Background: The significant justification for why vascular cognitive impairment (VCI) happens is because of cerebrovascular disease. If not recognized early, this will prompt vascular dementia. To have the option to analyze VCI the assessment procedure ought to be foremost, in order to assist with effective treatment strategy to forestall extra vascular harm.
Objective: The purpose of this meta-analysis is to evaluate the scoring system used to assess VCI after magnetic resonance imaging (MRI) technique.
Methods: A PRISMA selection protocol was used to identify neuroimaging studies across electronic database such as PubMed, Google scholar, Embase and web of science from May 13, 2011 to October 10, 2022. A total of 26 studies evaluating neuropsychological assessment such as Educational experience, Mini-mental state examination (MMSE), Montreal cognitive assessment (MoCA), Fazekas perivascular (PV) Score, Hamilton depression rating scale (HAMD), Hamilton anxiety scale (HAMA) and Activities daily living scale(ADL) for VCI after MRI method. Meta-analysis was performed by Rev-Man 5.4.
Results: The meta-analysis included 26 MRI studies on VCI patients and control. The studies included a total number of 2,253 individuals, 1,192 were in the control group and 1,061 patients in VCI group. The cognitive function assessed by the meta-analysis revealed VCI with lesser MMSE scores (Heterogeneity: Tau2 = 6.75; Chi2 = 879.81, df = 19 (P < 0.00001); I2 = 98%) and MoCA scores (Heterogeneity: Tau2 = 12.76; Chi2 = 736.56, df = 15 (P < 0.00001); I2 = 98%) respectively. The analysis showed that, educational level is positively related with cognitive function in VCI patients (Heterogeneity: Chi2 = 39.68, df = 20 (P = 0.005); I2 = 50%). The control group observed a lesser HAMA and Fazekas PV score compared to VCI. But there was no significant difference for HAMD and ADL between the two groups.
Conclusion: Cognitive performance in subjects with VCI can be evaluated using neuropsychological scoring system following MRI technique. Furthermore, MMSE and MoCA scores following education increases positive cognitive function.
Vascular cognitive impairment, MRI, Cognitive impairment, Neuroimaging, Scoring system
MRI: Magnetic Resonance Imaging; VCI: Vascular Impairment; VaD: Vascular Dementia; MMSE: Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; HAMA: Hamilton Anxiety scale; HAMD: Hamilton Depression rating scale; Fazekas PV: Fazekas Perivascular; ADL: Activities Daily Living scale; I2: Inconsistency Statistic; CI: Confidence Interval; SIVD: Subcortical Ischemic Vascular Disease; VCIND: Vascular Cognitive Impairment, No Dementia; WMH: White Matter Hypersensitivity; CT: Computed Tomography; FAB: Frontal Assessment Battery
The definition of vascular cognitive impairment (VCI) is when the whole vascular brain pathologies play a role in any level of cognitive impairment, that ranges from subjective cognitive decline to dementia [1-3]. A neuropathological study revealed that pure vascular disease (8-10%), Alzheimers disease (60-70%) and dementia with lewy bodies (10-25%) play a greater role in dementia cases [4]. There are three categories of VCI which include vascular dementia (VaD), Alzheimer's disease (AD) with a vascular component and vascular cognitive impairment with no dementia (VCIND) [5]. Studies by O'Brien, et al. suggested that people with VCI have a particular cognitive reports which includes conservation of memory and executive function is reduced which differs from AD [2]. Studies on VCI mechanism is still under research and also subcortical ischemic vascular disease (SIVD) which is a type of cerebral vascular disease is considered to be chief cause of VCI [6]. VCI is still important to doctors and researchers due to probable prevention, expense and its incidence [7]. The pathologies (cerebrovascular) of VCI are white matter hyperintensities (WMH) and infarct which occurs due to ischemia [8,9]. The severity of white matter damage is usually as a results of obstruction of small blood vessels and this can be assessed by the Fazekas scale [10].
To measure the severity and ascertain the state of vascular brain injury, imaging of the brain becomes paramount. Detection of small brain lesions, WMH, microbleed and superficial siderosis, MRI is selected over computed tomography due its sensitivity [11,12]. Patient's age should be considered when weighing the burden of brain atrophy and vascular brain lesions, because the occurrence of WMH increase from 50% to 95% at 45 and 80 years respectively in the overall populace [13,14]. Usually patients who do not show any symptoms also present with silent brain infarcts, lacunes, microbleeds, evident perivascular space and brain atrophy [11-14].
Individuals with VCI show heterogeneous cognitive manifestation. Conventionally, VCI is represented by mental deceleration and poor executive function in combination with gait loss and urinary incontinence. But the cognitive impairment can be affected depending on the area of vascular brain injury [15]. Intellectual or cognitive assessment can be achieved by simple bed side test or use of screening tools such as the Montreal Cognitive Assessment (MoCA) which has been developed to this end [16]. The administration of mini-mental state examination (MMSE) can also be used to uncover executive dysfunction but this tool needs probing with supportive tests such as frontal assessment battery (FAB) [16,17]. Other screening tests such HAMA and HAMD also use questionnaire to indicate depression and also as a guide to evaluate recovery [18,19]. In addition ADL profile measures everyday activities for individuals with VCI [20]. To gain further insight into the neuropsychological assessment, the meta- analysis aims to evaluate the scoring system for VCI following an MRI examination.
The current meta-analysis followed the PRISMA guidelines [21]. This search was executed to identify literature concerning MRI examination in relation with scoring system evaluation for patients with vascular cognitive impairment (VCI). Electronic database such as PubMed, Google scholar, Embase and web of science from May 13, 2011 to October 10, 2022 were queried using the keywords such as; Vascular cognitive impairment; MRI; Cognitive impairment; Neuroimaging; and Scoring system. All articles were checked by title and abstract to decide their importance to the study question. Relevant articles in relations with the study question were successively added (Figure 1).
 Figure 1: Prisma flow diagram.
View Figure 1
Figure 1: Prisma flow diagram.
View Figure 1
• Cerebral vascular abnormality (hemorrhage, infarction and ischemia)
• Patients with Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy.
• Patients with white matter hyperintensities (WMH)
• MRI and sub-types (resting state functional MRI)
• Assessment of all enrolled patients within the range of cognitive impairment
• Studies with stages of VCI (SVCI and MCI)
• Disease of the brain such as poisoning, immune abnormalities etc.
• Intercranial tumors
• Patients with visual impairment
• Patients who Fail to cooperate
• Non-English papers
• Reviews
• Case reports
Data were collected for selected literature. Firstly, data about author, publication year, nationality, age, total number of patients, VCI and control was recorded as shown in Table 1. Educational experience, MMSE scores, MoCA scores, HAMA scores, HAMD scores, Fazekas PV scores and ADL scores as shown in Table 2.
Table 1: General characteristics of included studies. View Table 1
Table 2: Outcomes after cognitive testing. View Table 2
A total of 956 studies were retrieved by database search. 355 articles were remaining after duplicate articles were removed. The remaining 355 articles were screen thoroughly after reading the title and abstracts. After screening, 312 were excluded because it did not meet the requirements. This led to 43 articles remaining which were reviewed in detail and finally 26 articles were included in the meta-analysis as shown in Figure 1. The total number of patients recorded in 26 included studies were 2,253. Out of these patients, 1,192 were in the control group and 1,061 patients in VCI group. 23 of the included studies were conducted in China, 1 in Taiwan, 1 in Egypt and 1 in Italy as shown in Table 1. Studies reported neuropsychological assessment such as educational experience, MMSE, MoCA, Fazekas PV, HAMA, HAMD and ADL as shown in Table 2.
Statistical analysis was accomplished using the Review Manager (RevMan) software, version 5.4 presented by the Cochrane collaboration. Continuous variables were pooled using mean difference with a 95% CI. Random effect and fixed effect models were computed under statistical methods of Mantel-Haenszel for OR. Heterogeneity among studies was evaluated using the inconsistency statistic (I2). If I2 was < 50%, the eligible studies were considered to be homogenous; hence, the fixed effect model was used. In contrast, if I was > 50%, the pooled results were said to be significant, heterogeneous, and the random effect model was used in its place. For studies that present with median and range, Hozo, et al. [48] was used to calculate for mean and standard deviation.
MMSE score is by and large utilized for screening patients with dementia and the score ranges between 0-30. Higher MMSE scores show better mental capability's score of 24 following educational correction is suggested for patients with VCI [49]. Twenty studies [22-28,30-35,37-40,44,46,47] collected MMSE scores. There was a statistically significant difference between the two groups. The VCI (n = 840) saw a lesser MMSE score as compared to the control (n = 974). Heterogeneity: Tau2 = 6.75; Chi2 = 879.81, df = 19 (P < 0.00001); I2 = 98%. Test for overall effect: Z = 6.28 (P < 0.00001) (Figure 2a).
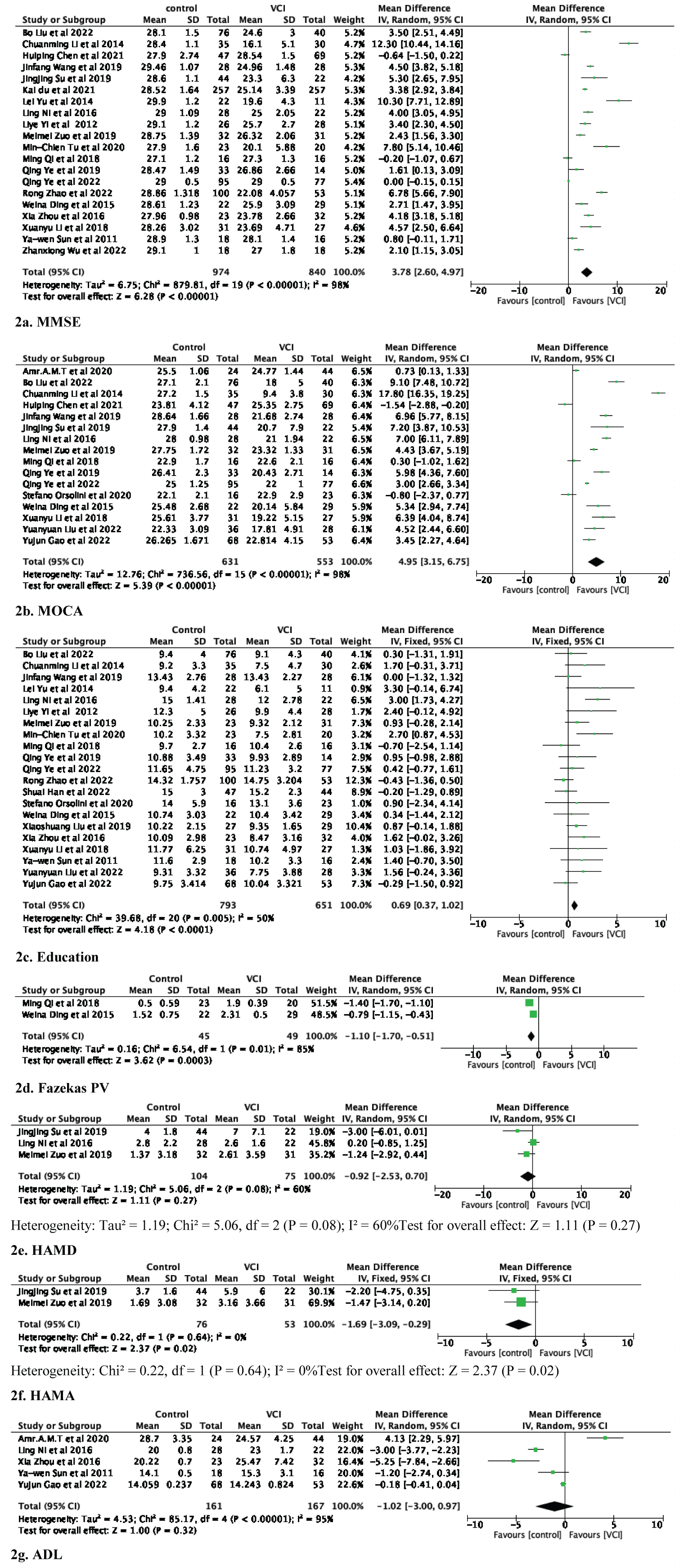 Figure 2: Forest plot of Control versus VCI: (a) MMSE; (b) MOCA; (c) Education year; (d) Fazekas PV; (e) HAMD; (f) HAMA; (g) ADL.
View Figure 2
Figure 2: Forest plot of Control versus VCI: (a) MMSE; (b) MOCA; (c) Education year; (d) Fazekas PV; (e) HAMD; (f) HAMA; (g) ADL.
View Figure 2
The MOCA is utilized for VCI and mild dementia which has been uncovered in examinations to have high responsiveness and particularity for separating individuals with VCI and the people who do not [50]. MoCA scores range from 0-30. Higher MoCA score represents good cognitive function and a cut off of 26 following education is need for people with cognitive disorders. The MOCA score was recorded in sixteen studies [23,24,27,30,31,33,37,39,40-47]. The meta-analysis showed a statistically significant difference between the two groups. Patient with VCI (n = 553) had a lesser MoCA score than those in the control group (n = 631). Heterogeneity: Tau2 = 12.76; Chi2 = 736.56, df = 15 (P < 0.00001); I2 = 98%. Test for overall effect: Z = 5.39 (P < 0.00001) (Figure 2b).
Twenty-one studies [22,23,25-33,36-37,40,42-47] recorded number of subjects that underwent education. The results discovered a significant difference between the control (n = 793) and VCI (n = 651). The educational years was decrease in the VCI group than control group. Heterogeneity: Chi2 = 39.68, df = 20 (P = 0.005); I2 = 50%. Test for overall effect: Z = 4.18 (P < 0.0001) (Figure 2c).
The Fazekas score suggests that the entire brain's white matter is hypersensitive. Additionally, this score may be used to predict future disability [10]. Two studies [27,46] recorded Fazekas PV scores. The result revealed a statistically significant difference. The control group (n = 45) observed a lesser Fazekas PV score than the VCI (n = 49). Heterogeneity: Tau2 = 0.16; Chi2 = 6.54, df = 1 (P = 0.01); I2 = 85%. Test for overall effect: Z = 3.62 (P = 0.0003) (Figure 2d).
Both scores are used to measure difference in anxiety and depression in individuals. it ranges from 21-29. A score of 29 indicated severe anxiety and depression, 21-29 (obvious anxiety and depression), 14-21 (anxiety and depression), 7-14 (indicates anxiety and depression may exist but not serious) and less than 7 shows good living conditions [51]. HAMD score was collected in three studies [24,31,33], with control with 104 and VCI 75 patients respectively. But there was no significant difference among the control (n = 104) and VCI (n = 75) Heterogeneity: Tau2 = 1.19; Chi2 = 5.06, df = 2 (P = 0.08); I2 = 60%. Test for overall effect: Z = 1. 11 (P = 0.27) (Figure 2e).
The two studies [24,31] retrieved for HAMA score showed a significant difference. The control (n = 76) had lesser HAMA score than VCI (n = 53). Heterogeneity: Chi2 = 0.22, df = 1 (P = 0.64); I2 = 0%. Test for overall effect: Z = 2.37 (P = 0.02) (Figure 2f).
The meta-analysis executed on five studies [26,28,33,41,43] showed no significant difference between control (n = 161) and VCI (n = 167). Heterogeneity: Tau2 = 4.53; Chi2 = 85.17, df = 4 (P < 0.00001); I2 = 95%. Test for overall effect: Z = 1.00 (P = 0.32) (Figure 2g).
The funnel plot on educational years (control vs. VCI) is shown in Figure 3. Because most studies placed inside the 95% CI limits, no evidence of publications bias was noted. Egger test was performed to provide statistical evidence regarding funnel plot symmetry. Result still did not reveal any evidence of publication bias in mortality (Heterogeneity: Chi2 = 39.68, df = 20 (P = 0.005); I2 = 50%).
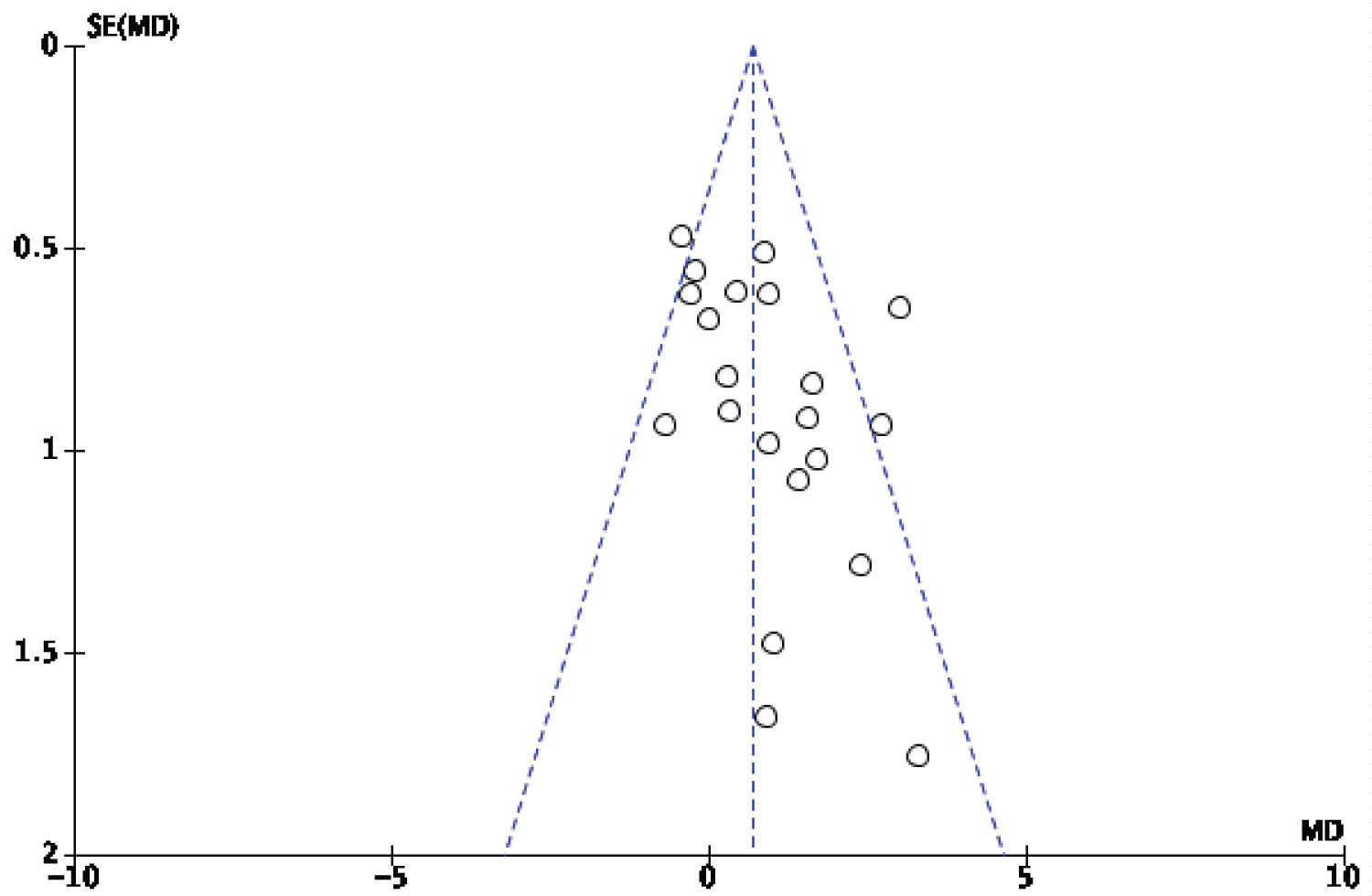 Figure 3: Funnel plot of educational years between control and VCI.
View Figure 3
Figure 3: Funnel plot of educational years between control and VCI.
View Figure 3
The present meta-analysis was conducted to investigate the scoring tools for VCI after MRI examination. Vascular cognitive impairment may be the initial stage of dementia. During the past decade, neuroimaging has gained increasing interest as a tool used for predicting mental disorders [52]. Precise screening of the beginning phases of VaD expects outrageous significance, taking into account the high commonness paces of vascular cognitive impairment and the accessible essential and auxiliary counteraction procedures.
The result of the meta-analysis exhibited that MMSE, MoCA and educational experience is legitimate psychometrically dependable device for mental screening of patients with VCI. Furthermore, the significant and fine correlations between the MoCA scores and the MMSE scores are indicative of convergent validity. On the other hand, the significant and positive correlations between each MoCA's cognitive domain and the MoCA total score are suggestive of construct-related validity [53]. The study showed a significant difference of MMSE and MoCA between VCI and control. The VCI saw a lesser MMSE (Heterogeneity: Tau2 = 6.75; Chi2 = 879.81, df = 19 (P < 0.00001); I2 = 98%) and MoCA (Heterogeneity: Tau2 = 12.76; Chi2 = 736.56, df = 15 (P < 0.00001); I2 = 98%) scores. Both patients with VCI and healthy individuals were used in a study on MoCA discriminant capability analysis (control). Age, orientation, and educational background were matched for this particular cohort. To guarantee comparable degrees of cognitive deterioration, the same clinical groups were matched for MMSE scores. Although this may have an impact on the correlation coefficient between the two tests, it is thought to be crucial for reliable comparison analysis. The outcomes showed that both the full and short forms of the MoCA productively segregate the cognitively adults from both clinical groups. MoCA scores in healthy patients was higher as compared to those in the clinical groups. But, between VaD and AD, the MoCA scores did not reveal any significant difference [53]. The present study revealed a significant difference for educational experience between VCI and control, where the VCI saw a low educational level than the control (Heterogeneity: Chi2 = 39.68, df = 20 (P = 0.005); I2 = 50%). Two groups made up of healthy control (HC) and VaMCI. examined in earlier studies documented education, MoCA, HAMA and HAMD. The outcome of the studies resulted in VaMCI having low education (p = 0.017) and decrease MoCA score (p < 0.001), HAMA (p = 0.009) and HAMD scores (p = 0.006) were also high for VaMCI than HC [54]. However, the meta-analysis disclosed no significant difference for HAMD score between VCI and control (Heterogeneity: Tau2 = 1.19; Chi2 = 5.06, df = 2 (P = 0.08); I2 = 60%). Also, there was a significant difference for HAMA scores, whereby VCI saw a low HAMA scores as compared to control. Although there was no significant difference for ADL between the two groups. ADLs should be well thought out in regards with age of person and the state of impaired cognition [55]. Additionally, the study also showed a lesser Fazekas PV scores (Heterogeneity: Tau2 = 0.16; Chi2 = 6.54, df = 1 (P = 0.01); I2 = 85%) for control group as compared to the VCI. Fazekas PV scores in other studies were recorded to be high in the sVCI group [27]. Other reports disclosed that patients who have been diagnosed with stroke with cognitive impairment presented with high periventricular white matter hypersensitivities [56]. Studies by Sudo, et al. proved the relationship between mild VCI and the gravity of WMH recorded by the Fazekas scale which reveals high grades are mostly associated with cognitive impairment as compared to low grades [57].
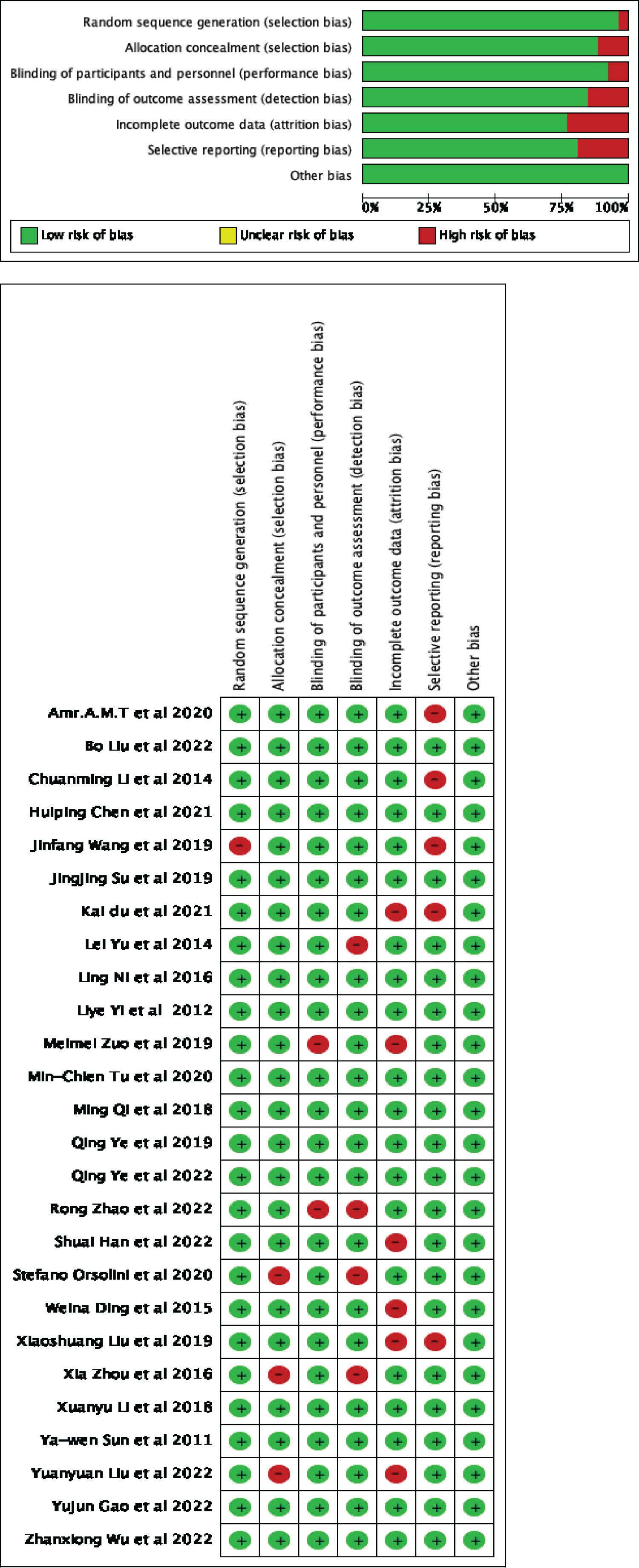 Figure 4: (a) Risk of bias graph: Review authors' judgements about each risk of bias item presented as percentages across all included studies; (b) Risk of bias summary: Review authors' judgements about each risk of bias item for each included study.
View Figure 4
Figure 4: (a) Risk of bias graph: Review authors' judgements about each risk of bias item presented as percentages across all included studies; (b) Risk of bias summary: Review authors' judgements about each risk of bias item for each included study.
View Figure 4
There are some limitations to this review. First, there are several diseases under VCI with the same pathogenesis and this could raise some limitations due to that studies that did not discuss VCI were omitted due disparity in terminology. This is because cognitive impairment related to vascular disease could not have continuously being called VCI, MCI and SVCI. Second, the small number of studies made it difficult to study a detailed unified categorization. This is because it may affect the statistical power and interpretation of the final results. In addition, the heterogeneity of the papers could not be denied because the domains of cognitive impairment in the included papers were different. Third, full texts of some articles are difficult to obtain.
Cognitive performance of VCI subjects can be assessed using a neuropsychological scoring system following MRI technology. Moreover, MMSE and MoCA scores after education enhance positive cognitive function. This may also provide a basis for new neuropsychological assessment approaches.
Would like to thank Rabarijaona Tony Manjato Ratiaray and Haibo Xu for supports towards the completion of this paper.
The studies included were retrieved from PubMed, Cochrane, Embase and Google scholar databases.
Rabarijaona Tony Manjato Ratiaray was the main contributor in data collection, statistical analysis, interpretation of data and text writing. Haibo Xu was involved in data check, critical revision of draft and data analysis. All authors approved and contributed to the research and writing of this manuscript.
No funding.
Not applicable.
Not applicable.
The authors declare they have no competing interest.