A 72-year-old woman with a history of acute renal failure treated with a bilateral double-J stent, presented with subacute bilateral lumbar pain, mild fever, and weight loss. Physical examination was normal, except for bilateral lumbar sensibility. Laboratory tests were normal an abdominal CT scan has been performed.
Post-contrast CT showed paraspinal and irregularly contoured soft tissue mass, not enhanced, infiltrating the periaortic soft tissues, invading the anterior peri-renal space (Figure 1) and surrounding the left adrenal gland (Figure 2).
 Figure 1: Paraspinal soft tissue mass extended to left anterior perirenal space, destructing the pancreatic caudal parenchyma.
View Figure 1
Figure 1: Paraspinal soft tissue mass extended to left anterior perirenal space, destructing the pancreatic caudal parenchyma.
View Figure 1
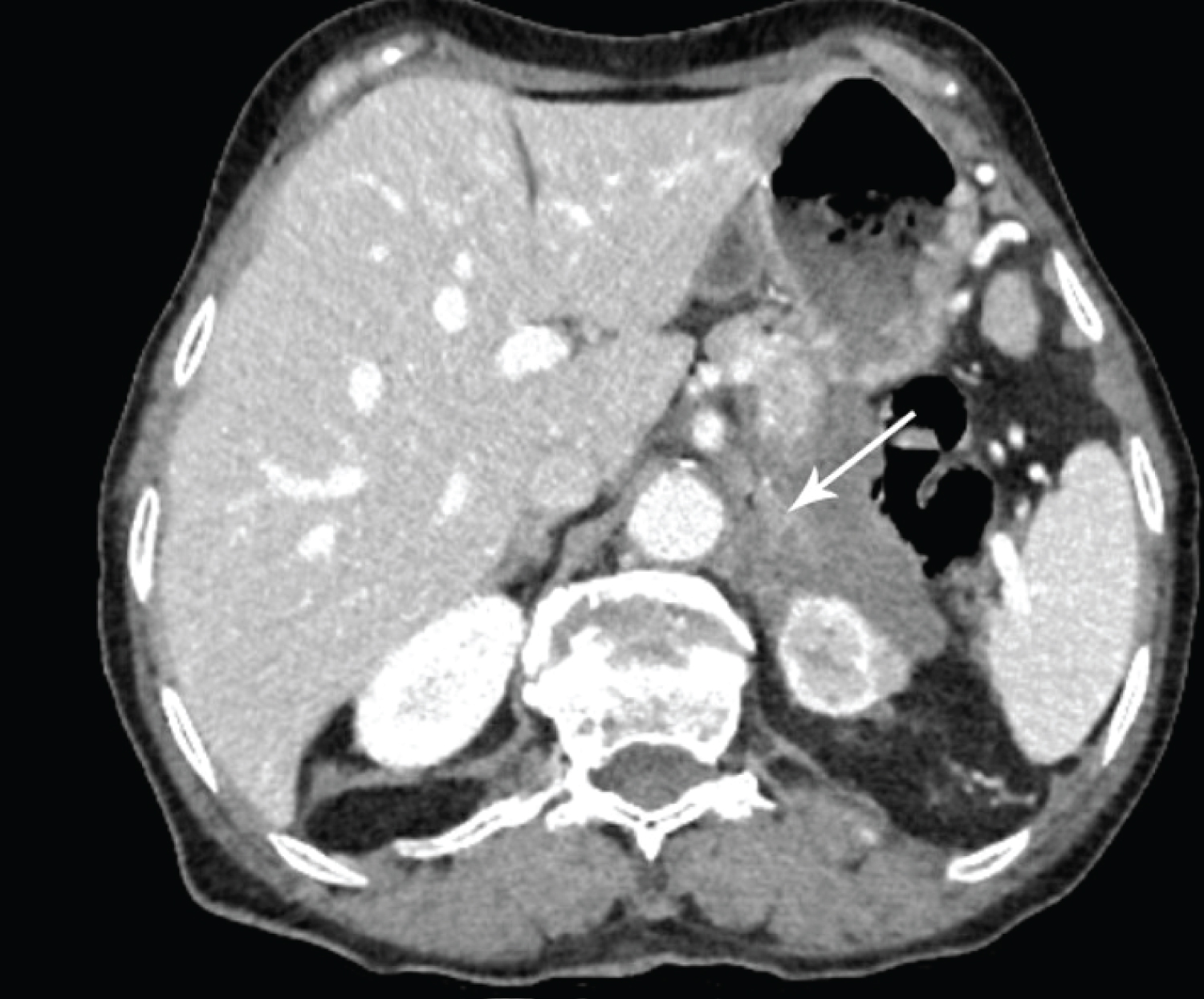 Figure 2: Adrenal gland (arrow) surrounded by retroperitoneal fibrosis.
View Figure 2
Figure 2: Adrenal gland (arrow) surrounded by retroperitoneal fibrosis.
View Figure 2
This process damages the tail of the pancreas and infiltrates the distal third of the transverse colon (Figure 1). It is extended and encased bilaterally the pelvic uretere at the level of the L4 vertebra (Figure 3).
 Figure 3: Soft-tissue density in the retroperitoneum extended and encased the abdominal part of the bilateral ureter.
View Figure 3
Figure 3: Soft-tissue density in the retroperitoneum extended and encased the abdominal part of the bilateral ureter.
View Figure 3
A. Retroperitoneal fibrosis is a rare fibro-inflammatory disease characterized by an extensive fibrous formation in the retroperitoneal space. It can be classified as idiopathic also known as Ormond’s disease or secondary. It is idiopathic in most cases (> 75%) [1] but it can be secondary to surgery, malignant disease, radiation exposure, or retroperitoneal bleeding [2]. Idiopathic retroperitoneal fibrosis is due to an inflammatory reaction to an atherosclerotic plaque of the abdominal aorta [3].
B. The most common symptoms signs are back pain and abdominal pain. The diagnostic is often delayed due to non-specific clinical presentation [4].
C. Imagery is useful in the diagnosis, prognosis, and differential diagnosis.
Sonography has a low sensibility and it shows hypoechoic or anechoic, irregularly contoured retroperitoneal mass.
CT detects the retroperitoneal fibrosis as paraspinal, well-demarcated although irregularly contoured mass that is iso-dense surrounding muscle. It shows the extension of fibrosis, which may occur anteriorly to involve the pancreas, duodenum, and spleen. There is a correlation between the activity of the fibrotic process and the degree of enhancement. CT is also useful to detect the primum movens such as abdominal aortic aneurysms or inflammation. CT may be beneficial to differentiate between benign retroperitoneal fibrosis from neoplasia, malignant retroperitoneal fibrosis tends to be larger and display a mass effect.
On MRI, the soft tissue mass is hypointense on T1W and T2W unless there is an active inflammatory process whereby it is hyperintense on T2W images [5].
D. Idiopathic retroperitoneal fibrosis is usually treated with steroids in the early stsages, surgical treatment may be needed in case of ureteral obstruction. Early and properly treated, idiopathic retroperitoneal fibrosis has a good prognosis. Otherwise, it can cause severe complications such as chronic renal failure [3].
E. Retroperitoneal fibrosis is a rare but serious disease. If early and properly treated and diagnosed, it has a good outcome.
Idiopathic retroperitoneal fibrosis.
Retroperitoneal bulky lymphoma, retroperitoneal sarcoma, and retroperitoneal metastatic lymphadenopathy.