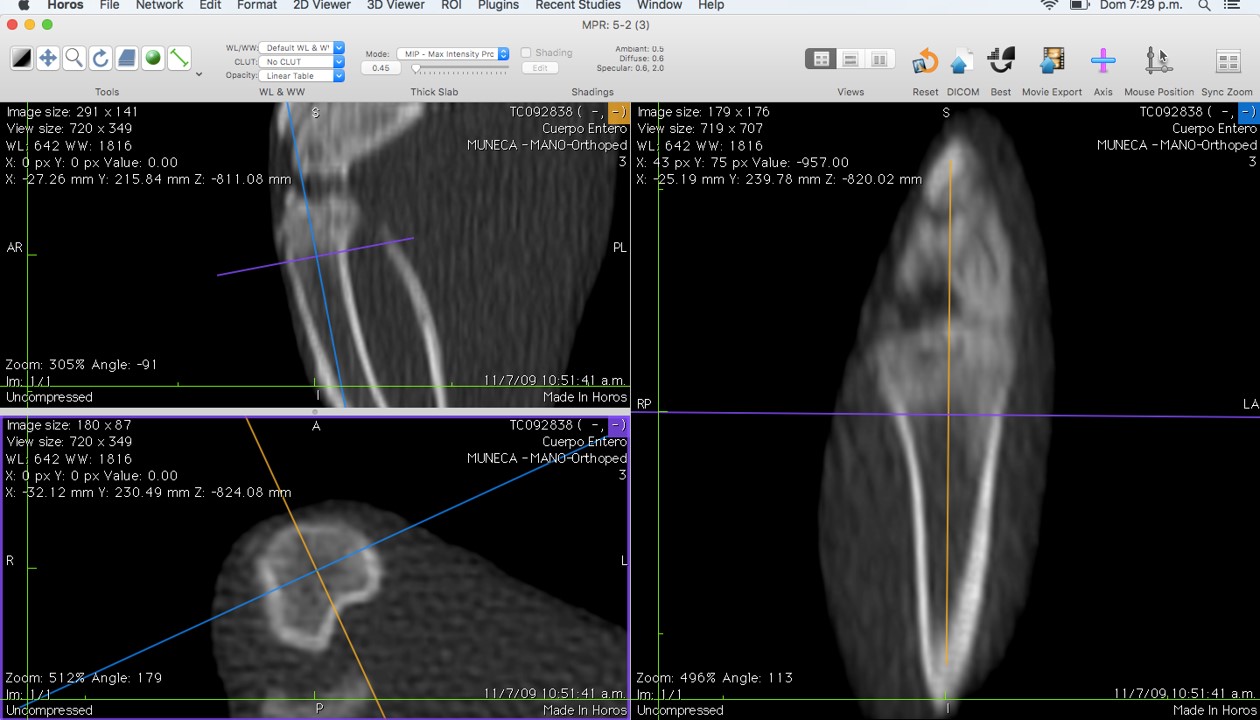 Figure 1: Image shows standardized measurements performed with the HOROS program under environment Mc Intosh. Multiplanar review for drawings to display sagittal, coronal and axial positions, taking as reference tibial plate and placing a centered parallel to the cortical and a perpendicular intercondylar line as guides.
View Figure 1
Figure 1: Image shows standardized measurements performed with the HOROS program under environment Mc Intosh. Multiplanar review for drawings to display sagittal, coronal and axial positions, taking as reference tibial plate and placing a centered parallel to the cortical and a perpendicular intercondylar line as guides.
View Figure 1
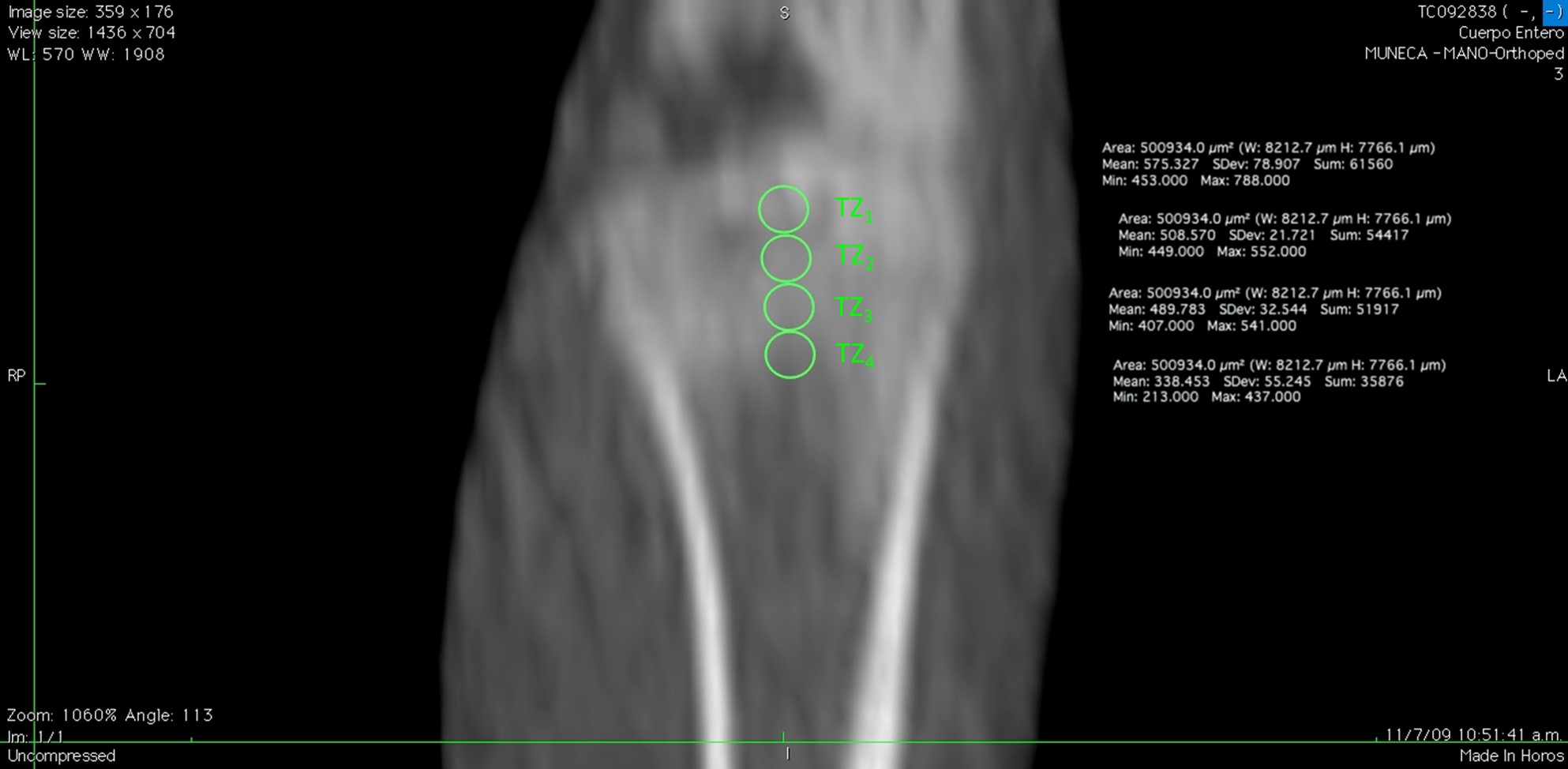 Figure 2: Image shows standardized measurements performed with the HOROS program under environment Mc Intosh. Thickness was 0.45 mm and a ROI (Region of Interest) for the measurement of density of 0.5 mm2 area. In this way four tibial zones (TZ1-4) were defined, from the tibial plate towards the metaphysis.
View Figure 2
Figure 2: Image shows standardized measurements performed with the HOROS program under environment Mc Intosh. Thickness was 0.45 mm and a ROI (Region of Interest) for the measurement of density of 0.5 mm2 area. In this way four tibial zones (TZ1-4) were defined, from the tibial plate towards the metaphysis.
View Figure 2
After rats were euthanized, tibiae were removed and cleaned of soft tissue, fixed in 10% neutral formalin, decalcified in EDTA (pH = 7.2), and processed to be embedded in paraffin. Oriented 8-10µm longitudinal sections were stained with hematoxyline-eosine (H & E), in order to asses histomorphometric values.
On digital microphotographs, with the Image Pro Plus 2.0 program, the bone volume as a percentage of total bone volume (BV/TV%) of trabecular bone in the tibiae was determined on the central area of subchondral bone. Histomorphometric measurements were divided in primary (BVA/TVA%) and secondary (BVB/TVB%) cancellous bone (Figure 3A). Also, thickness of growth plate cartilage (GPC.Th) with its hyperthrophic zone (HpZ.Th) was determined as the mean of thirteen independent records (Figure 3B).
 Figure 3: Digital micrographs of tibiae in longitudinal section, H & E A: Bar equivalent to 500 μm. Boxes show regions of primary (1°) and secondary (2°) cancellous bone. 25X. B: Ephiphyseal cartilage analyzed by image pro plus. Bars indicate 13 repeats of GPC. Th and HpZ. Th. 125X.
View Figure 3
Figure 3: Digital micrographs of tibiae in longitudinal section, H & E A: Bar equivalent to 500 μm. Boxes show regions of primary (1°) and secondary (2°) cancellous bone. 25X. B: Ephiphyseal cartilage analyzed by image pro plus. Bars indicate 13 repeats of GPC. Th and HpZ. Th. 125X.
View Figure 3
Results were expressed though descriptive statistics as mean ± standard deviation (SD). Zoometric, intake, serum lipid profile and histomorphometric measurements were compared with independent sample Student t-test. Pearson's correlation between BMD of each TZ and serum T-cho was performed. All results proved to be Normal (Wilk Shapiro of residuals) and of equal variances (Barlett's test). For statistical calculations "Statistix for Windows 2.1" Copyright© 1985, 99 Analytical Software, was used. Significance level was set at 5% probability.
At 7w, zoometric body weight and length had no significant differences (p > 0.05) (Figure 4). This proved that our experimental model paralleled child growth pattern up to young adult, showing no anthropometric differences by HFD intake. During the first three weeks of rapid growth and the next four, in which adult size was acquired, diet intake did not differ significantly between groups (p > 0.05) (Figure 5), nor did water consumption throughout experimental period (p > 0.05).
 Figure 4: Zoometry: Body weight (g) and length (cm) in control (C) and experimental (E) groups at initial time (t0) and 7w (t7). Data are expressed as mean ± SD (n = 6/group). NS (p > 0.05), between groups.
View Figure 4
Figure 4: Zoometry: Body weight (g) and length (cm) in control (C) and experimental (E) groups at initial time (t0) and 7w (t7). Data are expressed as mean ± SD (n = 6/group). NS (p > 0.05), between groups.
View Figure 4
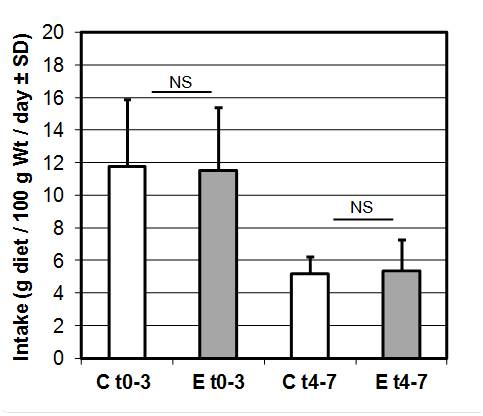 Figure 5: Intake (g diet/100g Wt/day) NS (p > 0.05) between groups, at 0-3w (t0-3) and 4-7w (t4-7). Data as mean ± SD control (C) and experimental (E).
View Figure 5
Figure 5: Intake (g diet/100g Wt/day) NS (p > 0.05) between groups, at 0-3w (t0-3) and 4-7w (t4-7). Data as mean ± SD control (C) and experimental (E).
View Figure 5
Serum lipid-lipoprotein profile confirmed experimental diet's atherogenic capacity. This was evidenced in E, by a significant increase of T-cho and n-HDL-cho (p < 0.0001), and decrease of TG (p < 0.001) at 7w. Conversely, HDL-cho showed no statistical differences (p > 0.05) (Figure 6).
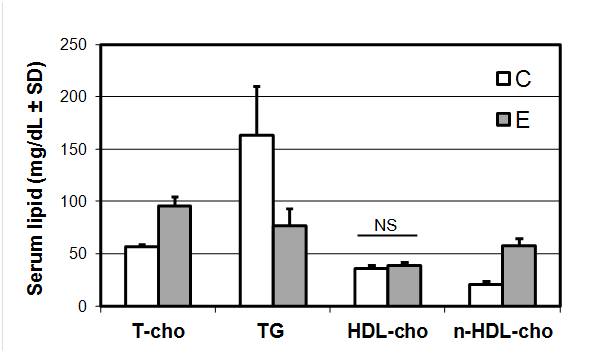 Figure 6: Serum lipid-lipoprotein profile (mg/dL): Total cholesterol (T-cho), triglycerides (TG), high density lipoprotein-cholesterol (HDL-cho), non-HDL-cholesterol (n-HDL-cho) at 7w. Data as mean ± SD control (C) and experimental (E). ***p < 0.0001; **p < 0.001; NS (p > 0.05).
View Figure 6
Figure 6: Serum lipid-lipoprotein profile (mg/dL): Total cholesterol (T-cho), triglycerides (TG), high density lipoprotein-cholesterol (HDL-cho), non-HDL-cholesterol (n-HDL-cho) at 7w. Data as mean ± SD control (C) and experimental (E). ***p < 0.0001; **p < 0.001; NS (p > 0.05).
View Figure 6
No significant histomorfometric differences (p > 0.05) were encountered in total bone volume, nor in primary or secondary cancellous bone areas (Figure 7, Figure 8 & Figure 9A). The same occurred in thickness of growth plate cartilage and its hyperthrophic zone (Figure 9B).
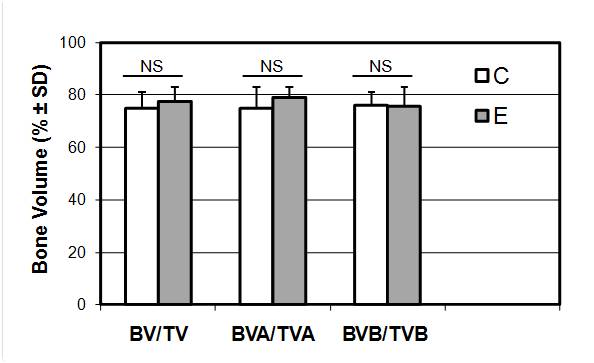 Figure 7: Bone volume (BV/TV%), primary cancellous bone (BVA/TVA%) and secondary cancellous bone (BVB/TVB%) at 7w. Data as mean ± SD control (C) and experimental (E). NS (p > 0.05).
View Figure 7
Figure 7: Bone volume (BV/TV%), primary cancellous bone (BVA/TVA%) and secondary cancellous bone (BVB/TVB%) at 7w. Data as mean ± SD control (C) and experimental (E). NS (p > 0.05).
View Figure 7
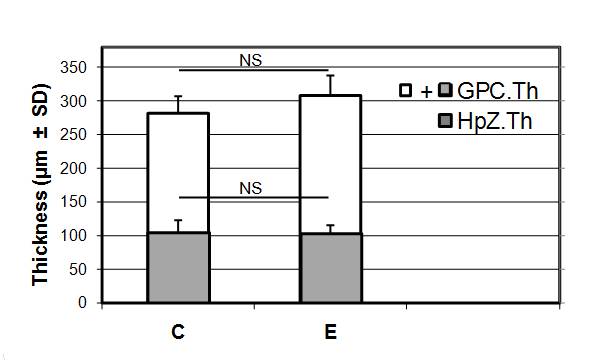 Figure 8: Thickness (μm) of growth-plate cartillage (GPC.Th) and Hypertrophic zone (HpZ.Th) at 7w. Data as mean ± SD control (C) and experimental (E). NS (p > 0.05).
View Figure 8
Figure 8: Thickness (μm) of growth-plate cartillage (GPC.Th) and Hypertrophic zone (HpZ.Th) at 7w. Data as mean ± SD control (C) and experimental (E). NS (p > 0.05).
View Figure 8
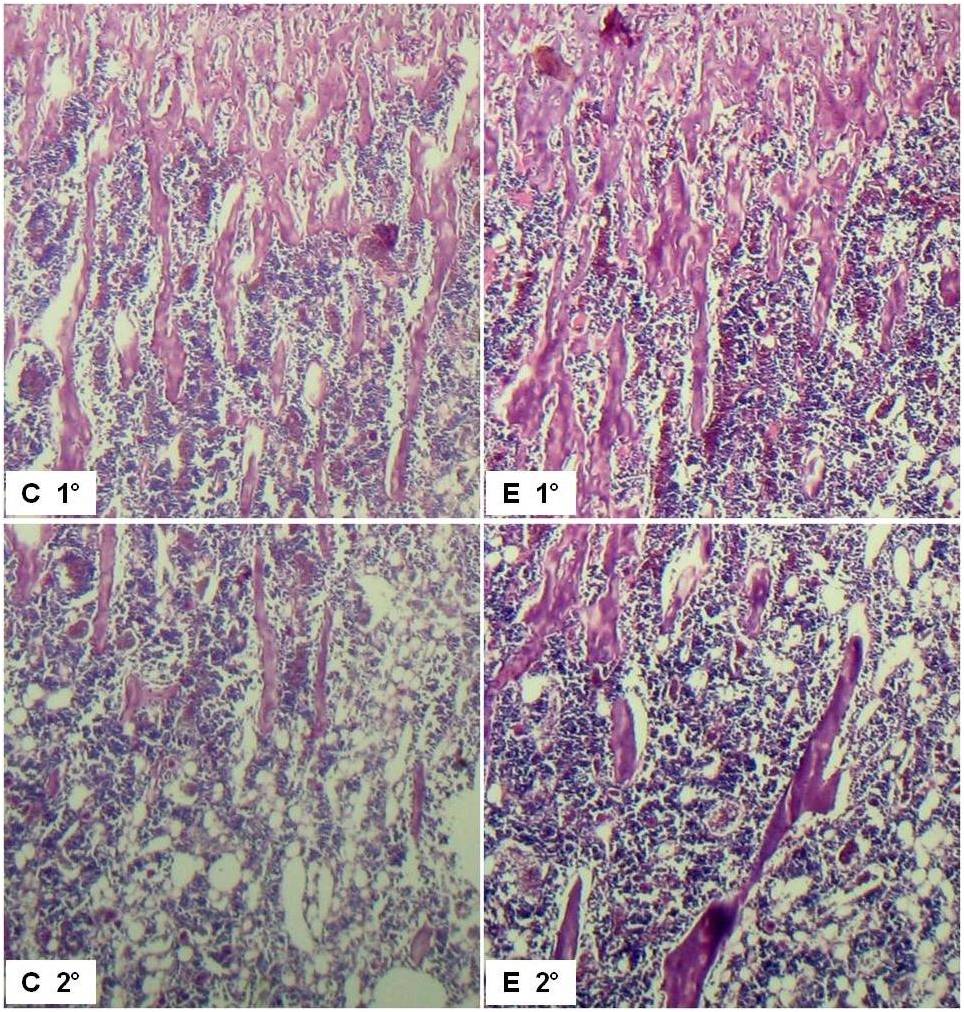 Figure 9: A) Digital micrographs of tibiae in longitudinal section, H & E 125X of control (C) and experimental (E), primary (1°) and secondary (2°) cancellous bone. B) Digital micrographs of tibiae in longitudinal section, H & E 125X of control (C) and experimental (E), ephyphyseal cartilage.
View Figure 9
Figure 9: A) Digital micrographs of tibiae in longitudinal section, H & E 125X of control (C) and experimental (E), primary (1°) and secondary (2°) cancellous bone. B) Digital micrographs of tibiae in longitudinal section, H & E 125X of control (C) and experimental (E), ephyphyseal cartilage.
View Figure 9
Inverse correlation (r) was significantly (p < 0.05) relevant for BMD and T-cho in all tibial zones studied: TZ1:- 0.8121(p < 0.001); TZ2: -0.4691 (p < 0.05); TZ3: -0.6814 (p < 0.01); TZ4: -0.8175 (p < 0.001) (Figure 10).
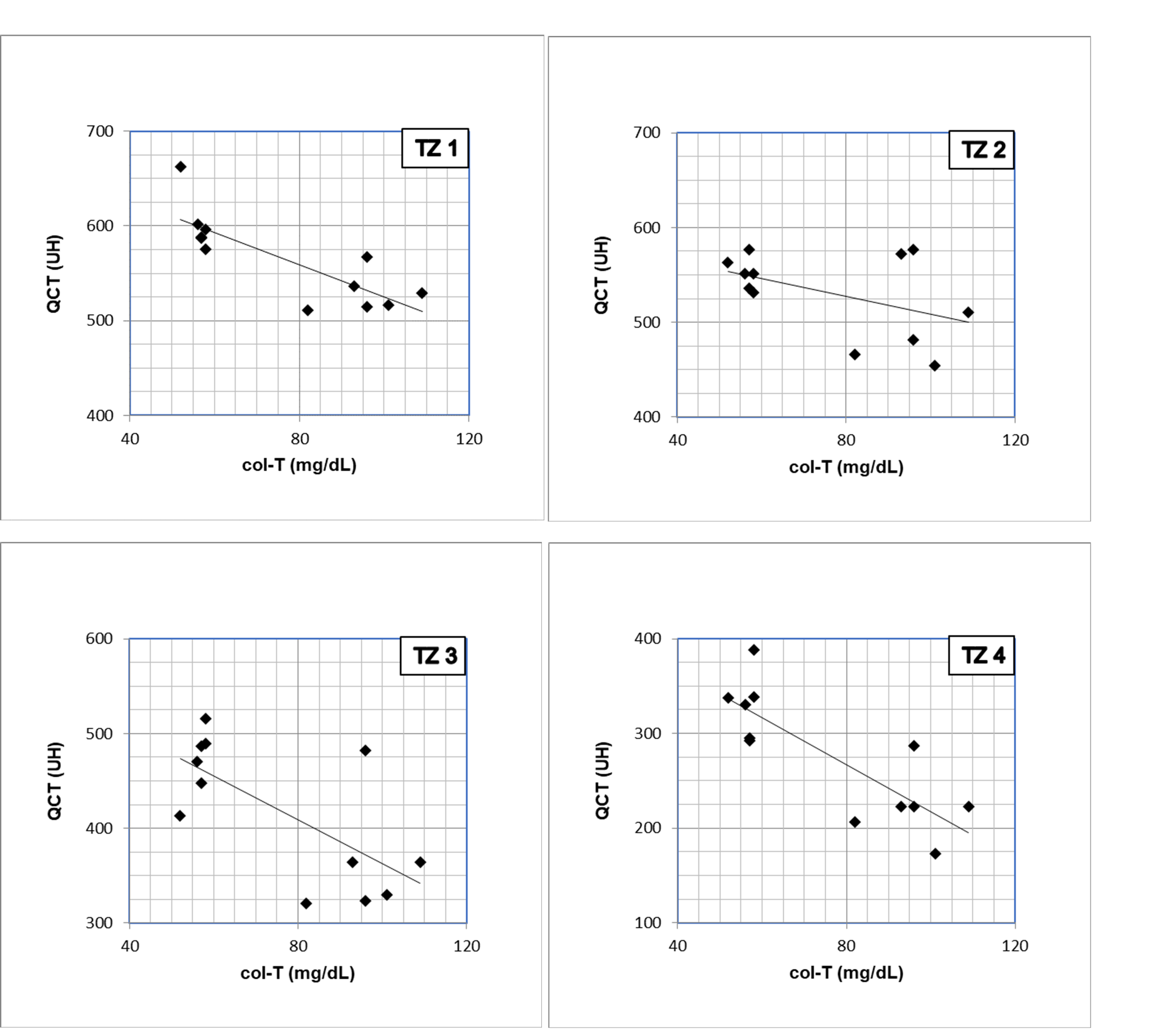 Figure 10: Tibial Zones (TZ) correlation (r) between BMD (MS-QCT) and serum T-cho (mg/dL). Each TZ was significant (p < 0.05) at 7w. TZ1: -0.8121 (p < 0.001); TZ2: -0.4691 (p < 0.05); TZ3: -0.6814 (p < 0.01); TZ4: -0.8175 (p < 0.001).
View Figure 10
Figure 10: Tibial Zones (TZ) correlation (r) between BMD (MS-QCT) and serum T-cho (mg/dL). Each TZ was significant (p < 0.05) at 7w. TZ1: -0.8121 (p < 0.001); TZ2: -0.4691 (p < 0.05); TZ3: -0.6814 (p < 0.01); TZ4: -0.8175 (p < 0.001).
View Figure 10
At the present time, studies that focus on bad eating habits, seek to anticipate on health and wellbeing. Children and adolescents are considered among the most vulnerable groups in which preventive actions are to be applied. In this sense, the risk factors that are vastly documented in literature, in the past decades, are mainly the ones related to cardio-vascular-disease in adults.
Moreover, others contribute to knowledge of high cholesterol and saturated fat eating habits, in overweight or obese infants and adolescents, but no references are aimed on those that do not show visible signs.
Routine pediatric procedures do not include assay of biochemical markers that may anticipate metabolic changes onset by bad eating behaviors, unless anthropometric changes or preceding family medical record are present.
The need to disclose the level of impact on long bone structure of adults that have had a long-term high fat and cholesterol diet intake during childhood and adolescence was the focus of this study. Our experimental model in growing rats, made possible to assess in tibiae the bone parameters that reveal long bone's association with diet. In doing so, the importance that pediatricians should take in mind when monitoring children.
Prevalence of coronary risk factors in adolescents was examined in Argentina, 2003 by FRICELA study (Coronary Risk Factors in Adolescence) [20]. Outcome showed that 11.7% (total of 2599) student teenagers aged 12 to 19 years of both genders had hypercholesterolemia (T-cho > 200 mg/dL) with a body mass index (BMI) < 25 kg/m2. Also, 35% of those students had T-cho greater than 170 mg/dL. This value established the need to carry out a fit diet and exercise regularly.
Further on, more evidence showed that T-cho values from 140 to 170 mg/dL during youth had 25% aorta's total surface covered with fat, when autopsied; while in those greater than 200 mg/dL, 50% total aortic surface was compromised. PDAY study (Pathological Determinants of Atherosclerosis in Youth) gave knowledge of 70% rise in risk of atherosclerotic plate development in adolescents and young adulthood with 50 mg/dL increase in LDL-cho. Actually, they are identified as a high-risk group. These observations clearly demonstrate the importance of cardiovascular risk factors in childhood and adolescence [20-22].
Coronary risk factors in children and young adults were associated with the early development of calcification of the coronary arteries. These were the increase in BMI, both in childhood and adulthood, the increase of blood pressure and the descent of the HDL-cho [20,23]. In our experimental model, no differences in body size and weight or HDL- cho are observed, placing these indicators in subclinical values.
Aguilar and collaborators [24] emphasize that, of the total number of children and adolescents they studied and considered healthy, prior to the determination of blood cholesterol, 22.8% (n = 153) showed values higher than normal, proving that hypercholesterolemia in children is now a reality. There are children and adolescents with alterations in blood cholesterol values that are currently considered healthy. There is also a clear influence of bad eating habits and physical inactivity in the development of these high numbers. All these evidences suggest the need to anticipate detection of lipid-lipoprotein metabolism indicators.
In a study that assessed the prevalence of cardiovascular risk factors in adolescents in public and private schools of the city of Salta in 2009, the significant increase in the levels of T-cho ≥ 200 mg/dl were evidenced in private schools, without being altered LDL, TG, HDL, or blood pressure [25]. While these levels are not away from normal values: LDL < 130 mg/dl; TG < 110 mg/dl and HDL > 40 mg/dl, they were close to the higher limits [26-28].
In our model, the serum lipid-lipoprotein profile confirmed the potential atherogenicity of the experimental diet, being the significant increase in T-cho at the expense of n-HDL-cho. While reduction of TG indicates a change in the endogenous lipid metabolism cycle [10,15,16].
Anthropometric parameters, in our study, do not give evidence of altered nutritional history, confirmed by the unchanged endochondral growth. Therefore, it is possible that children and teenagers will grow up within normal parameters, without being perceived by the pediatrician.
In addition, a cross-sectional descriptive study conducted in Chile, between 2010 and 2011, to assess the concentrations of serum lipids in healthy school children and adolescents from a high socioeconomic level (191 children aged 5-16) shows increased values (T-cho > 200 mg/dL) in 12% of women and 5% of men with no differences by gender, or association between serum lipids and abdominal perimeter or with BMI. This highlights the importance of our model that also shows the lipid metabolic changes are not always reflected in the body image [29].
According to Dr. Cuartas, who performed a descriptive and retrospective observational study of patients (885, from 2-18 years) attending Pediatric Office between 1992 and 2012, the prevalence of hypercholesterolemia was 21%. Of them, 47% consumed a high fat diet and 87% showed a proper BMI [30]. Bearing in mind that, with aging, cholesterol value tends to follow the same percentile (persistence or tracking), children who have cholesterol elevated over time, will have more possibilities of maintaining it in adult life [31-33].
In addition, a clinical research paper, presented at the XXX Annual Meeting of the Children's Hospital, Ricardo Gutierrez of Buenos Aires, Argentina, showed that it is convenient to request a lipid profile when a high fat diet in childhood is detected. The descent of the HDL-cho has a direct relationship with the diet and it is influenced by the lifestyle, a value less than 45 mg/dL, is a risk factor that can be modified [34].
In our experimental model, a high fat diet intake does not modify tibiae cancellous bone volume, as evidenced in initial mixed trabecula formation, and also when bone has replaced calcified cartilage, completing endochondral ossification. Likewise occurs in its longitudinal growth that paralleled zoometric values, as shown by growth plate cartilage. Inverse correlation between BMD and T-cho indicates bone's association with diet.
The present study, which intends to prognose endochondral ossification under high fat diet from childhood to a young adult, gives alert on the observation of long-term eating habits, which are part of the usual behavior of children and current adolescents, worldwide. For these reasons, we agree with other authors that it is necessary and urgent to implement programs focused on parents and children, to orient them about correct eating habits. It is also necessary to encourage the practice of sports to combat the sedentary lifestyle, as well as implement and stimulate attendance to complementary school activities to reduce the number of hours spent watching television or at leisure [10,24,35].
If the results of the work in this experimental model homologate the population of children and adolescents who consume diets of similar composition, the world population is in the need to identify early "at risk individuals" to act in a preventive way. From our analysis we can conclude that the consumption of a high fat diet does not modify the trabecular bone volume in the rat tibia, both in the initial formation of the spongy, or its final ossification. The same applies to the growth in length, which had corresponded with zoometric values.
These findings, taken together with BMD loss by MS-QCT, lead to think that the difference would be in the degree of mineralization of cancellous bone and not in its volume. From the present we can deduce that chronic intake of excess fat and cholesterol in diet during infancy may provoke a vulnerable bone in young adulthood that could be promptly detected by MS-QCT.
We are especially grateful to Dr Pedro Lylyk for his incommensurable generosity in providing us access to MS-QCT in ENERI, Sagrada Familia Clinic, CABA, Argentina. Also, we thank patience of computed tomography technicians and their collaboration in MS-QCT acquisition protocol settings. A special mention to Dr Silvia Friedman for her invaluable nutrition knowledge, transmitted over the years. We mention Florencia Nuñez that participated in measurements of microphotographs during her initial steps in investigation as a dentistry student of University of Buenos Aires, Argentina. Authors claim there are no forms of conflict of interest in this publication.
All authors have contributed to this paper equally.