Background: Myeloma is the most common primary malignancy affecting the skeletal system. Most of the patients are presented and diagnosed late at the disease process, so early detection is very beneficial for patient management and choice of treatment. Multiparametric MRI with the added value of diffusion weighted images together with PETCT had been beneficial for early patient diagnosis, choice of treatment and follow up management after treatment. The study was conducted on 24 patients with bone marrow biopsy and aspiration proven multiple myeloma who also underwent PET-CT within 10 days of each other.
Main body of the abstract: Whole body MRI had high diagnostic accuracy during initial staging and in disease assessment before treatment. After treatment, whole body MRI also showed high diagnostic accuracy in assessing progressive disease activity, while it proved low accuracy in stable disease and regressive disease activity. Whole body MRI showed sensitivity of 87.5%, specificity of 50%, positive predictive value of 78%, and negative prediction value of 67% (p = 0.01). PET had sensitivity of 75%, specificity of 75%, positive predictive value of 85%, and negative predictive value of 60% (p = 0.05). Whole body MRI findings were in agreement with PET-CT in most of the cases.
Short conclusion: During the initial disease assessment, whole body MRI with DWI performed better than PET-CT in detecting small lesions < 5 mm, diffuse (salt and pepper appearance) marrow involvement and total number of marrow lesions, having higher sensitivity and specificity. PET-CT performed better than whole-body MRI in assessment of disease activity before and after treatment. Whole body MRI is recommended for re-assessment if the patient had remission/exacerbation or progressive course of the disease. PET-CT is recommended if the patient had stationary or regressive course of the disease by clinical and laboratory data. When whole body MRI and PET-CT findings of the same patient combined with each other, it is found to have high satisfactory results for patient management, which may be of value to hematologists in assessing the response of bone marrow transplantation.
Whole-body MRI, DWI, Multiple myeloma, Whole-body PET-CT
ASCT: Autologous Stem Cell Transplantation; BMT: Bone Marrow Transplantation; CR: Complete Response; DWI: Diffusion Weighted Image; FDG: Fluorodeoxyglucose; MR: Minimal Response; MM: Multiple Myeloma; PET-CT: Positron Emitted Tomography-Computed Tomography; PD: Progressive Disease; SD: Stable Disease; WB-MRI: Whole Body Magnetic Resonance Imaging
Multiple myeloma is a cancer arising from plasma cells of the bone marrow. It accounts for 10% of hematological malignancies, and about 1% of overall malignancy. The incidence increases with age particularly > 40 years of age. Over production of plasma cells results in deposition of light and heavy chains of monoclonal immune-globulins, which causes expansion of the bone marrow by malignant myeloma cells, where they interact with stromal cells and cause subsequent excess of osteoclast activating factors and suppression of osteoblast activity [1]. Unstopped osteoclastic activity activates the production of various cytokines from stromal cells, which leads to further multiple myeloma clone proliferation [2]. A vicious cycle is set in process, with bone destruction promoting tumor growth and multiple myeloma cells causing bone destruction [2]. It also has tendency to cause immunosuppression, kidney impairment and lytic bone destruction.
The management and diagnosis of multiple myeloma includes good history taking and physical examination, several laboratory tests, bone-marrow aspiration/biopsy, and various imaging studies. The type of treatment to be given is chosen wisely on the basis of the patient’s age, risk factors and comorbidities [2]. Therapy with stem cell transplantation is the treatment of choice in patients under age of 75 years who has no other risk factors or comorbidities [1]. Few of the patients need adjuvant systemic chemotherapy treatment, as well as supportive treatment for myeloma associated organ damage and for the prevention of treatment induced toxicity [1].
The recent consensus statement from the International Myeloma Working Group (IMWG) has recommended whole body MRI for work up of solitary bone plasmactoma and all patients suspected of having asymptomatic or smouldering myeloma [3].
Furthermore, the International Myeloma Working Group (IMWG) includes PET-CT within the standard diagnostic flow chart for both initial and treatment response evaluation in multiple myeloma (Christine, 2020).
The International Myeloma Working Group’s (IMWG) updated criteria for the diagnosis of multiple myeloma include:
Clonal bone marrow plasma cells greater than 10% or biopsy proven bony or extramedullary plasmacytoma and any one or more of the following myeloma-defining events:
Evidence of end-organ damage
Hypercalcemia
Renal insufficiency
Anemia
Bone lesions
Any one or more of the following biomarkers of malignancy:
Clonal bone marrow plasma cell percentage of 60% or greater
Involved: Uninvolved serum free light chain ratio of 100 or greater
Greater than 1 focal lesions on MR imaging studies greater than 5 mm.
The most recent IMWG consensus guidelines issued in 2019 highlighted the importance of using sensitive imaging methods to detect asymptomatic, residual minimal disease and to assess treatment response [4]. These sensitive imaging techniques include low-dose whole-body CT, whole-body MRI, and PET-CT [5]. The 2019 IMWG guidelines also recommended the optimal use of imaging methods at the different disease stages of MM and for different purposes.
The excellent image contrast between normal and diseased marrow on WB MRI with DWI results in superior lesion differentiation compared to conventional and contrast-enhanced MRI sequences (Reem, et al., 2018). Measurement of ADC value has proved to be of value with sensitivity of 90% and specificity of 93% in separating myelomatous marrow lesions from normal marrow [6]. So, WB-MRI with DWI is helpful in monitoring patients with disease remission. The diagnosis of diffuse infiltration on conventional MRI makes it challenging to the radiologist to evaluate for marrow disease activity, but when combined with DWI and ADC measurement, it increases its sensitivity to detect underlying disease activity. However, the variability of ADC values makes it a huge limitation for disease follow up since it is operator and machine dependent. In our study we did not depend on ADC measurements since it its variable from one machine to another, and variable from one patient to another. So we were satisfied by the applicability of the sensitivity of the DWIs with 3D reformatting images.
Although whole-body DWI MRI is considered an emerging sensitive tool for imaging bone marrow, some studies showed several limitations according to its specificity. In lecouvet, et al. [7] and Wu, et al. [8] studies showed that it had high specificity for detection to metastatic bone disease and other causes for bony lesions. Those gave false positive results when these lesions where present in patients with multiple myeloma. So the approach offered by the IMWG of 3 to 6 months follow up of equivocal solitary lesions is a practical solution [6].
PET-CT have shown to be of high prognostic value in patient selection and as a tool to choose treatment dose and maintenance therapy during the post-induction and post-transplant phases in studies conducted Bartel, et al. [9] and Zamagni, et al. [10]. In a study conducted by Hillengass, et al. showed that whole-body MRI results before and after stem cell transplantation could predict overall survival in MM patients. Whilst FDG PET/CT has been shown to be a powerful tool in detecting residual disease, the increased sensitivity of DW-MRI and the capability to detect both tiny deposits and diffuse disease is likely to give it an advantage that merits prospective evaluation [3].
During the initial disease work up of the patients, PET-CT provides a whole body evaluation at one session in a concluded time when compared to the standard survey by whole body X-ray.
According to the new IMWG guidelines, PET-CT when associated with whole body low dose CT is very sufficient for diagnosis regardless whether a corresponding lesion is detected on conventional radiography [11].
Few studies have showed the powerful tool of PET-CT in monitoring therapy response. The study of Lapa, et al., Ulaner, et al. and Dimopolous, et al. [12-14] showed the excellent predictive marker of PET-CT for survival in patients who undertaken chemotherapy prior to stem cell transplant. Likewise, the low or no disease activity by PET-CT following stem cell transplantation is associated with longer disease control. For these reasons, the IMWG strongly recommends PET-CT as the preferred imaging technique to evaluate response to therapy in MM.
Several studies have showed the powerful tool of PET-CT and MRI in assessing disease activity after stem cell transplantation. In a study performed by Derlin, et al. [15], PET-CT showed post-treatment sensitivity of 54.6%, specificity of 82.1% and overall accuracy of about 65.5%. Although these results may show the PET-CT has low sensitivity than it seems, but it showed valuable prognostic information as regards long disease-free survival time.
Derlin, et al. [15] then evaluated 31 patients who had undergone both PET-CT and whole-body MRI after stem cells transplantation, and concluded that although PET-CT had lower sensitivity that whole-body MRI, the former had demonstrated greater overall accuracy in determining remission status than whole-body MRI (74.2% versus 51.6%). Derlin, et al. [15] stated that the higher accuracy of PET-CT in this setting was that the MRI had high false positive results due to metabolically in-active persistent marrow lesions.
Another study performed by Zamagni, et al. had concluded that PET-CT is very valuable in predicting survival rate till 3 months after stem cell transplantation.
Several other studies had showed the usefulness and utility of whole-body MRI in post stem cells transplant evaluation of MM patients. In a study conducted by Bannas, et al. [16] showed that the laboratory tests where concordant with whole-body MR results in 78.8% of the cases, and showed that whole-body MRI had sensitivity of about 63.6%. Hillengas, et al. also used whole-body MRI in his study and concluded that MRI was highly sensitive in detecting both focal and diffuse pattern of marrow involvement, which could be helpful in assessing overall survival rate of the patient post-treatment.
Alberto, et al. [3] had made a study using whole-body MRI with the use of DWI, and stated that DWI is a powerful tool in detecting both tiny deposits and diffuse disease, while it need further prospective evaluation in its sensitivity in detecting residual disease.
The aim of this study is to monitor changes in magnetic resonance imaging before and after bone marrow transplantation and correlate it with PET-CT findings to assess treatment response and survival in multiple myeloma patients.
Our study was done at the Radiology Department of Maadi Armed Forces Medical Compound, Ain Shams University hospitals and Dar Al-Fouad Hospital. Informed consent was taken from all patients as required.
We conducted our study on 24 patients (16 males and 8 females) with multiple myeloma who performed whole-body MRI and PET-CT from March 2020, and established a study registry. The registry had included eligible patients according to our inclusion and exclusion criteria.
Inclusion criteria included: 1. Patients who were diagnosed with MM at the above institutions with disease activity of > 30% by bone marrow aspiration. 2. Patients who underwent bone marrow transplantation at our institutions. 3. Patients who performed at least one whole-body MRI or PET-CT before and after transplantation.
Exclusion criteria included: 1. Patients who are not fitting the diagnostic criteria according to IMWG. 2. Patients who had another known malignancy with metastasis. 3. Patients contra-indicated for MRI (claustrophic patients, patients with intra-cerebral coils and cochlear implants). 4. Patients who refused to perform the exam according to their will.
Our study was performed on 1.5 tesla MRI machine (siemens) and PET-CT on 16 MDCT (siemens).
The whole-body MRI sequences consisted of un-enhanced whole body coronal T2 (TSE), whole body coronal T2 FAT SAT, whole body coronal T1 (VIBE), whole-spine sagittal T2 & T1 (TSE), axial whole body DWI at two different b-values (b50 and b800) using head and neck coil, body surface coil and special body coil. Multiple coils were applied to cover the whole body (skull to feet). No contrast was given at our study.
Patients were prepared for the PET-CT by eating low glucose diet the day before scanning and fasted from mid-night. The patients were given 18 FDG IV 45 minutes before scan. IV and oral contrast was given during the PET scan. The field of view was from the skull to feet (parameters were 120 kVp; 150 mAs; collimation, 16 × 1.5 mm).
In each case, we collected the patient age, sex and myeloma sub-type. The results of the bone marrow aspiration and laboratory results were correlated with the results of the PET-CT and whole-body MRI to assess image accuracy.
The bone marrow aspiration was obtained from the posterior iliac spine in all cases by the same hematologist. Disease activity was defined as > 30% plasma cells activity at bone marrow aspiration.
Whole-body MRI and PET-CT was taken during initial workup before bone marrow transplantation, and follow up by PET-CT and whole-body MRI was done at 1, 3 and 6 months after bone marrow transplantation. In all follow up cases, bone marrow aspiration was performed within 10 days after imaging.
A hematologist evaluated the clinical responses of the patients using the IMWG criteria and bone marrow disease activity by bone marrow aspiration. The IMWG criteria are based on changes in M-protein as a major indicator for response assessment. The response categories include complete response (CR), stable disease (SD), and progressive disease (PD). Complete response is considered when marrow plasma cells by bone marrow aspiration is < 30%, while stable and progressive diseases are considered by plasma cells is > 30% by bone marrow aspiration and levels of M-protein. The clinical response was then correlated with the radiologist to assess imaging accuracy.
Five imaging patterns of marrow involvement have been described in multiple myeloma in the study performed by Dimopolous, et al., [17]. We used similar imaging patterns in our study. The 5 patterns are: ( 1 ) Normal appearance of the bone marrow despite minor microscopic plasma cell infiltration, ( 2 ) Focal marrow involvement, ( 3 ) Homogeneous diffuse infiltration, ( 4 ) Combined diffuse and focal infiltration, and ( 5 ) ‘Salt and pepper’ pattern with inhomogeneous bone marrow.
The size and number of the bone marrow lesions were assessed as a target lesion. While the diffuse (salt and pepper pattern) was considered non-target lesion.
Statistical Package for Social Sciences (SPSS) was used for data administration and analysis, version 23. The Kappa agreement was used to detect the agreement between MRI diffusion and PET-CT findings with bone aspiration results. The significance level of p = 0.05 indicating statistical significance.
The PET-CT and whole-body MRI of the 24 patients were correlated with bone marrow aspiration results, where active disease was defined as > 30% plasma cells. The results were analyzed in two pairs, one for whole-body MRI and the other for PET-CT (Table 1 and Table 2), after 6 months of treatment.
Table 1: Whole-body MRI with DWI findings of activity found at bone marrow aspiration after treatment (n = 24). View Table 1
Table 2: PET positivity with disease activity on bone marrow aspiration after treatment (n = 24). View Table 2
The results of whole-body MRI and PET-CT together with the bone marrow aspiration results were then correlated with each other to assess the concordance of PET-CT and whole-body MRI and were studied separately at the discussion section.
In our study, the 24 patients showed the following treatment response after 6 months of stem cell transplantation:
8 patients showed complete response.
11 patients showed stable disease.
5 patients showed progressive disease.
Table 1 showed sensitivity of 87.5%, specificity of 50%, positive prediction value of 78%, negative prediction value of 67% and overall accuracy of about 75% (p = 0.01).
Table 2 showed sensitivity of 75%, specificity of 75%, positive prediction value of 85%, negative prediction value of 60% and overall accuracy of about 75% (p = 0.05).
The patient statistics in our study were similar to the expected population of myeloma patients with mean age of 60 years.
Few studies were done to assess the sensitivity and specificity of PET-CT in detecting disease activity before and after treatment. Studies of Gairiani, et al. [18] and Cavo, et al. [19] showed wide range of sensitivities (54-92%), which is near to our results (sensitivity of 75% in our study). However, in our study, the relatively low sensitivity was due to performing the study in different stages of treatment. The false positive cases were assessed and showed that it may be due to marrow reconversion and presence of concurrent bone disease during the exam.
Whole-body MRI showed sensitivity of 85% in our study. Our study was nearly concordant with the study of Ho, et al. [20] which showed sensitivity range of 70-89%, depending on the stage of the disease. Our study and Ho, et al. study showed the increased sensitivity of whole-body MRI in detecting diffuse marrow involvement of MM which wasn’t detected during the PET-CT study. The use of DWI MRI increased the sensitivity to detect marrow lesions. In our study we realized that active marrow lesions showed diffusion restriction. However, the focal marrow lesions seen after treatment did not resolve, but showed few of the treated patients showed no DWI restriction of previously restricted marrow lesions. This gave a low specificity in our study of about 50% and overall positive prediction value in assessing post-treatment cases, as well as causing high false positive cases at the post-treatment evaluation. The specificity in our study was significantly reduced when assessing post-treatment response, but was nearly similar to the study of Ho, et al. [20] and Shrott, et al. [21] in assessing marrow involvement during initial workup and before treatment.
These results where concordant with the NCCN guideline and IMWG consensus statement that routine WB- MRI is not recommended for the evaluation of treatment response (Figure 1 and Figure 2).
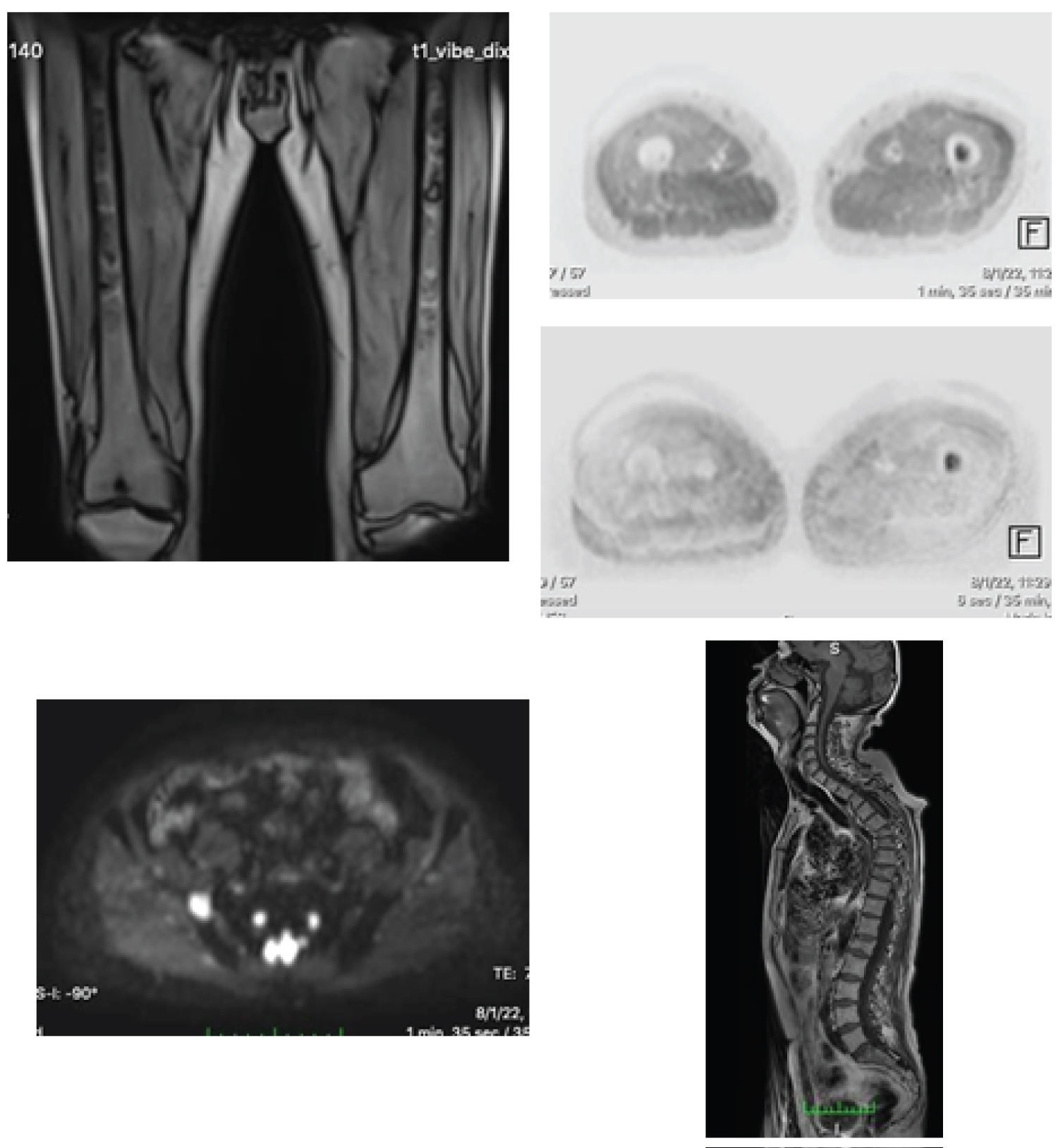 Figure 1: 66-years-old patient performed BMT. Recurrent active lesions are seen at the left mid-femoral shaft and right iliac bone. Conventional T1 image of the whole spine showed previous treated lesions with no diffusion restriction denoting in-active tumor activity.
View Figure 1
Figure 1: 66-years-old patient performed BMT. Recurrent active lesions are seen at the left mid-femoral shaft and right iliac bone. Conventional T1 image of the whole spine showed previous treated lesions with no diffusion restriction denoting in-active tumor activity.
View Figure 1
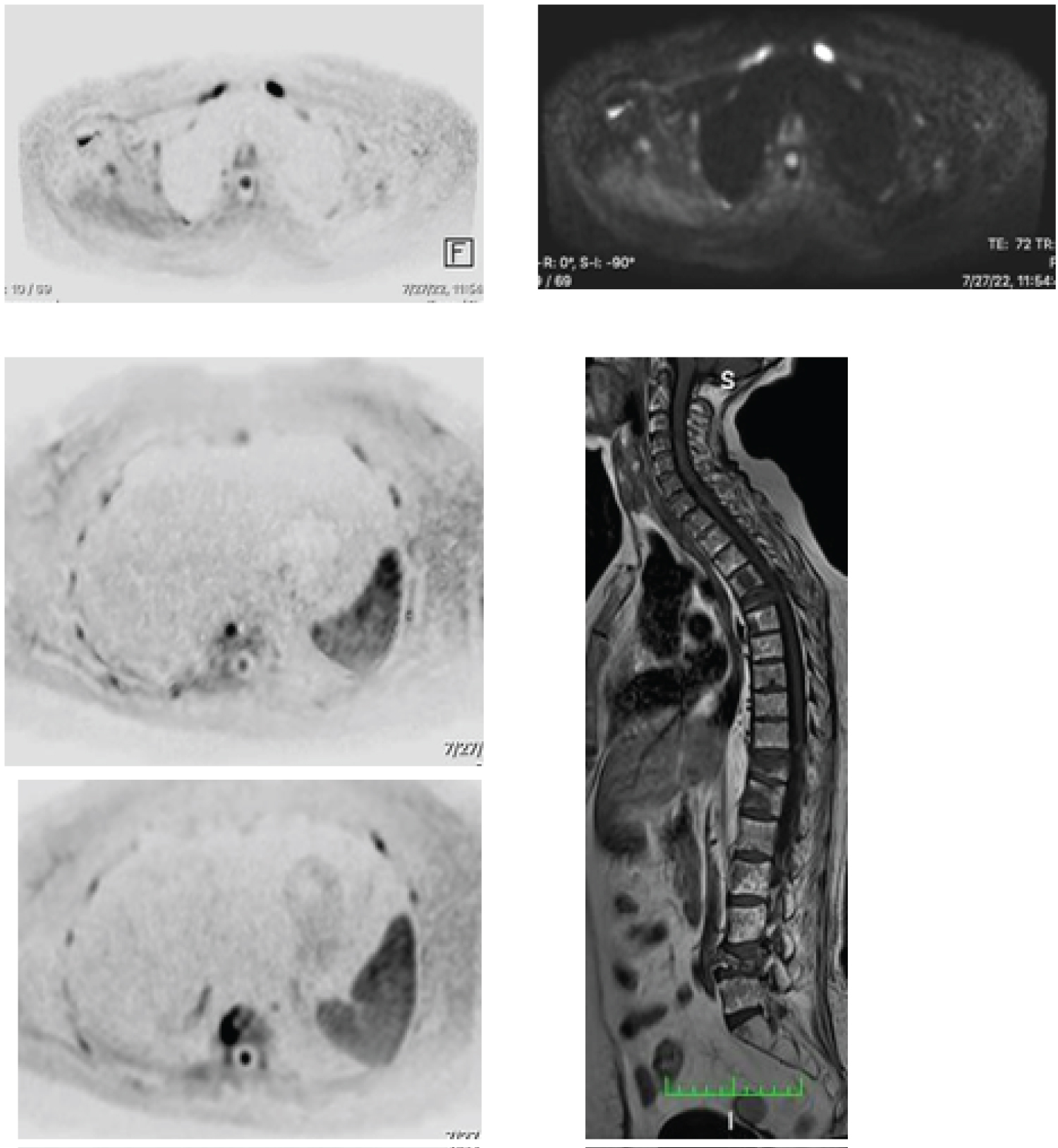 Figure 2: 63-year-old patient showing ill-defined marrow signal at the conventional MRI images, with restricted diffusion at the DWI series (done at two different b values), and laboratory criteria of active MM disease, denoting active marrow lesions.
View Figure 2
Figure 2: 63-year-old patient showing ill-defined marrow signal at the conventional MRI images, with restricted diffusion at the DWI series (done at two different b values), and laboratory criteria of active MM disease, denoting active marrow lesions.
View Figure 2
In our study we assessed the agreement of whole-body MRI with the PET-CT findings. During the initial work-up, whole-body MRI proved to have higher sensitivity to detect marrow lesions than PET-CT. Whole-body MRI also showed its increased sensitivity when using the DWI tool. The increased sensitivity of whole-body DWI MRI aided to detect other causes of marrow diseases concurrent with the patient disease of MM, which led to its reduced specificity in evaluating MM patients specially post-treatment.
In after treatment cases, PET-CT was highly sensitive and specific in evaluating active and treated marrow lesions. While these treated marrow lesions were also seen at the whole-body MRI, the whole-body MRI with diffusion showed no restriction at DWI which was concordant in 50% of the cases that showed no metabolic activity in PET-CT (Figure 3).
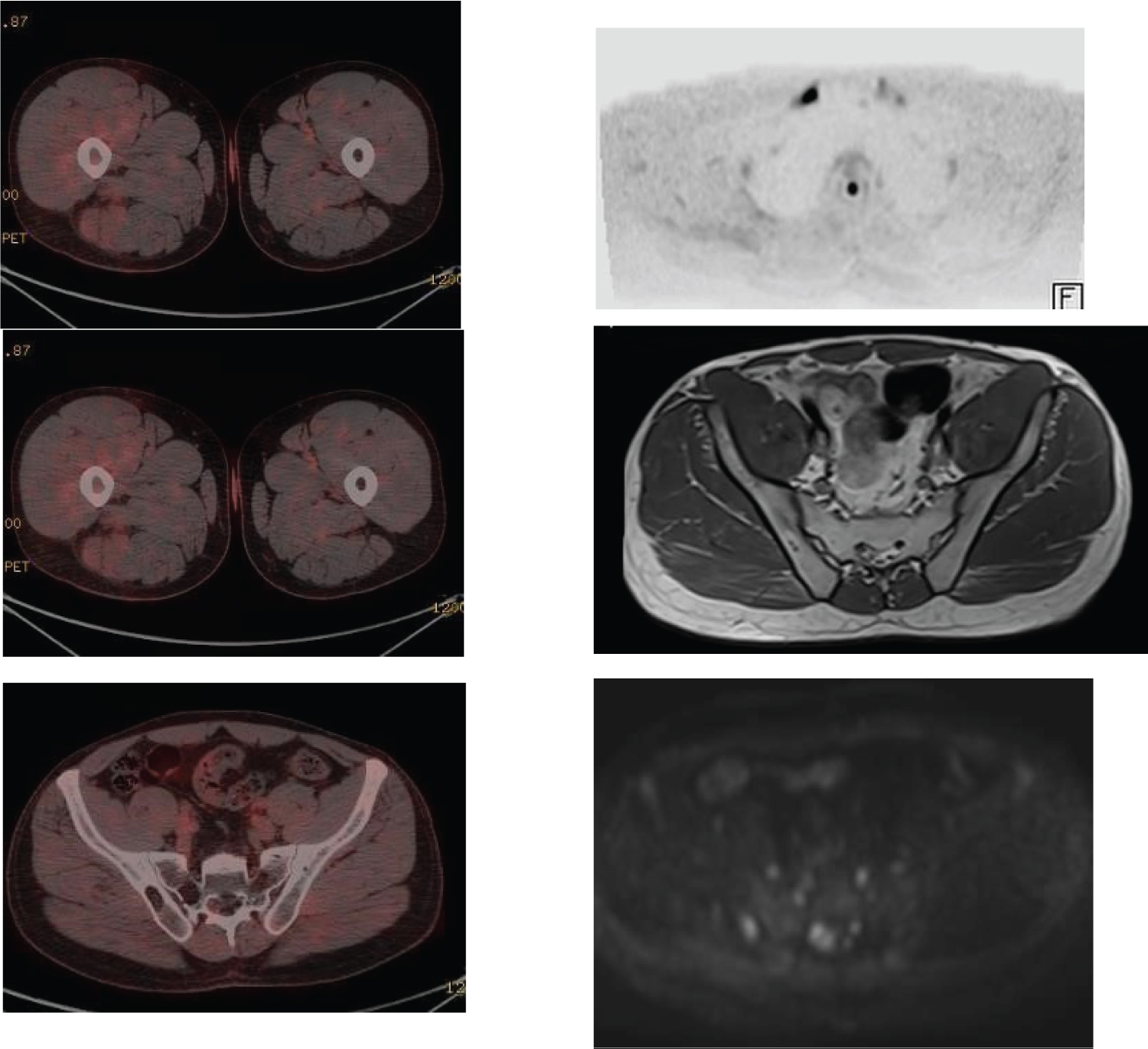 Figure 3: 35-year-old patient treated with stem cells BMT. The MRI showed diffusion restriction at the proximal 1/3 of the right clavicle, right S2/3 and right mid-femoral shaft denoting active lesions. PET-CT of the same patient showed small active tumoral uptake at the mid-femoral shaft.
View Figure 3
Figure 3: 35-year-old patient treated with stem cells BMT. The MRI showed diffusion restriction at the proximal 1/3 of the right clavicle, right S2/3 and right mid-femoral shaft denoting active lesions. PET-CT of the same patient showed small active tumoral uptake at the mid-femoral shaft.
View Figure 3
In patients with progressive disease and newly developed marrow lesions, whole-body MRI was sensitive in detecting the newly developed small marrow lesions, especially those < 5 mm. These small lesions wasn’t detected by the PET-CT. Whole-body MRI with DWI also was more sensitive than PET-CT in detecting diffuse marrow disease (salt and pepper type). However although the PET-CT showed more specificity in detecting active post-treatment marrow lesions, both the PET-CT and whole-body MRI showed low sensitivity and specificity, respectively, in assessing post-treatment diffuse marrow involvement (Figure 4).
 Figure 4: 46-year-old patient with MM treated with BMT showing diffuse marrow involvement, showing active disease by bone marrow aspiration, yet no metabolic activity by PET-CT.
View Figure 4
Figure 4: 46-year-old patient with MM treated with BMT showing diffuse marrow involvement, showing active disease by bone marrow aspiration, yet no metabolic activity by PET-CT.
View Figure 4
However, combined imaging modalities using PET-CT and whole-body MRI with DWI during initial work-up and during disease of the patient progression after treatment may yield high sensitivity, specificity, positive prediction value and high accuracy.
We had several limitations in our study. First that, we did not have a high variety of MM patients performed stem cells transplantation to assess. Second, few of the patients had previously treated with chemo-therapy. Third, the most of our patients had red marrow reconversion (due to anemia) which causes increased marrow FDG false activity, giving false impression of diffuse involvement. Fourth limitation was that the whole-body MRI is time consuming for the patient which caused patient discomfort. Another limitation was that the patients who had other benign marrow lesions (benign bone lesions, osteoarthritis and osteoporosis) which showed diffusion restriction just like the myelomatous lesions.
We conclude in our study that whole-body MRI provided excellent soft tissue contrast and better characterization of myelomatous lesions, especially in the assessment of diffuse marrow infiltration during the initial disease work-up. Although few of our patients showed no restriction of the myelomatous lesions at DWI after treatment, which was concordant with PET-CT, still has poor specificity in detecting treatment response and survival rates. On the contrary, PET-CT provided better overall assessment of treatment response after stem cells transplantation and provided better long term treatment outcome and survival rates.
We recommend the combined use of whole-body MRI with the use of DWI and PET-CT during initial work-up establishing good patient disease overview, and follow up post-treatment by PET-CT. We also recommend to not routinely using whole-body MRI during follow up except in patients with serological evidence of increased/progressive disease activity to detect newly developed lesions not sensitive enough to be detected by PET-CT.
Future prospective studies using whole-body MRI with DWI and ADC values is also recommended and may be considered a promising tool in case of standardizing reference values for ADC map.
The study protocol was approved by the Research Ethics Committee of Faculty of Medicine at Ain Shams University on 22/9/2019 under the number of FMASU M D 316/2019.
All patients included in this study gave written informed consent for data publishing contained within this study.
The datasets used and analyzed in this study are available from the corresponding author upon reasonable request.
The authors declare that they have no competing interests.
The research was self-funded by the authors.
SN was involved in data collection, validating the results obtained by the MRI and original manuscript draft writing. HAK, MHK, WAH and SME were involved in manuscript review and editing. All authors have read and approved the manuscript.
Not applicable.