Arterial misplacement of the venous central line catheter is not an uncommon early complication which carries devastating and fetal consequences. We report a case in which the patient condition command the use of closure devise over other surgical and endovascular options and with successful hemostasis. Stroke is a rare complication encountered in our case due to the misplaced central line.
This is a 90-years-old lady known diabetic and hypertensive, who presented to emergency room with signs and symptoms of septic shock on top of pneumonia and urinary tract infection. The primary assessment mandates a central venous access for rapid Intravenous hydration and antibiotics treatment.
At the emergency room, a 7-Fr Triple-lumen central line was inserted utilizing a right sub clavicular approach and using the anatomical landmarks technique.
The doctors have noticed an arterial blood back flow and they suspected an arterial puncture. This was confirmed on chest X-ray. The line was secured in place and labeled not for use. The patient developed Right posterior cerebral artery territory stroke few hours later confirmed by CT brain and CT angiogram of the head and neck. a consensus meeting was set including Vascular surgery, Interventional radiology and intensive care unit for the possible management measures Immediately, the vascular surgeon was consulted, and he advised to keep the line in place, labeled "not for use", and to set a plan for removal. Few hours later, the patient level of consciousness was deteriorated with drop of her Glasgow Coma Scale (GCS). urgent CT-brain was performed showing an acute right posterior cerebral artery (PCA) stroke. MR angiogram of head and neck showed right PCA, right superior cerebellar artery (SCA) territories sub-acute infarctions, with confirmation of the misplaced central line into the right subclavian artery.
The catheter tip noted within the Right Brachiocephalic artery with no associated thrombus around it and the entry site was just distal to the ostium of right internal mammary artery (RIMA) and opposing the origin of the right vertebral artery. The right vertebral artery was dominant with mild atherosclerosis at its origin. The tract distance from skin entry to the artery puncture site was approximately 8 cm. There was no other vascular injury, extravasations or hematoma. Then, IR team was consulted for endovascular line removal and arterial repair.
Giving the patient condition, and the site of arterial puncture, the plan for treatment was using a percutaneous closure devise (Angioseal®) and was based on consensus between the vascular surgeon, an intensive care unit (ICU) doctor, and interventional radiologist.
Additional to the Angioseal , 8 mm and 10 mm balloons were made available and ready if needed. An informed consent was obtained from the patient family.
The right neck, chest wall, and both groins were prepped and draped in a sterile fashion inside the interventional radiology suit.
The Right common femoral artery access was obtained, and angiogram of right brachiocephalic artery was performed (Figure 1). The entry point of the misplaced catheter is noted just proximal to RIMA and patent right subclavian, right vertebral, and RIMA.
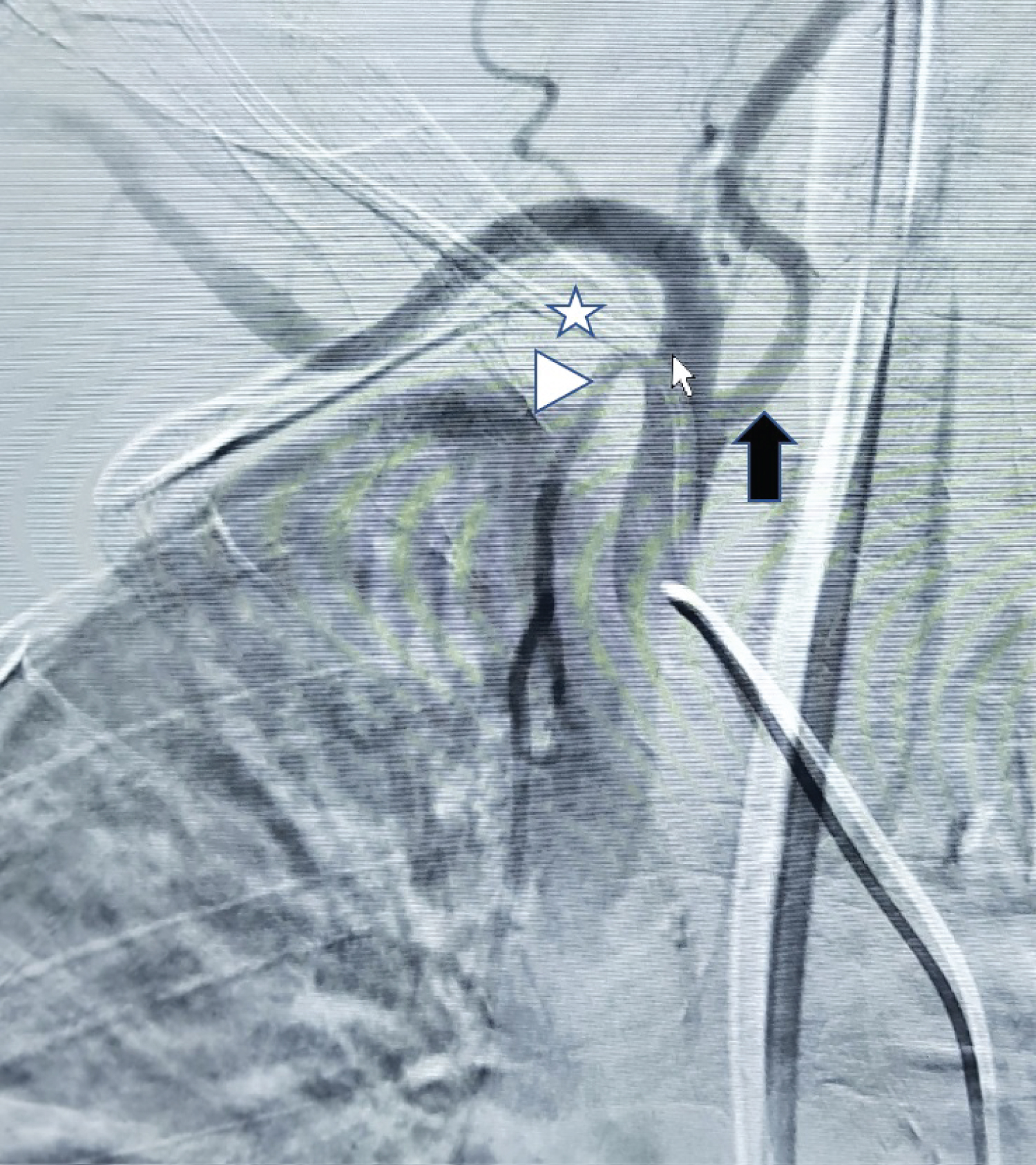 Figure 1: A right brachiocephalic artery angiogram before line removal showing the misplaced line (white star) with its entry point (small white arrow) at the proximal right subclavian artery. Note the proximity to the right internal mammary artery (white arrowhead) and the dominant right vertebral artery (black arrow).
View Figure 1
Figure 1: A right brachiocephalic artery angiogram before line removal showing the misplaced line (white star) with its entry point (small white arrow) at the proximal right subclavian artery. Note the proximity to the right internal mammary artery (white arrowhead) and the dominant right vertebral artery (black arrow).
View Figure 1
There was no extravasations.
A 0.035 Amplatz® guide wire was introduced through the pre-existing right subclavian artery line, followed by removal of the line over the guide wire. Then, a 6Fr AngioSeal® vascular closure device was introduced over the guide wire. Satisfactory hemostasis was achieved immediately.
Angiogram confirmed no vascular injury, or contrast extravasations. The right subclavian, right vertebral, and RIMA arteries were patent.
Final angiogram after 5 min confirm the successful hemostasis of the injury site without any complication (Figure 2).
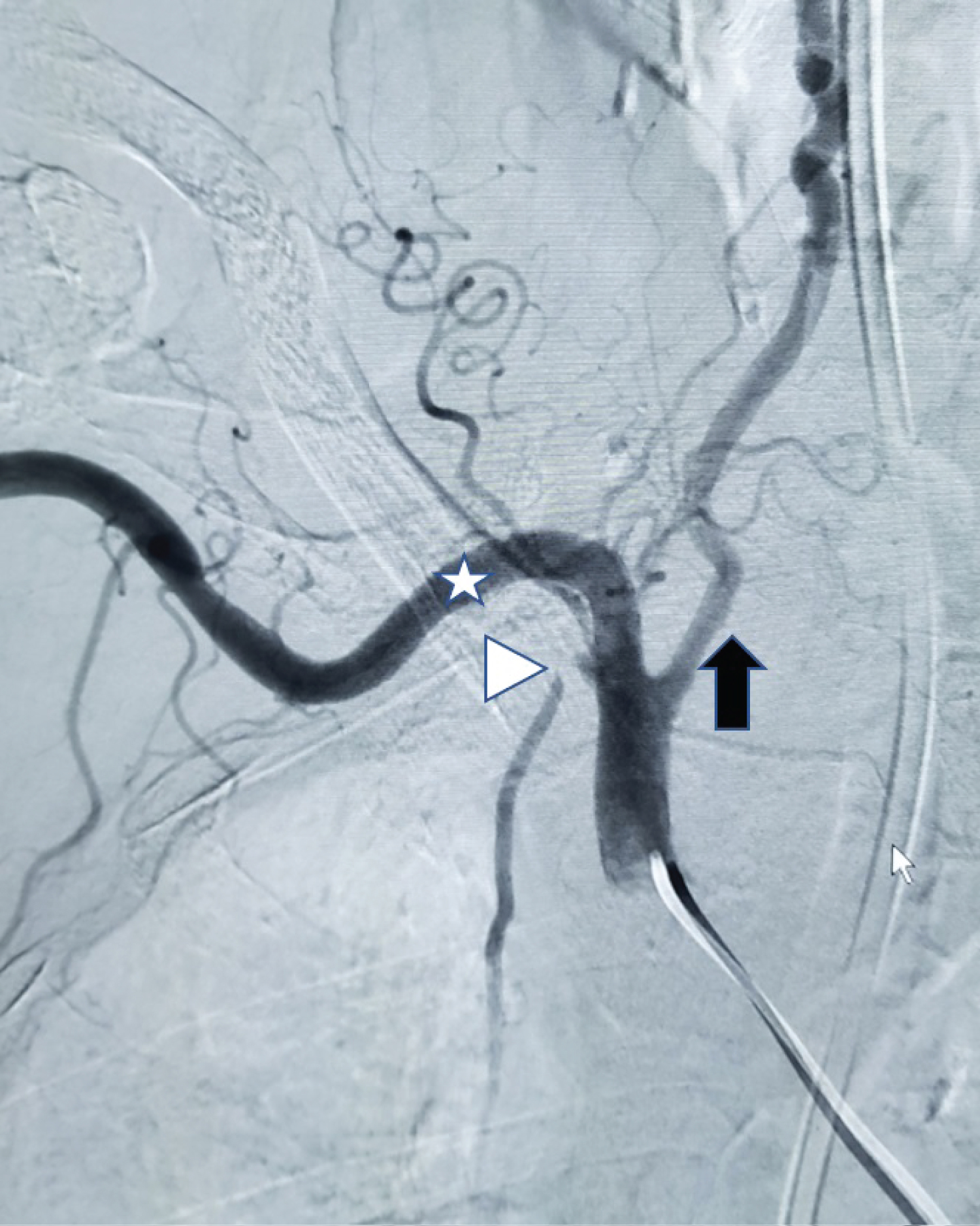 Figure 2: A right brachiocephalic artery angiogram after line removal and successful application of angioseal vascular closure device. The distal right subclavian artery (white star) and the dominant right vertebral artery (black arrow) are widely patent with no active bleeding. Also, note the mass effect over the proximal right internal mammary artery (white arrowhead) by the external collagen plug component.
View Figure 2
Figure 2: A right brachiocephalic artery angiogram after line removal and successful application of angioseal vascular closure device. The distal right subclavian artery (white star) and the dominant right vertebral artery (black arrow) are widely patent with no active bleeding. Also, note the mass effect over the proximal right internal mammary artery (white arrowhead) by the external collagen plug component.
View Figure 2
Our patient was transported to the recovery room and later to the ICU. Patient extubated and complete her hospital course and discharged after three weeks.
Arterial misplacement of the central line catheter is a well-known early complication with a reported incidence of 3.7% [1,2]. However, using a real-time ultrasound guidance showed a significant reduced risk of failure. Commonly reported complication of central line misplacement include arterial puncture, hematoma which can expand and obstruct the airway, pneumothorax, and hemothorax [3]. Other less common complications are pseudoaneurysm [1], arteriovenous fistula [4], and stroke due to intra-arterial thrombus [5].
To our knowledge stroke resulting from a subclavian arterial puncture is rare and only four cases have been reported [5-8].
The anatomical course of right subclavian artery and the proximal and deep arteriotomy site would not allow it for effective compression. Nevertheless, "pull and pressure technique" yield a devastating results [4]. A covered stent would be an attractive option [9]; however, it would occlude the vertebral artery and the open surgical repair with thoracotomy carries out a high morbidity and mortality rates in a such very ill patient.
The Angioseal device is designed to provide rapid and safe hemostasis after femoral artery puncture. It relies on a small collagen plug on the outer arterial wall held against the puncture site by a small collagen footplate inside the artery.
The off-label use of Angioseal vascular closure devise (Figure 3) in inadvertently catheterized subclavian arteries has been reported previously, where satisfactory hemostasis was achieved [1,4,9-12]. It is recommended for use if the length of the track from the puncture site to skin entry is less than 8 cm and after 8Fr catheter insertion but has been used successfully with 10Fr arteriotomy [9]. Other endovascular management include Suture mediated closure device [9,13], Balloon tamponade, Gradual Sheath downsizing and tract embolization on the outer-lumen side of the subclavian artery have been reported [9].
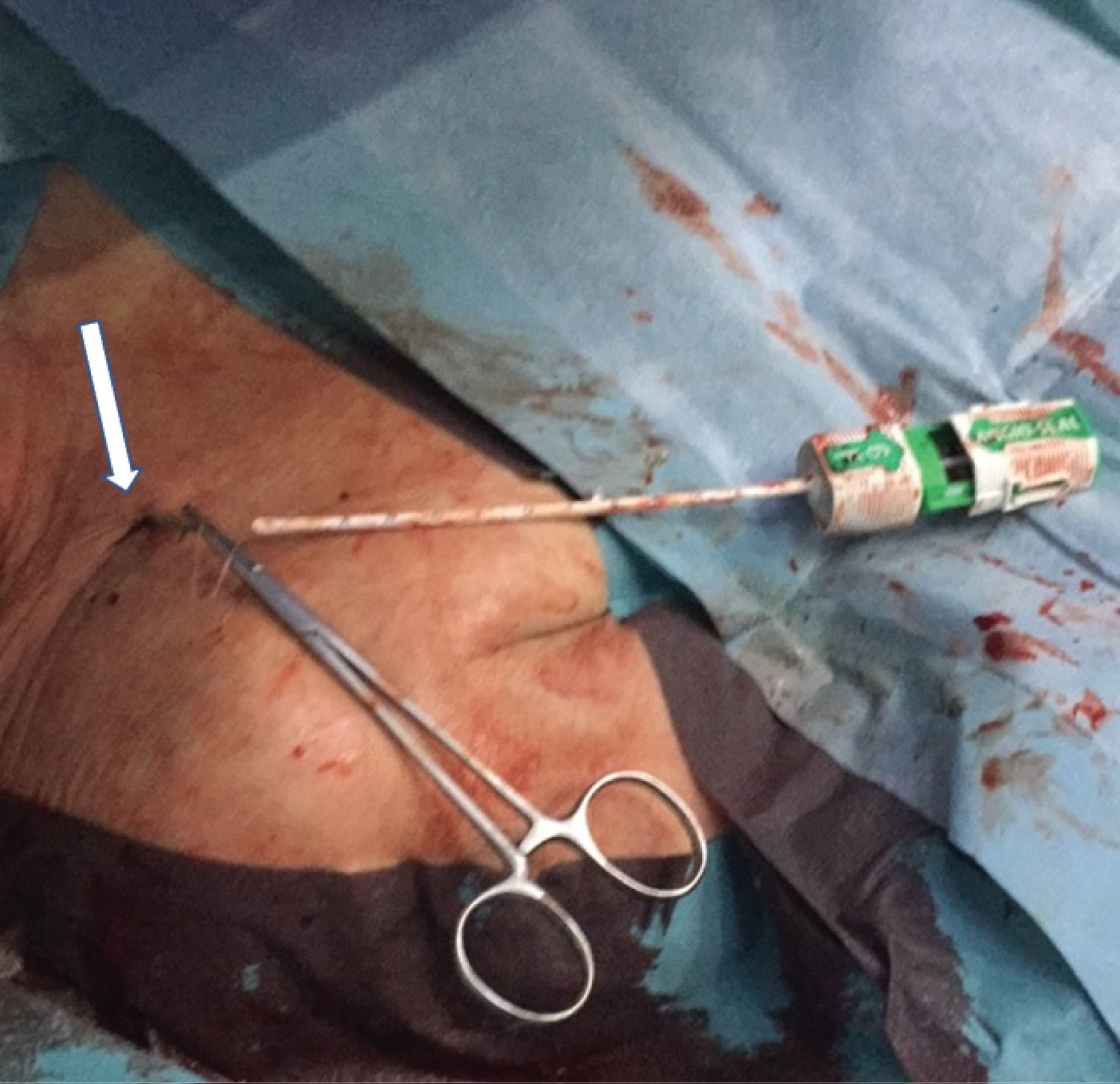 Figure 3: A digital photograph during the application of angioseal vascular closure device. Note the infraclavicular skin entry point (white arrow).
View Figure 3
Figure 3: A digital photograph during the application of angioseal vascular closure device. Note the infraclavicular skin entry point (white arrow).
View Figure 3
Inadvertent arterial puncture during central line placement is not an uncommon complication which carries devastating and fetal consequences. Once the arterial puncture is confirmed, it should be in situ and not used. Further imagining is recommended to assess the injury with prompt vascular surgeon and interventional radiology consultations to plan for management. Stroke is a rare complication encountered in our case; only four cases reported. Our case is unique in presenting which command the use of closure devise over other surgical and endovascular options. The Angioseal closure devise is licensed for use in femoral arteriotomy however, it provided successful hemostasis of the subclavian artery puncture in our patient.
None.