A 46-year female with long-standing disabling low backache with pain radiating to the right lower limb, pain at tail bone not allowing her to sit, sleep and stand for the last 3 months with acute exacerbation since 3 days were diagnosed as degenerative lumbar disc disease with right L5/S1 radiculopathy and coccydynia not responding to medical management and treated with minimally invasive procedures - CT guided ganglion impar block. CT showed a right lumbar nerve root block at L5/S1 level, leading to immediate and complete pain relief with a follow-up of 10 months.
Lumbar disc disease, Radiculopathy, Coccydynia, Computed tomography
The wear and tear of the lumbar intervertebral disc is known as lumbar disc degeneration, and it primarily affects the L3-L4 and L4-S1 vertebrae. Osteophytes, a loss of disc space, disc bulging, compression, and irritation of the nearby nerve root are all possible consequences of lumbar disc degeneration disease. It starts with tiny tears in the disc's annulus and progresses to a drop in the water content of the nucleus pulposus. Discogenic pain, radical pain, muscle weakness, and cutaneous manifestations are the clinical presentations connected to lumbar disc degeneration and lumbosacral nerve damage [1].
A 46-year female, working as a teacher, was admitted with long-standing disabling low backache with pain radiating to the right lower limb and pain at tail bone not allowing her to sit, sleep and stand for the last 3 months with acute exacerbation for 3 days. Previously, she consulted many doctors who investigated and treated her with NSAIDS providing minimal to no change in her condition. Her baseline blood investigations didn’t reveal any significant abnormality. Her MRI lumbo-sacral spine and Coccyx revealed a right postero-lateral annular tear at L5/S1 level without any neural foraminal compromise. No considerable abnormality at Coccyx Computed Tomography (CT) of Coccyx also revealed no significant abnormality. Because of severe lumbar region pain (score of 8 on the numeric pain rating scale) radiating to the right lower limb, severe pain (score of 8 on the numeric pain rating scale) at the coccyx region not correlating with her blood investigation results and imaging findings, the treating team converged to the diagnosis of degenerative lumbar disc disease with right L5/S1 radiculopathy and coccydynia. After discussing risks and benefits with the patient and her husband, the treating team offered her minimally invasive interventional procedures to relieve her pain in the lower back, right lower limb, and coccydynia, as she was not responding to conservative medical treatment for the last 3 months. Two procedures were planned:
CT guided ganglion impar block with trans discal technique
CT guided the right lumbar nerve root block at L5/S1 level
Positioning the needle under CT guidance is straightforward because the location of the needle tip and the anatomic structures can be directly visualized during nerve root injection and ganglion impar injection. A short planning CT allows for measuring the distance between the planned insertion point on the skin and the target and choosing the appropriate needle for the patient.
After essential pre-procedural work up, CT-guided right L5/S1 nerve root block and CT-guided ganglion impar blocks were done in a prone position. After precise positioning of 22G LP needles at desired locations: 1 ml (40 mg) triamcinolone, 3 ml of 0.5% bupivacaine, 2 ml of 2% xylocaine, and 0.5 ml contrast neurolysis mixture was injected for right lumbar nerve block and ganglion impar region. Sterile dressing was applied at skin entry sites.
She was immediately relieved of pain on the CT table with a numeric pain rating scale of 8 (severe pain) in pre-procedure and 0 (no pain) in immediate post-procedure, at lumbar region and tail bone region. She was discharged the next day with advice for checking her blood sugar levels regularly, follow up schedule without any oral NSAIDS. She could comfortably walk, sit and pursue her profession as a teacher from the second post-procedure day. She continues to be pain-free at 10 months of follow-up. CT guided ganglion impar block with transdiscal technique images were showed in Figure 1 and Figure 2 showed the CT guided right lumbar nerve root block at L5/S1 level.
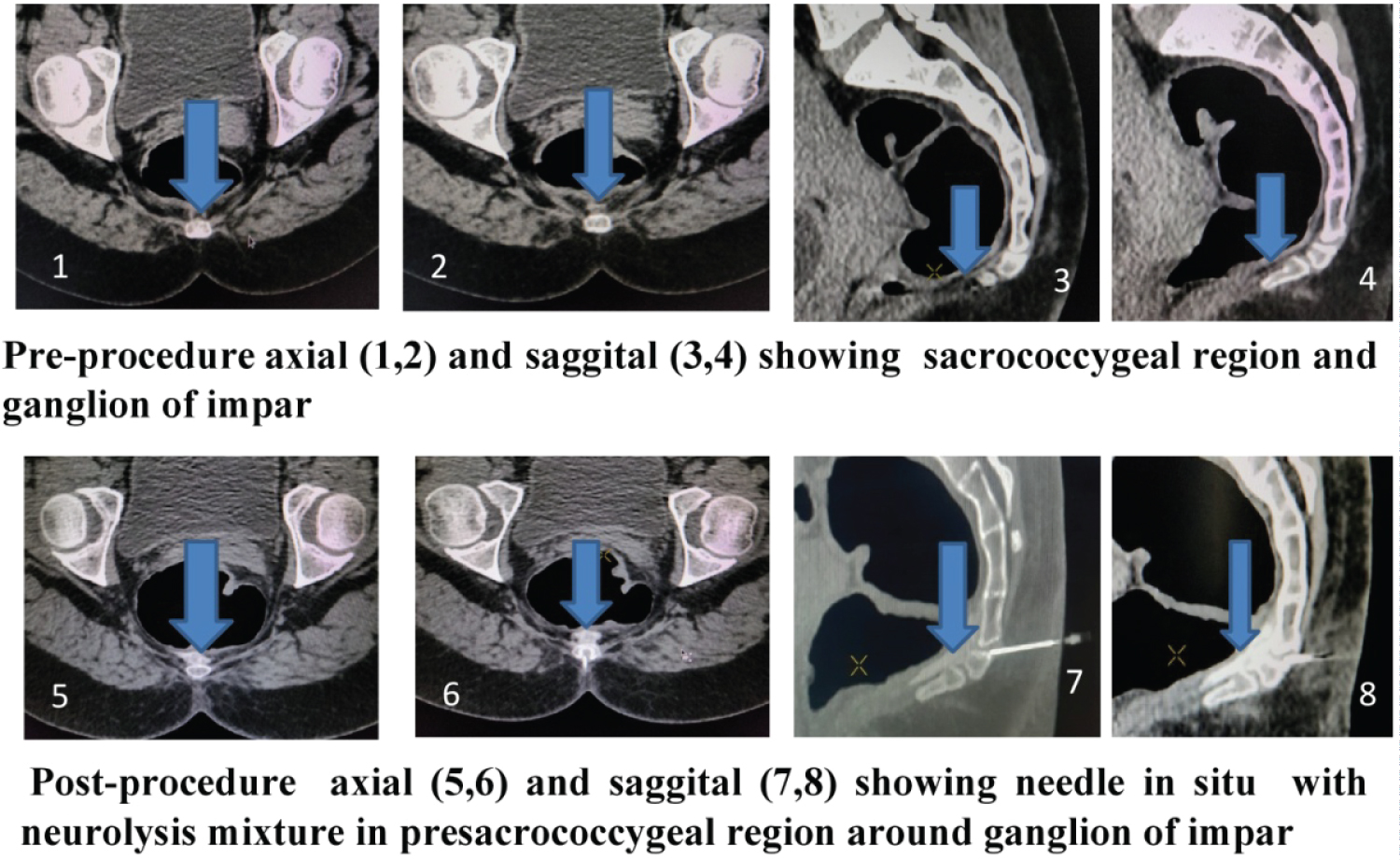 Figure 1: CT guided ganglion impar block.
View Figure 1
Figure 1: CT guided ganglion impar block.
View Figure 1
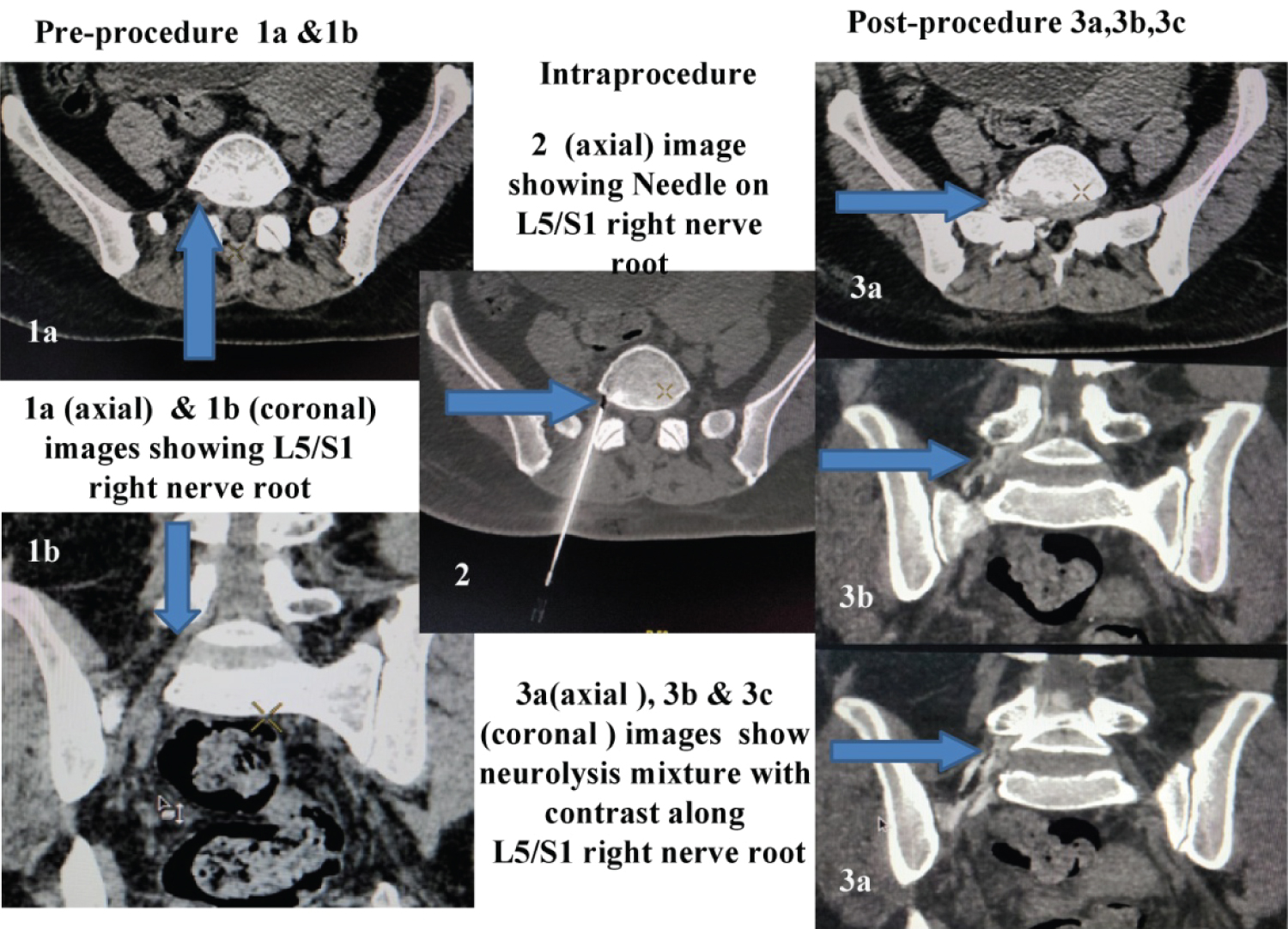 Figure 2: CT guided L5/S1right nerve root block.
View Figure 2
Figure 2: CT guided L5/S1right nerve root block.
View Figure 2
Coccydynia is a clinical condition with varied etiology, and no definitive diagnostic criteria exist [2]. The ganglion impar is a retroperitoneal structure at the level of the sacrococcygeal junction, which marks the termination of the paravertebral sympathetic chain. A ganglion impar block is usually considered to treat coccydynia, which is non-responsive to other conservative treatments. Pain relief is achieved by the blockade of nociceptive and sympathetic fibers [3]. The success of ganglion impar block is an effective treatment modality for long-term relief from coccydynia. The technique used in our case was the transdiscal technique, which is considered a relatively safe approach. The trans-sacro-coccygeal approach adopted in our case is better than the classical and paramedian approach to the ganglion. It is a technically feasible method that is easy to learn and perform. There is minimal risk involved in this technique compared to surgical treatment. The complications of this technique are neuritis and unintentional injection of the neurolytic agent into the rectum, which can be avoided by precise positioning of the needle under CT guidance. Back pain is among the most common medical problems associated with high socioeconomic costs. Imaging-guided lumbar nerve root blocks are a safe and effective minimally invasive method to evaluate where the back pain is originating from and to treat patients with radicular pain with infiltration of corticosteroids. The nerve blocks can lead to significant relief of back pain. CT-guided lumbar nerve root block is a safe procedure that allows direct visualization of the nerve root and the needle tip and the distribution pattern of the injected neurolysis mixture along with contrast.
CT-guided Ganglion impar block and lumbar nerve root blocks are minimally invasive interventional procedures for managing coccydynia and low backache with lumbar radiculopathy in an appropriate clinical setting. CT guidance during the procedures ensures better accuracy, safety, and favourable response for pain relief.
The authors would like to thank the management of Medicover Hospital, Visakhapatnam.
Nil.
Nil.