Background: There were neither specific therapeutic drugs for treatment COVID-2019 nor effective permanent vaccines. Therefore, it is essential to detect early the disease and immediately isolate the infected person from the healthy population. In severe cases with high fever and cough, chest computed tomography (CT) can lead to rapid diagnosis, and to early control of potential transmission. This is usually needed in patients with suspected disease, for the hospitals or communities lacking nucleic acid testing kits. Our study aimed to compare the accuracy of both chest CT and reverse transcriptase polymerase chain reaction (RT-PCR) results in diagnosing COVID-19 infection in clinically suspected patients. Also, to determine the correlation between CT Severity Scores (CTSSs) and RT-PCR results.
Results: We enrolled 200 patients clinically suspected with COVID-19 between 1 November 2021 and 31 March 2022. All patients had done Chest CT and RT-PCR tests at a time interval of no longer than 7 days between the two tests. The exclusion criteria include pre-existing chronic respiratory illness like pulmonary tuberculosis, chronic obstructive pulmonary disease (COPD), interstitial lung disease and time interval between chest CT and RT-PCR more than 7 days (> 7 day). Severity scores (CTSSs) and COVID-19 reporting and data system (CO-RADS) were used to detect severity of lung involvement in the chest CT of patients. Computed tomography specifically, with typical radiologic features, (as bilateral distribution ground-glass opacities, consolidation in a peripheral distribution, interlobular septal thickening, and crazy-paving pattern) can be considered cornerstone for COVID-19 diagnosis. The CT scoring bases (CTSS sand CO-RADS) were accurate in differentiation between mild/moderate and severe disease. The performance of the RT-PCR from various respiratory specimens is modest. In our study, there was a positive CT finding in the negative RT-PCR patients.
Conclusions: Chest CT can predict COVID-19 severity by showing the percentage of lung involvement and hence give an idea about the prognosis of the disease. However, RT-PCR is subject to false-negative results because it can easily be affected by multiple factors, such as insufficient cellular material for detection and improper extraction of nucleic acids from clinical materials.
COVID-19, Chest computed tomography, Reverse transcriptase polymerase chain reaction, Sensitivity, CTSS
COVID-19: Coronavirus Disease 2019; CT: Computed Tomography; ICU: Intensive Care Unit; SD: Standard Deviation; CTSS: CT Sensitivity Score; CO-RADS: COVID-19 Reporting and Data System; RTPCR: Reverse Transcriptase Polymerase Chain Reaction; COPD: Chronic Obstructive Pulmonary Disease; GGOs: Ground Glass Opacification; ARDS: Acute Respiratory Distress Syndrome
Coronavirus disease has multiorgan involvement with various extra- pulmonary manifestations [1,2]. Pneumonia is the most frequent severe manifestation of the disease with fever, dry cough, shortness of breath, and fatigue up to acute respiratory distress syndrome (ARDS) and death [3]. Chest CT is recommended in suspected COVID-19 cases, for both initial evaluation and follow-up [4].
Chest CT scoring bases (CTSS and CO-RADS) were used for classification and staging of COVID-19 together with disease progression. Luo, et al. [5] evaluated the severity of lung involvement assessed by admission CT scan and its association with clinical outcomes in COVID-19 patients.
The severity of lung involvement was assessed by CT severity score developed and based on lung involvement percentage for each patient [5% or less; 5-25%; 26-50%; 51-75%; > 75% = 1-5 respectively] [6].
The RT-PCR test considered the standard for the diagnosis of COVID-19, but in some cases, it can have false-negative results in the early stages of the disease. The RT-PCR test has varying sensitivities ranging from 28% to 85% [7]. CT findings have confirmed the diagnosis in a number of patients with an initial false-negative RT-PCR result [8]. False negative results are common in RT-PCR test in early stage of infection and if the sample not collected in the time of viral replication [9].
Our study aimed to compare the accuracy of both chest CT and RT-PCR results in diagnosing COVID-19 infection in clinically suspected patients. Also, to correlate between CT Severity Scores (CTSSs) and RT-PCR results.
This prospective interventional study was carried out following the approval of the Research Ethical Committee, from 1 November 2021 to 31 March (code: 35902/10/22) on 200 patients suspicious for COVID-19 pulmonary infection, collected from hospitals; ICU and out patients clinic. All patients had done chest CT and RT-PCR tests at a time interval of no longer than 7 days between the two tests. The exclusion criteria include pre-existing chronic respiratory illness like pulmonary tuberculosis, and more than 7days time interval between chest CT and RT-PCR (> 7 day).
Demographic data (age, sex), medical history of comorbid diseases (diabetes mellitus, hypertension, chronic kidney disease, cardiac disease, cancer) and clinical data (presenting symptoms, risk factors and ICU admission) were collected from each patients. A written informed consent was obtained from all patients that clinical, laboratory and radiological data had to be used in the study.
Chest CT was performed on GE 128 slice machine at time of admission for patient in acute phase. The scans were obtained while the patient in supine position at end of inspiration with hands raised above head and hold his breath. Three expert radiologists examined the images in conjunction. The CT scans were either positive or negative based on CT findings (ground-glass opacity, consolidation, thickened interlobular septa, crazy paving) and site of lesion (left, right or bilateral). Severity of lung involvement on the chest CT was assessed using the CT scoring bases (CTSS and CO-RADS).
This study comprised 200 patients with CT suspicious for COVID-19 pulmonary infection and having done RT-PCR within 3 days. They were 132 males (66%) and 68 females (34%) with ages range 18-74 years (mean age of 48 years). Table 1 summarizes the baseline characteristics of patients, results of both CT and RT-PCR. The severity of lung involvement using CT scoring bases (CTSS and CO-RADS) was correlated with age, sex, and RT-PCR results (+ve and -ve).
Table 1: Baseline characteristics in studied patients. View Table 1
CO-RADS classifications: The CO-RADS categorization allows for dividing then on-enhanced chest CT scan into groups related to severity and confirmed COVID-19 cases from low grade or normal (CO-RADS 1,2) to high grade proven infection by comparing symptoms and signs of disease. CO-RADS 1 (normal scan/non-infection), CO-RADS 2 (typical for other infections), CO-RADS 3 (present in COVID and other diseases), CO-RADS 4 (suspicious), CO-RADS 5 (typical).
The most common CT lesion patterns in both positive and negative RT-PCR groups were ground glass opacities (GGO) and mixed GGO + consolidation.
The most frequent distribution was peripheral distribution (Bilateral and in lower lobe). The distributions of lesions, and lesion patterns seen in patients of both groups were shown in Table 2 and Figure 1, Figure 2, Figure 3 and Figure 4. CTSS calculated for 162 patients with positive chest CT scans showed that there was strong positive correlation in CT severity score and male sex. Twelve out of 14 patients with score 4 and 8 out of 8 patients with score 5 of lung involvement were male patients (Table 3 and Figure 5).
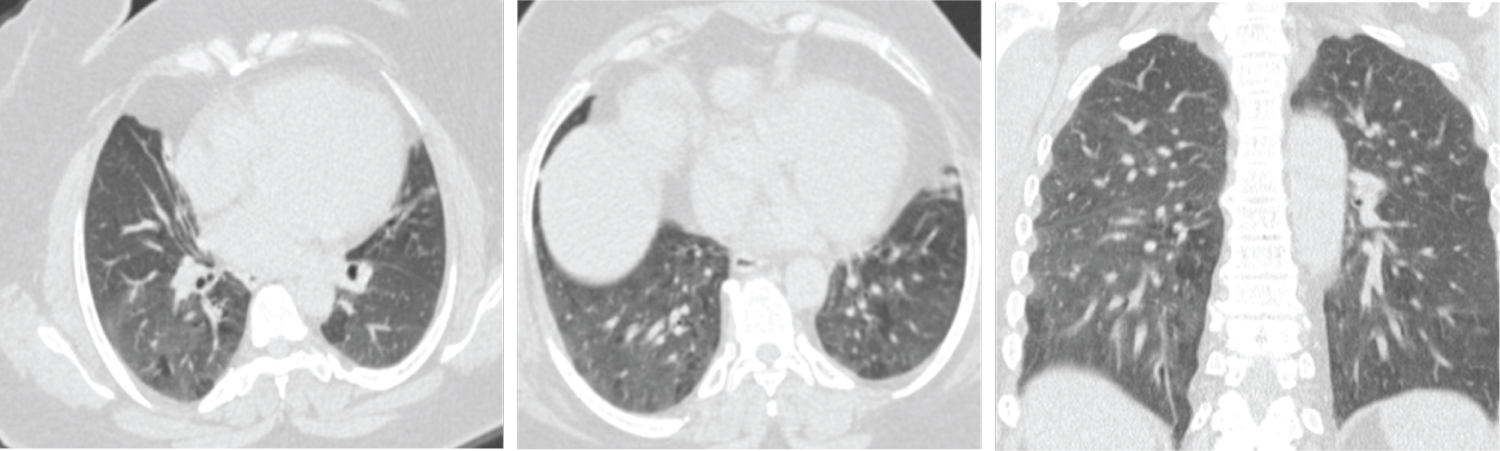 Figure 1: Female patient aged 51-years-old had negative initial reverse transcription-polymerase chain reaction results. Axial and coronal CT chest cuts shows diffuse mosaic lung attenuation with bilateral basal fine at electatic bands likely of cardiac causes (CORADS 1).
View Figure 1
Figure 1: Female patient aged 51-years-old had negative initial reverse transcription-polymerase chain reaction results. Axial and coronal CT chest cuts shows diffuse mosaic lung attenuation with bilateral basal fine at electatic bands likely of cardiac causes (CORADS 1).
View Figure 1
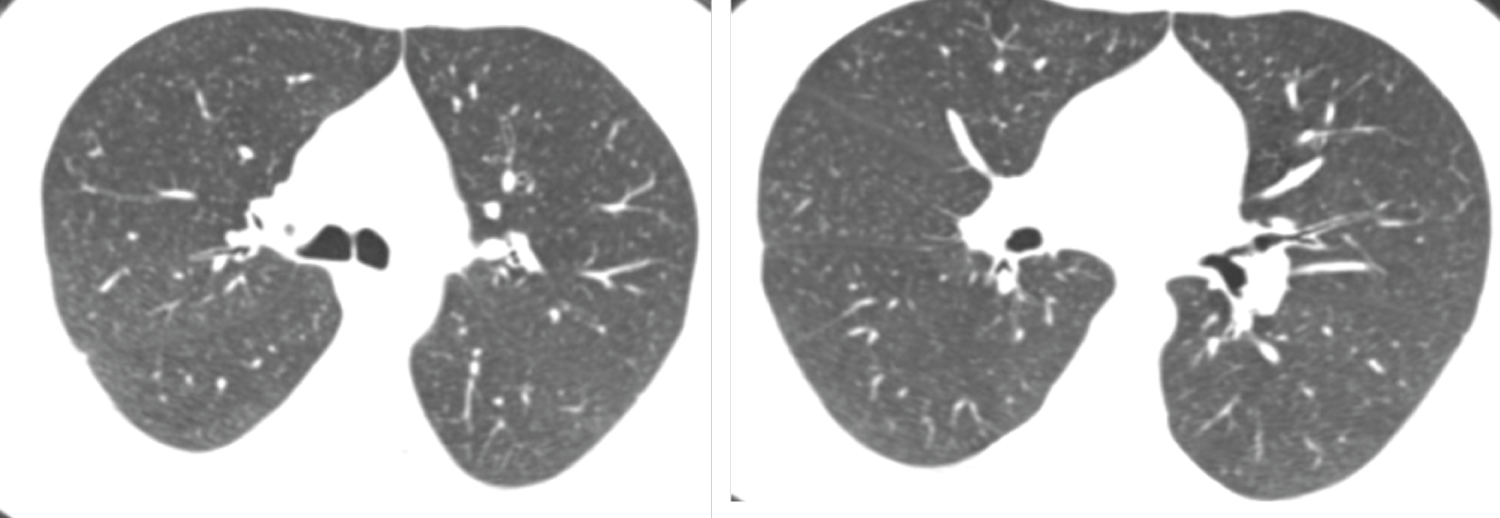 Figure 2: Male patient aged 49-years-old had negative initial reverse transcription-polymerase chain reaction results. Axial CT chest cuts show bilateral decreased both lung attenuation with increased both lung volumes denoting hyperinflation associated with bilateral upper lobe fine centrilobular ground glass nodular infiltration suggestive of smoking related bronchiolitis (respiratory bronchiolitis) (CORADS 1).
View Figure 2
Figure 2: Male patient aged 49-years-old had negative initial reverse transcription-polymerase chain reaction results. Axial CT chest cuts show bilateral decreased both lung attenuation with increased both lung volumes denoting hyperinflation associated with bilateral upper lobe fine centrilobular ground glass nodular infiltration suggestive of smoking related bronchiolitis (respiratory bronchiolitis) (CORADS 1).
View Figure 2
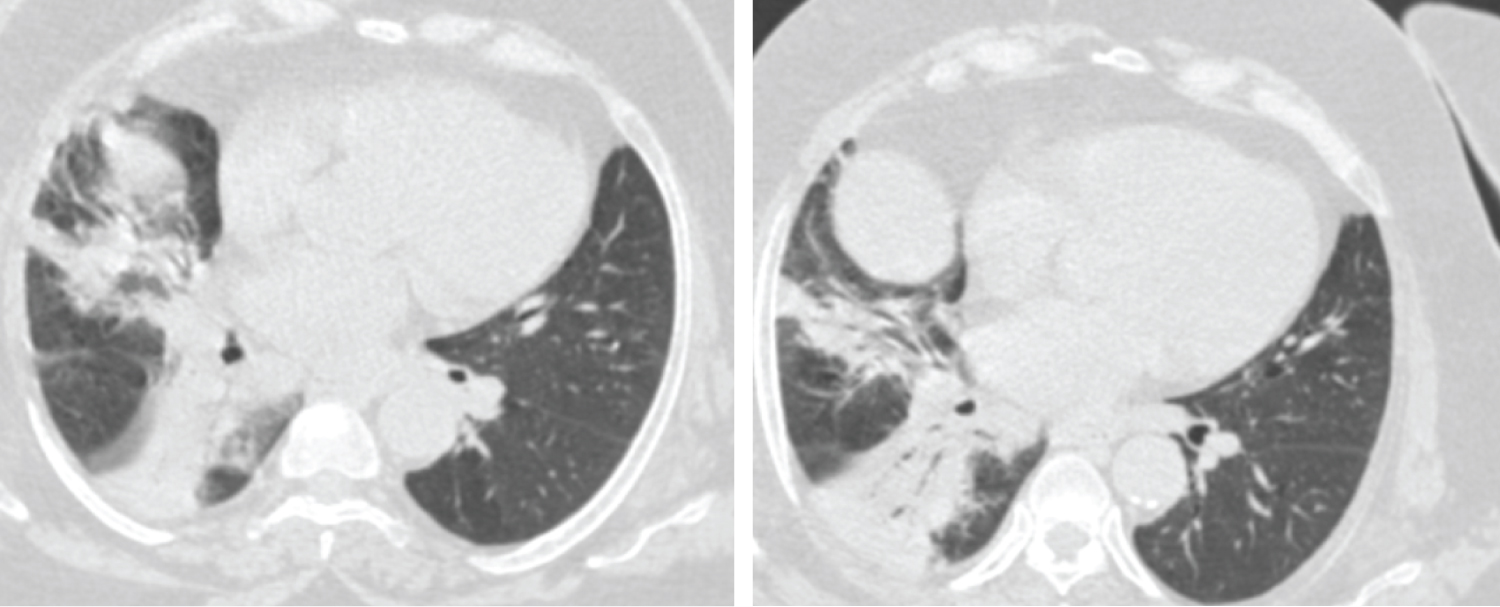 Figure 3: Female patient aged 56-years-old had positive initial reverse transcription-polymerase chain reaction results. Axial CT chest cuts show two patchy areas of consolidation with air bronchogram within are seen at middle lobe of right lung and right lower lung lobe these findings are unclear for COVID-19 (CORADS 3).
View Figure 3
Figure 3: Female patient aged 56-years-old had positive initial reverse transcription-polymerase chain reaction results. Axial CT chest cuts show two patchy areas of consolidation with air bronchogram within are seen at middle lobe of right lung and right lower lung lobe these findings are unclear for COVID-19 (CORADS 3).
View Figure 3
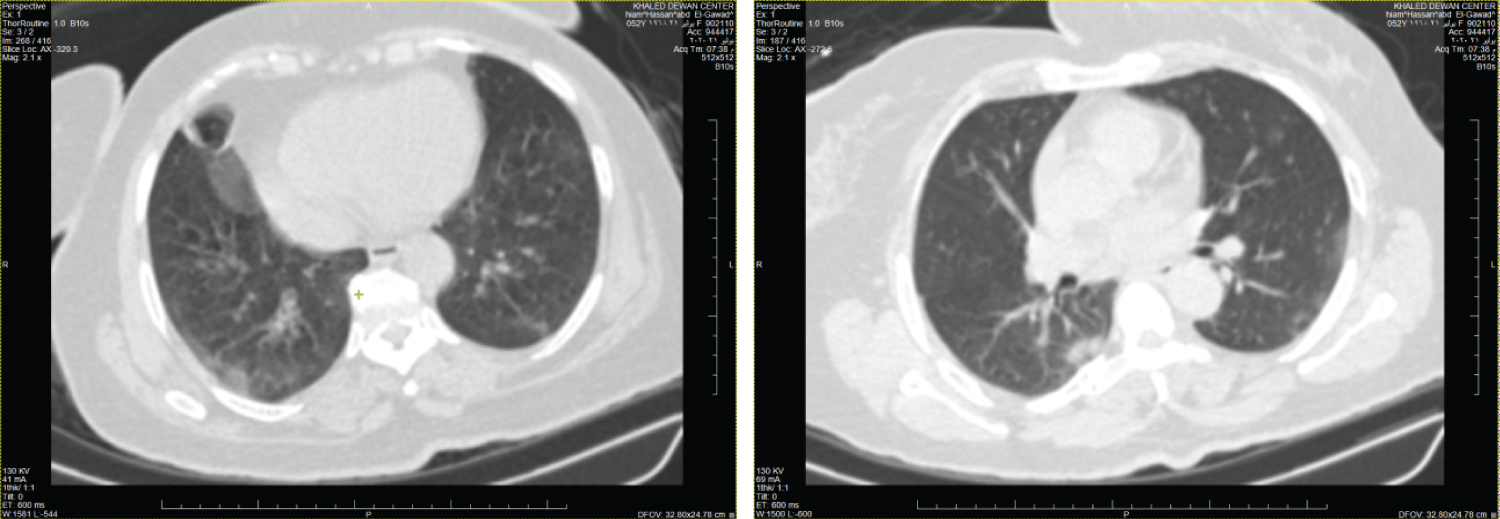 Figure 4: Female patient aged 37-years-old had negative initial reverse transcription-polymerase chain reaction results. Axial CT chest cuts shows bilateral ill-defined ground glass opacities with peripheral & sub-pleural in distribution seen at both upper and lower lung lobes these findings are highly suspected for COVID-19 (CORADS 4).
View Figure 4
Figure 4: Female patient aged 37-years-old had negative initial reverse transcription-polymerase chain reaction results. Axial CT chest cuts shows bilateral ill-defined ground glass opacities with peripheral & sub-pleural in distribution seen at both upper and lower lung lobes these findings are highly suspected for COVID-19 (CORADS 4).
View Figure 4
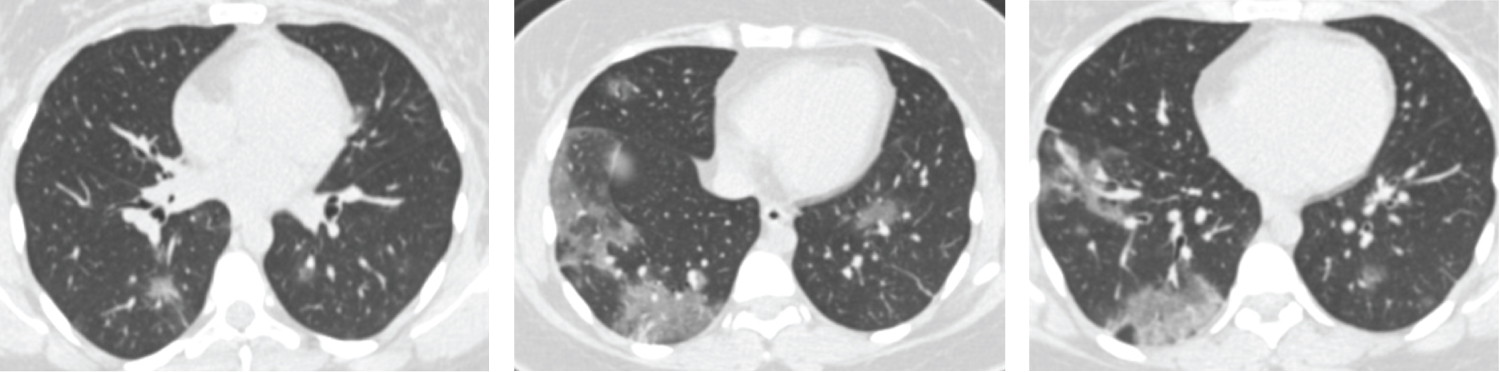 Figure 5: Male patient aged 60-years-old had positive initial reverse transcription-polymerase chain reaction results. Axial CT cuts show bilateral multi-focal ground glass opacities & smaller areas of consolidation are seen involving both lung fields with peripheral/subpleural predominance, this together with multiple subpleural lines this in keeping with viral pneumonia (COVID-19) (CORADS 5).
View Figure 5
Figure 5: Male patient aged 60-years-old had positive initial reverse transcription-polymerase chain reaction results. Axial CT cuts show bilateral multi-focal ground glass opacities & smaller areas of consolidation are seen involving both lung fields with peripheral/subpleural predominance, this together with multiple subpleural lines this in keeping with viral pneumonia (COVID-19) (CORADS 5).
View Figure 5
Table 2: Lesion and distribution pattern in reverse transcription polymerase chain reaction positive and negative (RT-PCR). View Table 2
Table 3: Correlation between CT severity score (CTSS) and sex. View Table 3
In addition, the age group was categorized into three groups: Those with less than 40 years of age; between 40 and 60 years and those above 60 years. There was significant correlation of CT severity score with increasing age; 22 patients out of total 162 who had total lung involvement of more than 50% were 60 years or above 60 years of age (with score 4 and 5) (Table 4, Figure 5 and Figure 6). CTSS had high correlation with RT-PCR results. Patients with higher CTSS were more usually RT-PCR positive (Table 5).
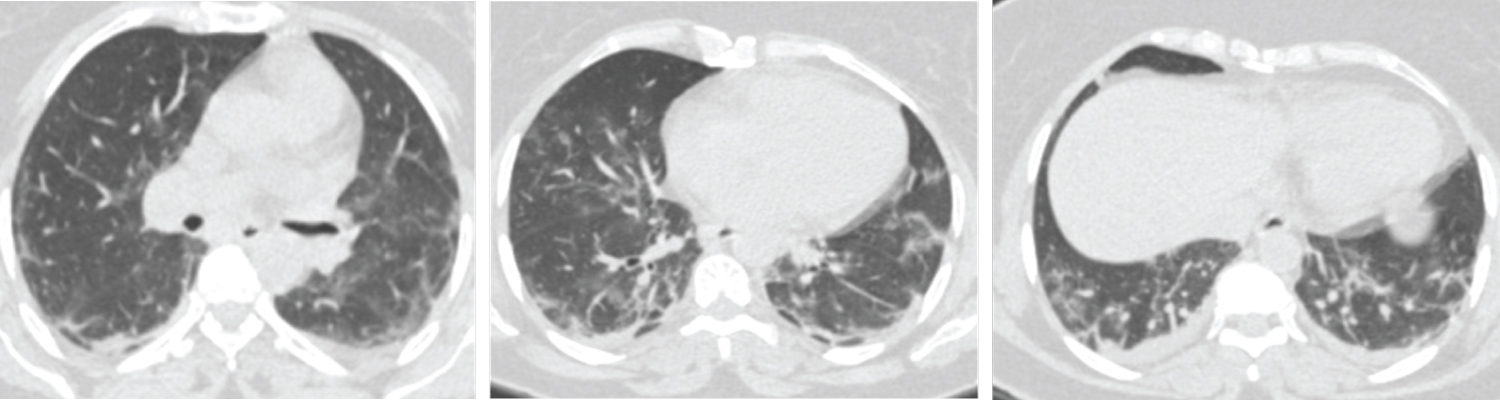 Figure 6: Male patient aged 63-years-old had positive initial reverse transcription-polymerase chain reaction results. Axial CT cuts shows bilateral multi-focal ground glass opacities are seen involving both lung fields with Peripheral/subpleural predominance. This together with multiple subpleural lines and bilateral minimal pleural effusion, these findings is in keeping with viral pneumonia (COVID-19) (CORADS 5).
View Figure 6
Figure 6: Male patient aged 63-years-old had positive initial reverse transcription-polymerase chain reaction results. Axial CT cuts shows bilateral multi-focal ground glass opacities are seen involving both lung fields with Peripheral/subpleural predominance. This together with multiple subpleural lines and bilateral minimal pleural effusion, these findings is in keeping with viral pneumonia (COVID-19) (CORADS 5).
View Figure 6
Table 4: Correlation between CT severity score (CTSS) and age groups. View Table 4
Table 5: Correlation between CT severity score (CTSS) and PCR results. View Table 5
The thin section CT image chest became an essential diagnostic tool during the COVID-19 outbreak [10]. Similar to other viral pneumonia, the CT features include ground glass opacification, segmental and sub-segmental thickness (crazy paving), consolidation, and interstitial infiltration [11,12]. The typical findings in CT of COVID-19 patients were patchy, rounded segmental and sub-segmental ground glass opacification that may end to consolidation [13,14].
In our study, we analyzed 200 patients presenting with clinically suspected COVID-19, out of them 132 (61%) were male, and 68 (34%) were female. The mean age of all patients was 48 ± 16.0 years (range, 18-74 years).
The clinical symptoms ranging from fever and cough to severe respiratory distress. We found that old age male gender presented with more severe CT pulmonary changes (i.e., higher CT severity score). This matched to that reported by Liu, et al. [13]. We detected in our study that the predominant lesion distribution was present in posterior and basal part of the lung. This closely matched with that of Song, et al. [15] who found that 82% of COVID-19 patients had posterior lung involvement. Also, Yang, et al. [16] whose results added that the consolidation was significantly associated with disease severity too. Both groups of RT-PCR (+ve and -ve) showed similar symptoms with fever and cough being the most frequent symptoms. Nearly all patients with +ve RT-PCR had COVID-19 and showed positive findings at chest CT and typical CT findings were present in most patients with negative RT-PCR tests. The most common lesion patterns in the present study was GGO, consolidation, and GGO + consolidation (mixed) observed in bilateral, peripheral, and lower lobe distributions. Similar results had been reported in different studies [17,18], and other CT findings such as crazy-paving pattern, halo and reversed halo sign, had been described [19]. Previous researchers suggested that the sensitivity of CT findings was higher than that of RT-PCRs [20]. Similar findings in previous study that reported the sensitivity of CT to be 98% in diagnosing COVID-19 infection compared to RT-PCR that showed a sensitivity of 71% [7,21].
Chest CT is important in the screening of patients in whom disease was clinically suspected, especially those who had negative initial RT-PCR results. Higher CT severity score was positively correlated with male gender and older age group patients. Due to the false-negative rate of RT-PCR tests caused by various reasons, (insufficient cellular material for detection and improper extraction of nucleic acids from clinical materials), therefore Chest CT is more accurate, available, realistic, and fast method for diagnosing and assessing suspected COVID-19 patients compared to RT-PCR. Were commend chest CT to be a part of the diagnostic work-up in a suspected patient with high clinical symptoms of COVID-19 before, hospitalization, intensive care unit admission and when RT-PCR testing is unavailable or negative test.