Introduction: Although uncommon, breast cancer is the leading cause of cancer related deaths in young women. There are limited studies on the imaging characteristics of malignant breast lesions in women under the age of 45 years. This study highlights the imaging characteristics of malignant breast lesions in young symptomatic patients coming for diagnostic mammography.
Objective: To describe digital mammographic and sonographic features of histopathologically proven malignant breast lesions in young patients under 45 years of age.
Methods: Retrospective analysis of prospectively collected data of 36 young female patients below 45 years of age with breast related complaints undergoing diagnostic imaging at our institute was done.
Results: Out of 36 patients, majority presented with an irregular shaped breast mass with spiculated margins on mammography with suspicious calcifications (n = 16). Majority of them had fine pleomorphic pattern of calcification (n = 11). The final BIRADS assessment category was BIRADS 4b in 4 out of 36 patients, BIRADS 4c and BIRADS 5 in 16 patients each.
Conclusion: Radiologists reporting mammography in young symptomatic women should be aware of the spectrum of lesions found on mammography that might indicate breast cancer, as illustrated in the present study. In particular, there should be a high level of suspicion in young women with breast lumps with microcalcification, with or without a mass or density, in the region of the clinical finding.
Young patients with invasive breast cancer, Breast lump, Focal asymmetry, Mammography
Although uncommon, breast cancer is the leading cause of cancer related deaths in young women. There are limited studies on the imaging characteristics of malignant breast lesions in women under the age of 45 years. This study highlights the imaging characteristics of malignant breast lesions in young symptomatic patients coming for diagnostic mammography.
To describe digital mammographic and sonographic features of histopathologically proven malignant breast lesions in young patients under 45 years of age.
This retrospective descriptive study was conducted in our institute which has a dedicated breast imaging facility between July to November 2022. The subjects in the study were below 45 years of age and were referred from the breast OPD unit in our institute after thorough clinical examination. Thirty-six adult female patients below 45 years of age who had a positive histopathological report for breast malignancy were assessed. All of them underwent diagnostic mammography followed by dedicated breast ultrasound.
These patients underwent digital mammography in two views: The cranio-caudal (CC) and medio-lateral oblique (MLO) views and tomosynthesis in one view (MLO) of both breasts using Digital Mammography Unit (GE Healthcare Senographe Essential 54020/CSEM1/SenoClaire A.6). Additional views like spot-compression view and axillary tail views, etc were taken when needed. They also underwent 3D digital tomosynthesis on the same machine. During tomosynthesis scan, multiple projections of low dose exposure of the breast were acquired at angles of ± 15.6 degrees, while the X-ray tube moved in an arc fashion across the breast. Then, the thin slices were reconstructed to a three-dimensional image. Images were displayed in slice or cine loop mode on dedicated high-resolution work stations. Mammography was followed by dedicated breast ultrasound in all the patients on Supersonic AIXPLORER Multiwave Version 12.2.0808 USG scanner using linear frequency probes between 7.5 and 12 MHz.
The 5 th edition of the American College of Radiology-Breast Imaging Report and Data System (ACR BIRADS) lexicon was used for radiological descriptors. All breast imaging studies were interpreted by a dedicated breast radiologist with more than 10 years of experience in breast imaging.
Thirty-six patients with a histopathologically confirmed diagnosis of breast malignancy were included in the study; four patients with non-malignant biopsy reports (breast abscess/granulomatous/Phylloides/Fibroadenoma) were excluded from the study.
Informed written consent was taken from all the study subjects. No pressure or coercion was exerted on the subjects for participation in the study. Confidentiality and privacy were ensured at all stages.
A total of 36 females aged below 45 years with histopathologically proven breast carcinoma were included in the study. Digital mammography of a total of 72 breasts was done. The mean age of the patients was 38.86 years with ages ranging between 28 and 45 years. Majority of the patients (58%) were in the age range 31-40 years.
ACR breast density B and C showed prominence being 75% and 22% respectively. Out of these 36 patients with carcinoma breast, 35 had an identifiable lesion on mammography (Table 1).
Table 1: Mammographic presentation. View Table 1
Six out of 35 patients had more than one lesion on mammography. The mean of greatest dimension of these lesions was ± cm. Eighteen out of 35 patients had greatest dimension above 3 cm. All the 35 masses were irregular in shape on mammography. Most of the masses had spiculated margins (n = 26), followed by obscured (n = 5), indistinct (n = 2) margins. One patient each had microlobulated and circumscribed margins (Table 2 and Figure 1).
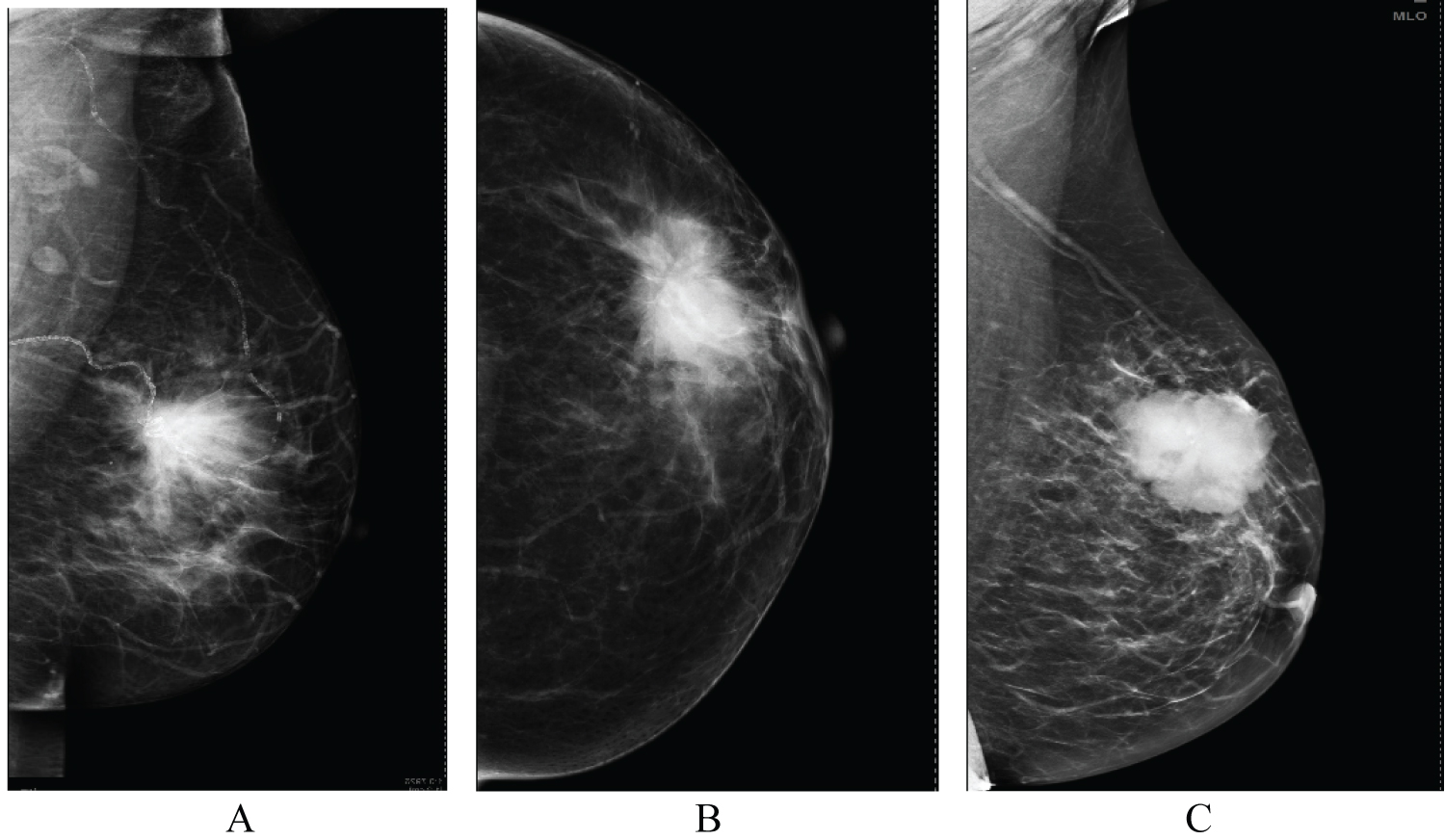 Figure 1: (A-C) MLO and CC views of mammography showing spiculated margins in figure A and B and microlobulated margins in figure C.
View Figure 1
Figure 1: (A-C) MLO and CC views of mammography showing spiculated margins in figure A and B and microlobulated margins in figure C.
View Figure 1
Table 2: Distribution according to pattern of intralesional calcifications (n = 16). View Table 2
Out of 35 patients, 16 patients showed intralesional suspicious calcifications. The commonest pattern of calcifications seen in these patients was of fine pleomorphic type (11 out of 16:68.7%), followed by coarse amorphous (4 out of 16) and fine linear calcifications (1 out of 16) (Figure 2).
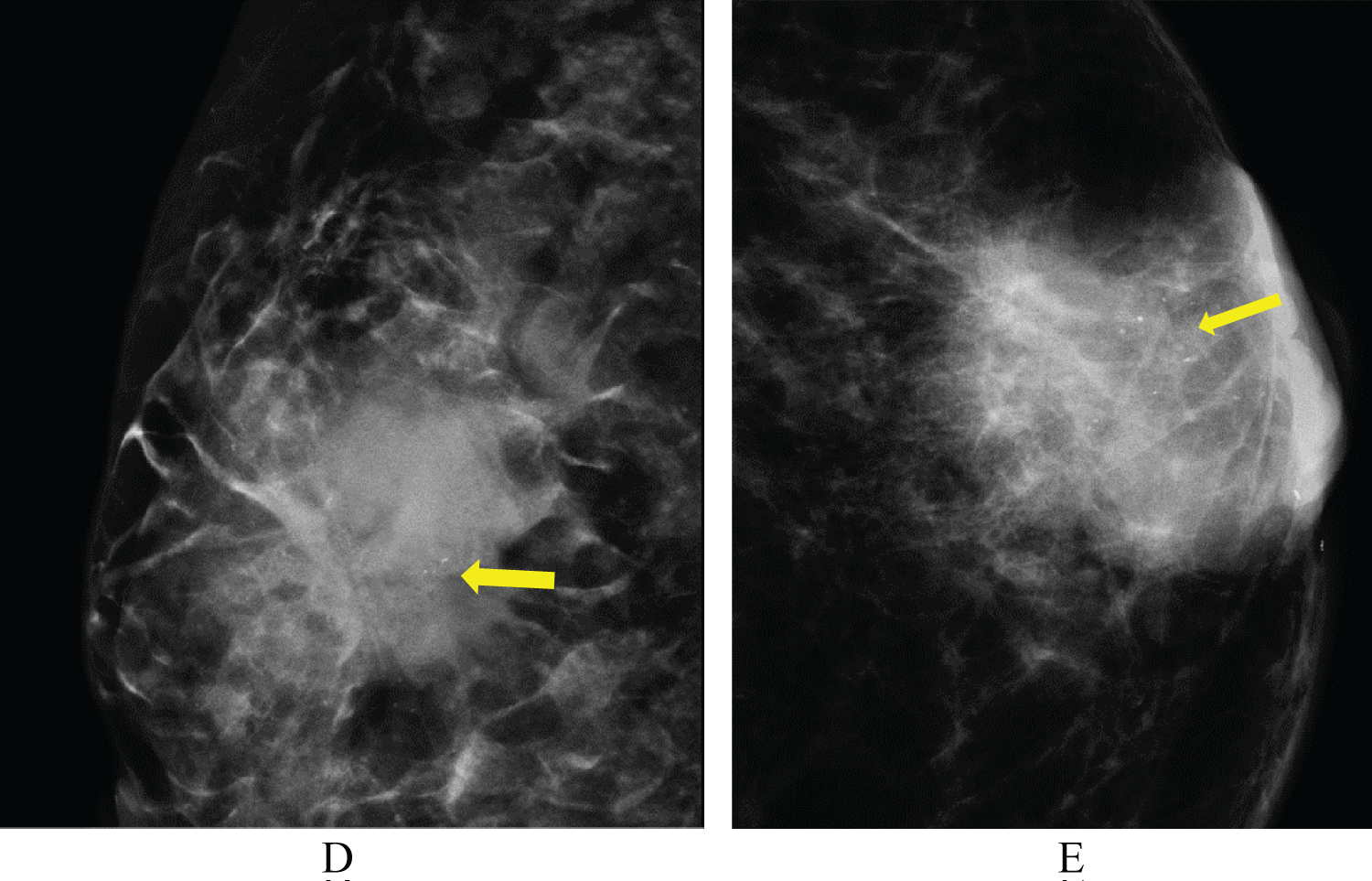 Figure 2: Figure D and E showing the most common fine pleomorphic pattern of calcification in our study (n = 11 out of 16).
View Figure 2
Figure 2: Figure D and E showing the most common fine pleomorphic pattern of calcification in our study (n = 11 out of 16).
View Figure 2
10 patients had architectural distortion, 13 patients had skin & trabecular thickening. Nipple retraction was seen in 4 patients. Axillary lymphadenopathy was a prominent feature in these patients and was seen in 26 out of 36 patients.
Only one patient had with a palpable breast mass had focal asymmetry on mammography in upper outer quadrant of her left breast which on subsequent ultrasonography showed heterogenous breast parenchyma with a small irregular hypoechoic lesion with angulations in at 3 o’clock position. USG guided biopsy was done from the lesion that turned out to be invasive ductal carcinoma (Figure 3).
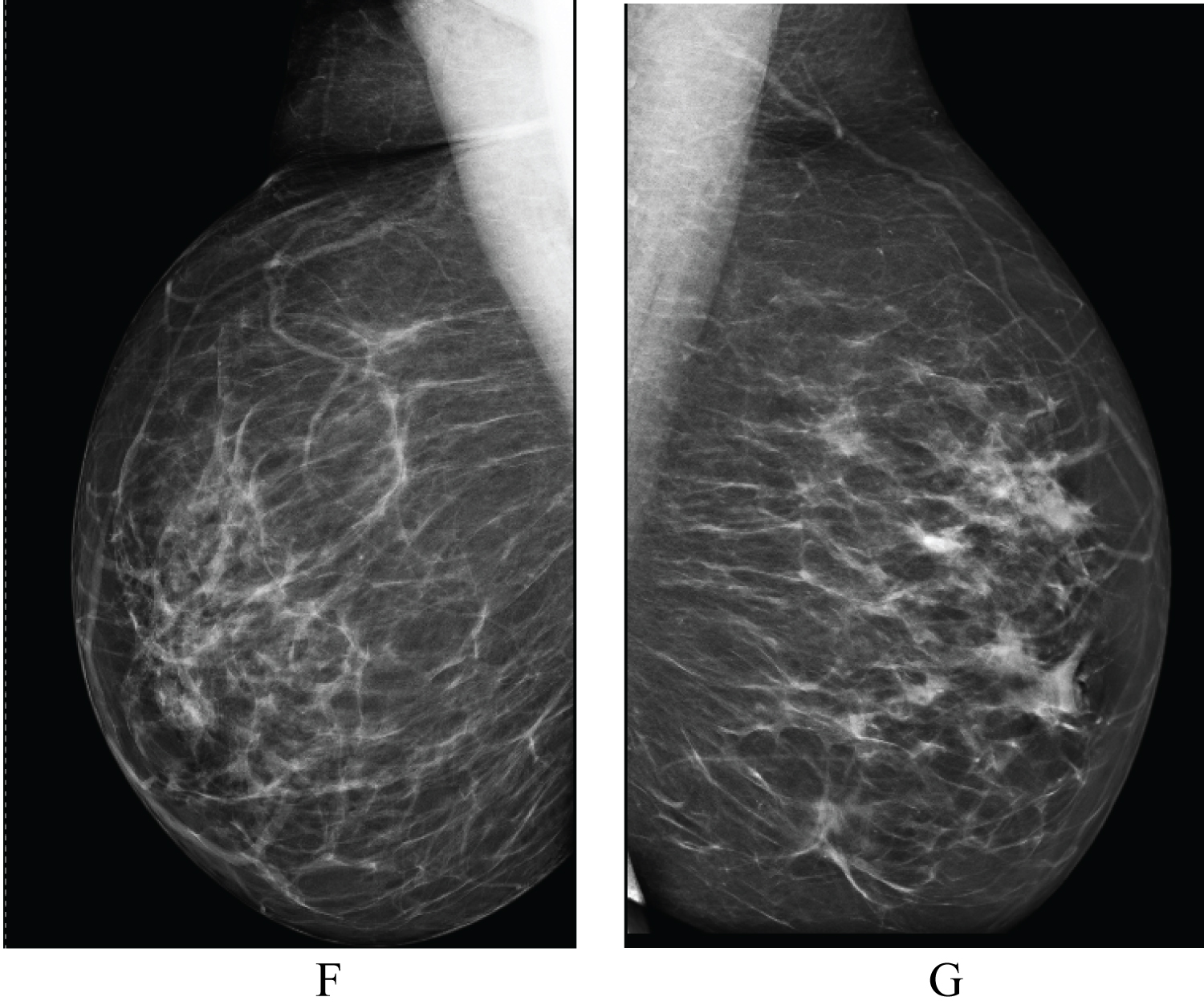 Figure 3: Figure F and G showing MLO views of bilateral breast with focal asymmetry in upper outer quadrant of her left breast which on subsequent ultrasonography showed a small irregular hypoechoic lesion with angulations in at 3 o’ clock position that turned out to be malignant.
View Figure 3
Figure 3: Figure F and G showing MLO views of bilateral breast with focal asymmetry in upper outer quadrant of her left breast which on subsequent ultrasonography showed a small irregular hypoechoic lesion with angulations in at 3 o’ clock position that turned out to be malignant.
View Figure 3
On ultrasonography, all the 35 masses had an irregular shaped lying in anti-parallel orientation with spiculated margins in 20 cases. One patient had a mass with angular margins. 10 out of 35 masses showed posterior acoustic shadowing. Ductal extension, thickening and nodularity was another peculiar feature in these malignant breast masses that was seen in 10 patients (Table 3).
Table 3: Distribution of patients according to final BIRADS assessment category. View Table 3
The final BIRADS assessment category was BIRADS 4b in 4 out of 36 patients, BIRADS 4c and BIRADS 5 in 16 patients each.
The diagnosis of malignant breast lesions in young patients is sometimes more difficult than older women. With the advent of digital mammography including tomosynthesis, these young patients with relatively denser breast parenchyma can be assessed effectively.
Ultrasonography is usually the first imaging modality which is utilised in the evaluation of young females with palpable abnormalities on clinical examination. However, it is inferior to mammography in identifying subtle suspicious calcifications in malignant lesions which may at times cause a delay in appropriate diagnosis and treatment. Therefore, radiologists should be well aware of the suspicious features on ultrasound that prompts detailed breast evaluation with digital mammography in these young patients [1].
The mean age of patients in our study was 38.8 years with 58% of the patients in the age group of 31-40 years. This is consistent with an epidemiological retrospective study conducted in a tertiary health care centre of Northern India by Sandhu DS, et al. [2] who found that the majority of the patients with carcinoma breast were in the age group of 31-50 years. They also emphasized that the mean age of female breast cancer patients in their study was lower compared to the western world, with an average difference of one decade, emphasizing the role of extensive diagnostic work-up in young patients with palpable breast lumps.
All the patients included in our study were symptomatic with some palpable breast abnormality. All of them underwent a thorough clinical examination in dedicated breast OPD unit of our institute. The average duration of presentation as recorded from the database was found to be 3.5 months with majority of patients presenting after 3 month duration. None of the patients had a positive family history of breast cancer or ovarian cancer. These patients did not underwent BRCA gene testing as they were from low socioeconomic strata and had no awareness about carcinoma breast. Nineteen (52.8%) out of 36 patients had a lump in the right breast and 17 cases (47.2%) had it in the left breast.
We observed a prominence of ACR breast density B and C in this study; being 75% and 22% respectively. Out of these 36 patients with histologically proven breast carcinoma, 35 had an identifiable mass on mammography. Only one patient who had swelling in her left nipple presented with focal asymmetry on mammography in upper outer quadrant of her left breast. On subsequent ultrasonography heterogenous breast parenchyma with a small irregular hypoechoic lesion with angulations was seen in subareolar region at 3 o’clock position that later turned out to be malignant on image guided trucut biopsy. This highlights the fact that ultrasonography and mammography work hand-in-hand in correctly labelling focal asymmetry- a probably benign or suspicious finding which needs further evaluation. A prospective study performed by Shetty MK, et al. [3] also reinforces the role of ultrasound in evaluation of focal asymmetries who said that even after a high negative predictive value of sonography for breast cancer in a patient with a focal asymmetric density, biopsy is still indicated when it is new, enlarging, or palpable.
The mean of greatest dimension of breast masses on digital mammography was ± cm. Eighteen out of 35 patients had greatest dimension above 3 cm. All the masses were irregular in shape on mammography. Most of the masses had spiculated margins (n = 26), followed by obscured (n = 5), indistinct (n = 2) margins. One patient each had microlobulated and circumscribed margins. Similar observations were made by Eugênio DS, et al. [4] in their retrospective study on 120 patients, where most of the malignant breast lesions in young patients below 40 years of age had spiculated margins, followed by obscured and indistinct margins.
Sixteen out of 35 patients showed suspicious calcifications in our study. The commonest pattern of calcifications seen in these patients was of fine pleomorphic type (11 out of 16:68.7%), followed by coarse amorphous (4 out of 16) and fine linear calcifications (1 out of 16). Similar observations were seen by Eugênio DS, et al. [4] in their study where fine pleomorphic pattern of calcifications showed prominence.
On ultrasonography, all the lesions were irregular in shape (n = 36) with most of the lesions (n = 20) exhibiting spiculated margins, circumscribed margins (n = 14) and angular margins (n = 1). The lesions were anti-parallel in orientation (n = 30) and showed posterior acoustic shadowing (n = 10). Ductal thickening/nodularity/intraductal extension was an additional feature that was observed in 10 out of 35 malignant breast masses. Final BIRADS assessment category was assigned after performing both mammography and USG in which BIRADS 4b was given to 4 patients, BIRADS 4c to 16 patients and BIRADS 5 to 16 patients out of 36 cases of carcinoma breast.
Radiologists reporting mammography in young symptomatic women should be aware of the spectrum of lesions found on mammography that might indicate breast cancer, as illustrated in the present study. In particular, there should be a high level of suspicion in young women with breast lumps with microcalcification, with or without a mass or density, in the region of the clinical finding. In the present study, microcalcification was frequently a feature of invasive breast cancer in women aged below 45 years. We also recommend to perform breast ultrasound in all the cases after digital mammography to look for additional features like ductal extension and also in cases with focal asymmetry on mammography before labelling it as a benign finding.
Due to short span of study duration, the number of patients examined was limited in our study.
Nil.
Dr. Swasti Pathak and Dr. Neha Singh conceptualized the study and collected data, wrote manuscript. Dr. Gaurav Raj helped in writing and proof reading the manuscript. All authors read and approved the final manuscript.
There are no conflicts of interest.