Around 10% of abdominal trauma injuries are accounted for renal injuries [1]. And amongst renal injuries, renal pedicle injuries are extremely rare. Renal pedicle injury is defined by the American Association for the Surgery of Trauma (AAST) as grade V renal injury in which the kidney is either shattered, has avulsion of renal hilum or laceration of the main renal artery or veincausing devascularization, or is devascularized with active bleeding [2]. Such injury is diagnosed by dual arterial/portal venous phase imaging for evaluation of a vascular injury of liver, spleen, or kidney [2]. Contrast enhanced CT is the golden standard in which it is recognised as a non-enhancing kidney. Perirenal haematoma is not always present and depends on the cause of the injury; If the pedicle is avulsed then there will be a large hematoma, whereas in the case of dissection hematoma isn’t necessarily seen [2]. After confirmation of the diagnosis, renal pedicle injury is managed directly through surgery either by pedicle ligation or nephrectomy depending on the extent of damage [2].
A 17-year-old male, previously healthy with no past medical or surgical history, presented to the emergency department following a motor vehicle accident. On presentation, vitals were normal; BP 120/80 mmHg, HR 80 bpm, RR 15 bpm, and SpO2 98%. The patient complained of left flank and leg pain.
Regarding the physical exam, the patient was conscious, cooperative, and oriented. An open fracture of the left tibia and abdominal bruises were inspected. On auscultation, good bilateral air entry on both lung lobes, and regular S1S2 were noted. On palpation, the abdomen was soft, non-distended and nontender.
A foley was directly inserted and urine output was clear, non turbid and no gross hematuria was seen. Laboratory studies on admission showed WBC = 25,200/cu.mm, neutrophils 89%, Hb 12.2 g/dl, Hct 37.1%, platelets 306/ul, BUN 19 mg/dl, Cr 1.28 mg/dl, blood glucose 136 mg/dl, PT 12.8 sec, Activity 80.6%, INR 1.15. Portable CXR showed mild left pneumothorax.
About 3.5 hours later, the patient started deteriorating clinically, he became tachycardic, tachypneic, and then dyspneic. Therefore, CT abdomen and pelvis without contrast (Figure 1) showed splenic laceration, so another one was done with IV contrast that further reported moderate pneumothorax on the left side, devascularization of the left kidney was reported with grade 5 laceration, in addition to irregular contour and cortical edema, all in favour of renal pedicle injury. On the other hand, the right kidney was of normal dimensions with normal cortical thickness. Moreover, ulceration of the spleen with moderate intraabdominal haemorrhage were reported. The bladder was normal without any rupture (Figure 2).
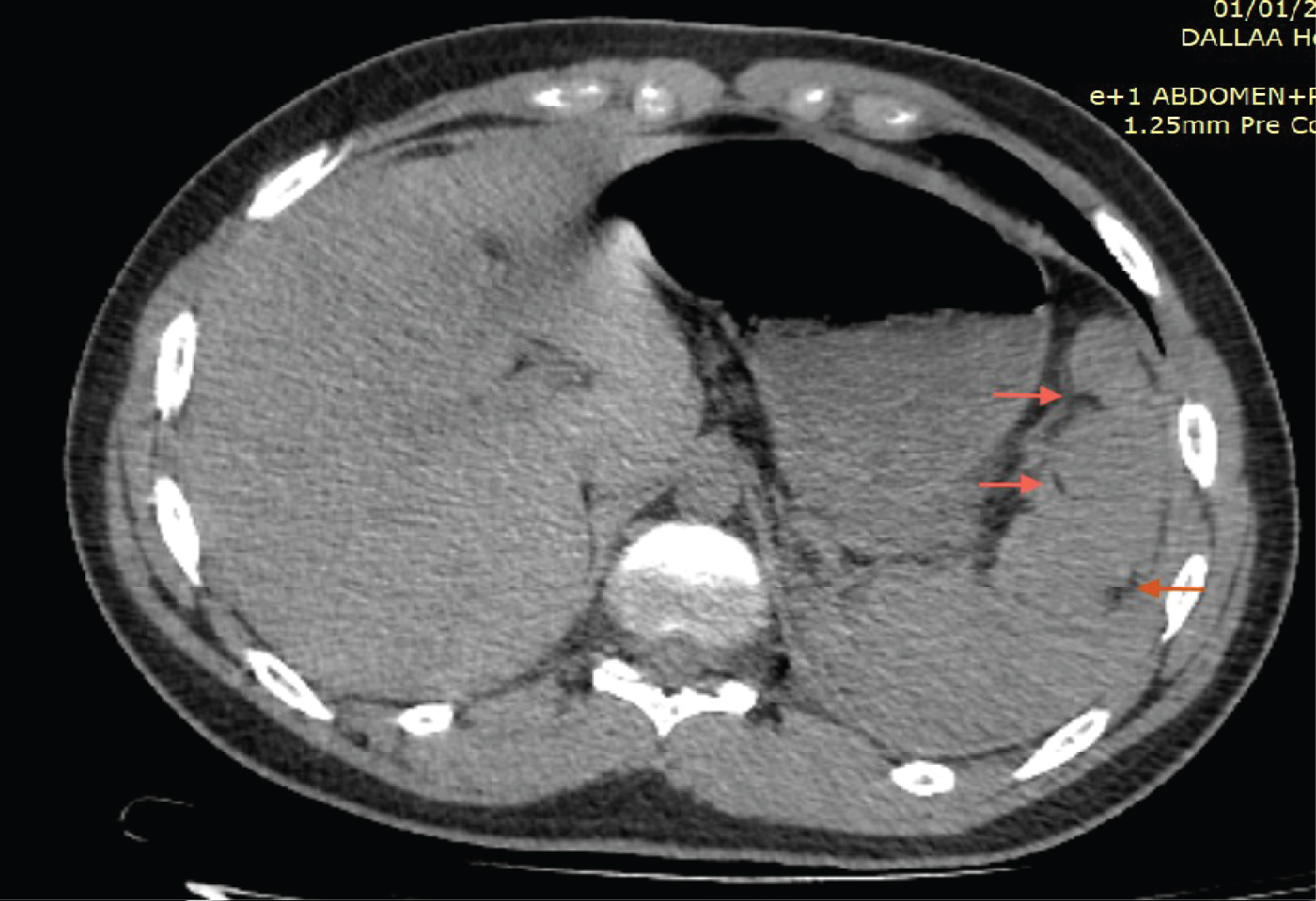 Figure 1: CT abdomen and pelvis without contrast showed splenic laceration.
View Figure 1
Figure 1: CT abdomen and pelvis without contrast showed splenic laceration.
View Figure 1
 Figure 2: CT abdomen and pelvis showed the bladder was normal without any rupture.
View Figure 2
Figure 2: CT abdomen and pelvis showed the bladder was normal without any rupture.
View Figure 2
The patient was admitted for an urgent operation, the left kidney and spleen were removed (Figure 3), and he was given 2 units of pRBCs intraoperatively.
 Figure 3: The left kidney and spleen were removed.
View Figure 3
Figure 3: The left kidney and spleen were removed.
View Figure 3
The postoperative period was eventful as and patient was admitted to the ICU ward postoperatively, his laboratory studies showed decrease in the WBC and stable Hb, however, a positive urine analysis demanded urine culture to be ordered which turned out negative. 3 days later, a chest tube was inserted to relieve the growing pneumothorax.
The patient was transferred to a regular medicine ward on day 8 postoperatively. 9 days postoperatively, the tibial fracture was stabilised intraoperatively by ORIF, then he was discharged home 3 days later.
According to the updated RISC (Revised Injury Severity Classification II) criteria, renal pedicle injuries are classified as grade 5 ASST (American Association for the Surgery of Trauma) renal injuries and only include damage to the major renal artery and/or vein, including laceration, thrombosis, and avulsion. Which, compared to the other grades, imply a more serious injury that poses a life-threatening situation with a greater exploration rate and a lower renal salvage rate [3]. This type of renal lesions represents 1-4% of all renal traumas and therefore is extremely rare [4,5].
However, such lesions have a high mortality rate of 37% [6]. There are no associated risk factors for renal pedicle injury except for trauma as patients with deceleration accidents typically sustain renal vascular pedicle damage [7]. And due to the positioning of the liver with respect to the right kidney, the left renal artery is more susceptible to injury than the right one [7]. Renal pedicle injuries occur in critically damaged patients with numerous system injuries [8]. As a result, the identification and treatment of renal pedicle injuries have fallen behind the management of concomitant injuries, which are frequently life-threatening. The lack of symptoms or indicators that might indicate a renal pedicle injury is another reason for the delay in diagnosis. Hematuria, whether macroscopic or microscopic, is frequently missing and is absent in 24, 38, and 40% [8] of the renal pedicle injuries, making the diagnosis, if it's made, often delayed [9]. Such diagnosis of renal pedicle injury was established with the use of intravenous excretory urography and confirmation by arteriography in the past. But IV urography is of low sensitivity (30% FN) and arteriography is time consuming (takes around 7 hours for result to show).
Therefore, these two modalities are nowadays replaced by CT which defines the extent of intraperitoneal and retroperitoneal trauma [6]. CT findings that are in favour for renal pedicle injury include central retroperitoneal hematoma, which was reported in our case, in addition to absence of parenchymal enhancement or urinary excretion of IV contrast. Moreover, rim sign and abrupt cut of an enhanced renal artery are special in renal pedicle injury [6]. However, angiography may be indicated if CT findings indicate renal perfusion in the presence of other findings suggestive of vascular injuries.
Finally, the treatment of renal pedicle injury involves surgery which can range from total or partial nephrectomy, direct vascular repair, arterial bypass and autotransplantation. In our case, a total nephrectomy was done due to the dislodged state of the left kidney [9]. Timely control of the renal pedicle reduces the need for nephrectomy and facilitates assessment of the extent of damage, and nephrectomy should only be performed in cases of irreparable parenchymal damage [10], like the case of our patient. Complications have been rarely reported in the literature, except for hypertension which has been documented in 57 and 50 percent of renal pedicle injury survivors who had no initial surgical management [8].
Consent was obtained from all involved parties including patient, attending physicians, and radiologist following the discussed case.
The authors of this article declare no conflicts of interest.