The present case report discussed the management of a 62-year-old female patient with medically refractory trigeminal neuralgia with percutaneous CT-guided gasserion ganglion block (CT-GGB). Using Hartel anterior approach, we successfully performed CT-GGB with precise positioning of 22G LP needle tip in the medial aspect of foramen ovale at the base of the skull as was witnessed clinically by the patient as sharp pain along the affected areas of the face, confirmed by serial CT screening until it reaches the predefined depth. Later neurolysis mixture was injected, the needle was finally flushed with 0.5 mL of normal saline and then withdrawn. Sterile dressing was applied at the skin entry site after removing the LP needle. Post-procedural check CT was performed to look for any immediate complications. Patients were observed for regular follow-up at 1 week, 2 weeks, 1 month, 3 months, and every 3 months after that. The patient was relieved entirely of facial pain on the CT table (NRSP - 0) with minimal facial numbness and no sensation loss. To conclude, CT-GGB invention is an effective and safe technique for medically refractory trigeminal neuralgia.
Gasserion ganglion block, Computed tomography, Trigeminal neuralgia, Neurolysis mixture
Trigeminal neuralgia is a painful condition that causes shooting or jabbing sensations similar to an electric shock on one side of the face and is more likely to occur in people older than 50 years, affecting women more often than men. The symptoms may be short-lived mild attacks but can progress to more-frequent chronic bouts of searing pain involving the trigeminal nerve, which carries sensation from face to brain. Although the condition is not life-threatening, the intensity of the pain can be debilitating. Treatment options range from medications to surgical (Microvascular decompression) management. Percutaneous Rhizotomy procedures (Balloon compression, Glycerol injection, Radiofrequency thermal lesioning) are on the rise; however, they are performed using fluroguidance with little literature on computed tomography (CT) use as a tool of interest.
A 62-year-old female came to the interventional radiology (IR) department with a history of chronic toothache which had undergone root canal management, complaining of right-sided severe facial pain diagnosed as trigeminal neuralgia and was on medical management. Presently she suffers from severe pain in the right half of her face with mild swelling, which worsens while brushing, eating, chewing, and swallowing. She has been unable to sleep for the last 3 days owing to severe sharp pain. She is a known diabetic, hypertensive, hypothyroid, seizure disorder, multi-infarct state and was admitted to the hospital with altered sensorium twice in a span of last 3 months, during which she was found to have hypoglycaemic encephalopathy, septic shock on first admission and hypomagnesemia on second admission for which she was treated conservatively and recovered completely. Her MRI brain plain revealed multiple chronic lacunar infarcts in bilateral thalami, left caudate nucleus, both halves of the midbrain, and right cerebellum with mild to moderate periventricular and subcortical ischemic changes in bilateral frontal and parietal regions. 3D FIESTA MRI didn’t reveal any significant abnormality (Figure 1). The treating team converged on a diagnosis of trigeminal neuralgia resistant to conservative medical management and offered her options of microvascular decompression neurosurgery and percutaneous CT Guided Gasserion Ganglion block. After understanding its risks and benefits, the patient and their relatives opted for a CT-guided procedure. Basic pre-procedural blood investigations were done, peri procedure antibiotic started, and NRSP (numerical rating scale pain score) was recorded. The patient was placed in a supine position with head first (towards the gantry) on the CT table with neck extended and head tilt of 15-30 degrees contralateral to the affected side of the face. Sterile draping and local anaesthetic infiltration at the skin entry site were done. Using Hartel anterior approach, we successfully performed CT-guided percutaneous gasserion ganglion block (CT-GGB) with precise positioning of 22G LP needle tip in the medial aspect of the foramen ovale at the base of the skull as was witnessed by a patient as sharp pain along the affected areas of the face, confirmed by serial CT screening until it reaches the predefined depth. Following this neurolysis mixture consisting of 1 ml (40 mg) triamcinolone, 2 ml of 2% xylocaine, 3 ml of 0.5% bupivacaine, and 0.5 ml contrast was injected (Figure 2, Figure 3 and Figure 4). The needle was finally flushed with 0.5 mL of normal saline and then withdrawn. Sterile dressing was applied at the skin entry site after removing the LP needle. Post-procedure check CT was performed to look for any immediate complications. Patient was observed for 2 hours and then sent home with advice to monitor blood sugars, stop oral analgesic medications, and regular follow-up at 1 week, 2 weeks, 1 month, 3 months, and every 3 months after that.
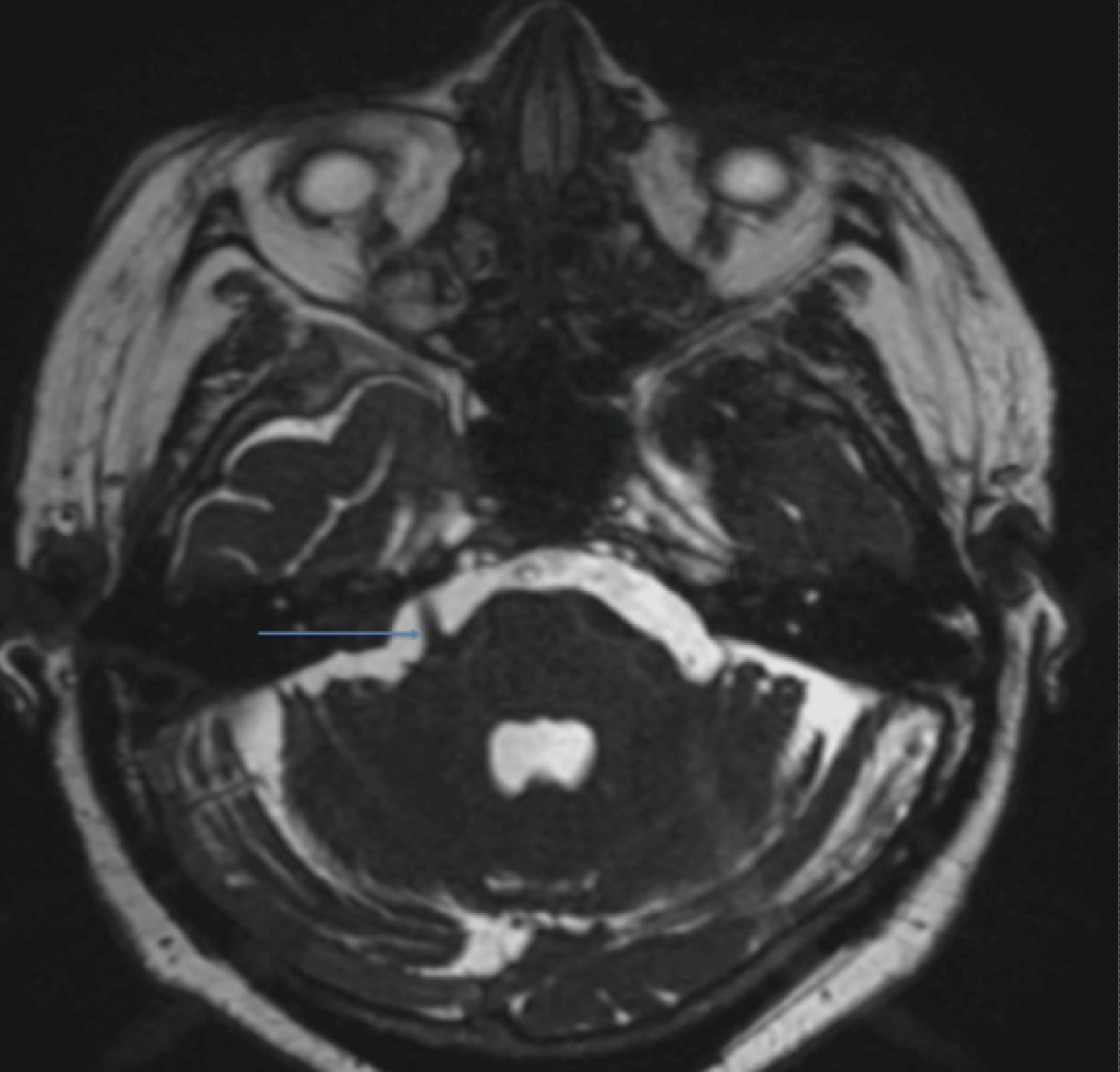 Figure 1: MRI brain 3D FIESTA showing right trigeminal nerve (blue arrow).
View Figure 1
Figure 1: MRI brain 3D FIESTA showing right trigeminal nerve (blue arrow).
View Figure 1
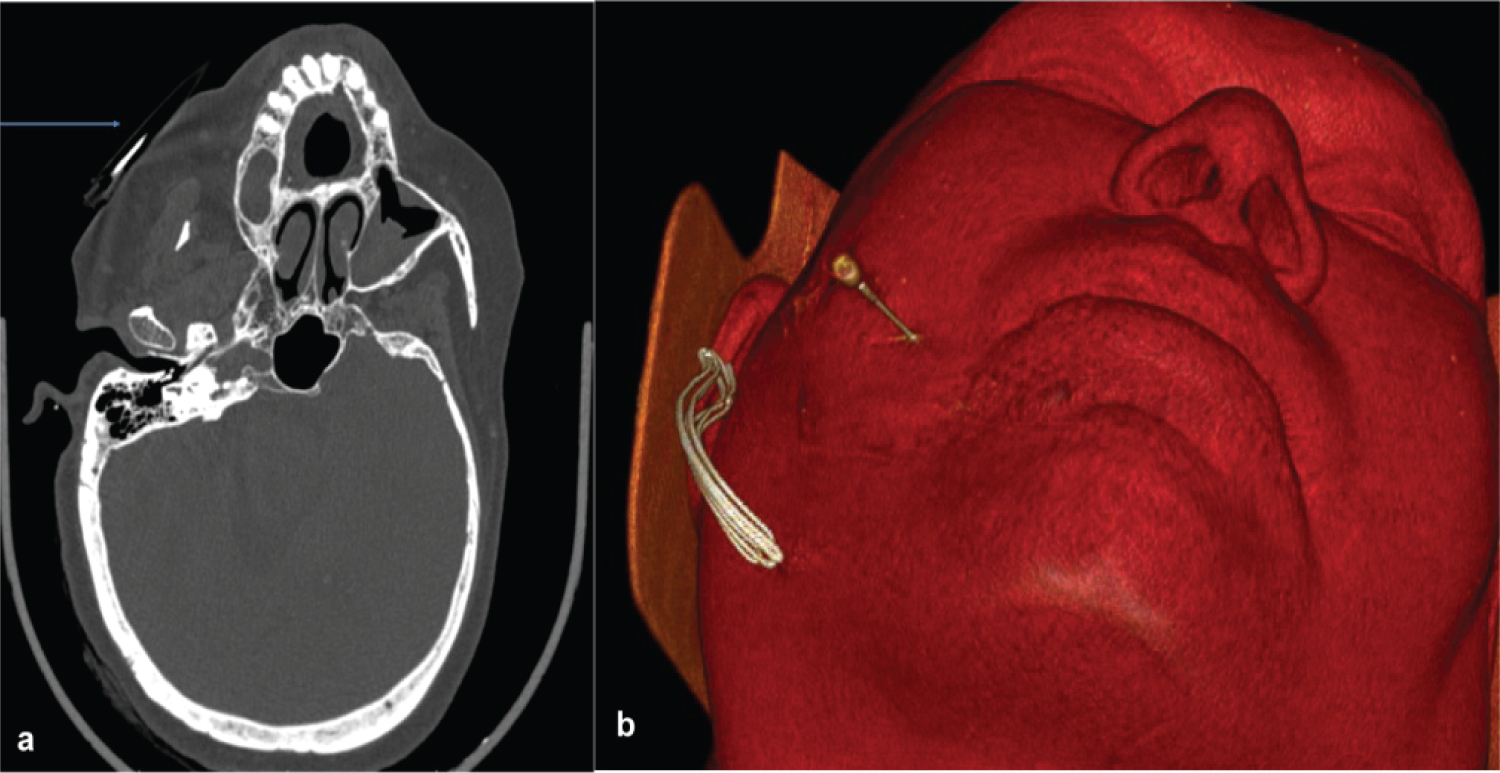 Figure 2: CT axial view (a) and 3D VR reformat (b) showing dense radio marker (blue arrow); lateral head tilt positioning along with the site of needle entry.
View Figure 2
Figure 2: CT axial view (a) and 3D VR reformat (b) showing dense radio marker (blue arrow); lateral head tilt positioning along with the site of needle entry.
View Figure 2
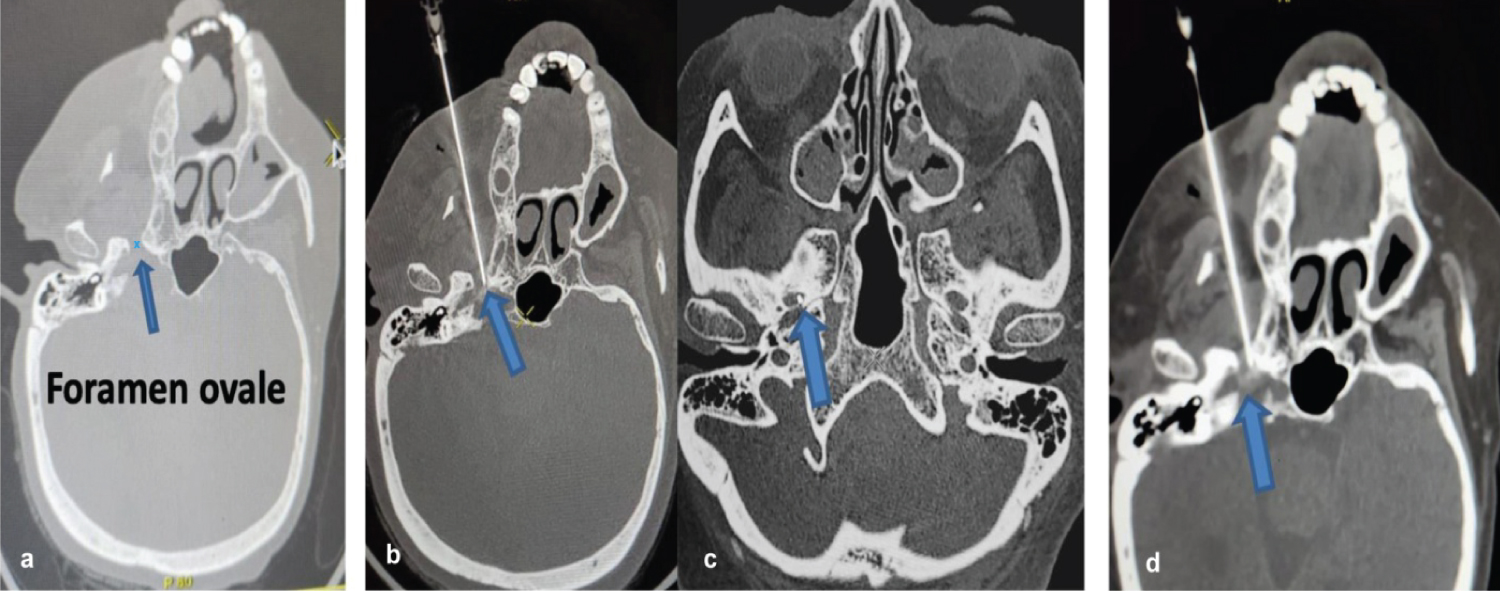 Figure 3: CT Brain sections with blue arrows showing (a) foramen ovale intra-procedure: Needle tip (b,c) in the medical aspect of foramen ovale with drug percolation (d).
View Figure 3
Figure 3: CT Brain sections with blue arrows showing (a) foramen ovale intra-procedure: Needle tip (b,c) in the medical aspect of foramen ovale with drug percolation (d).
View Figure 3
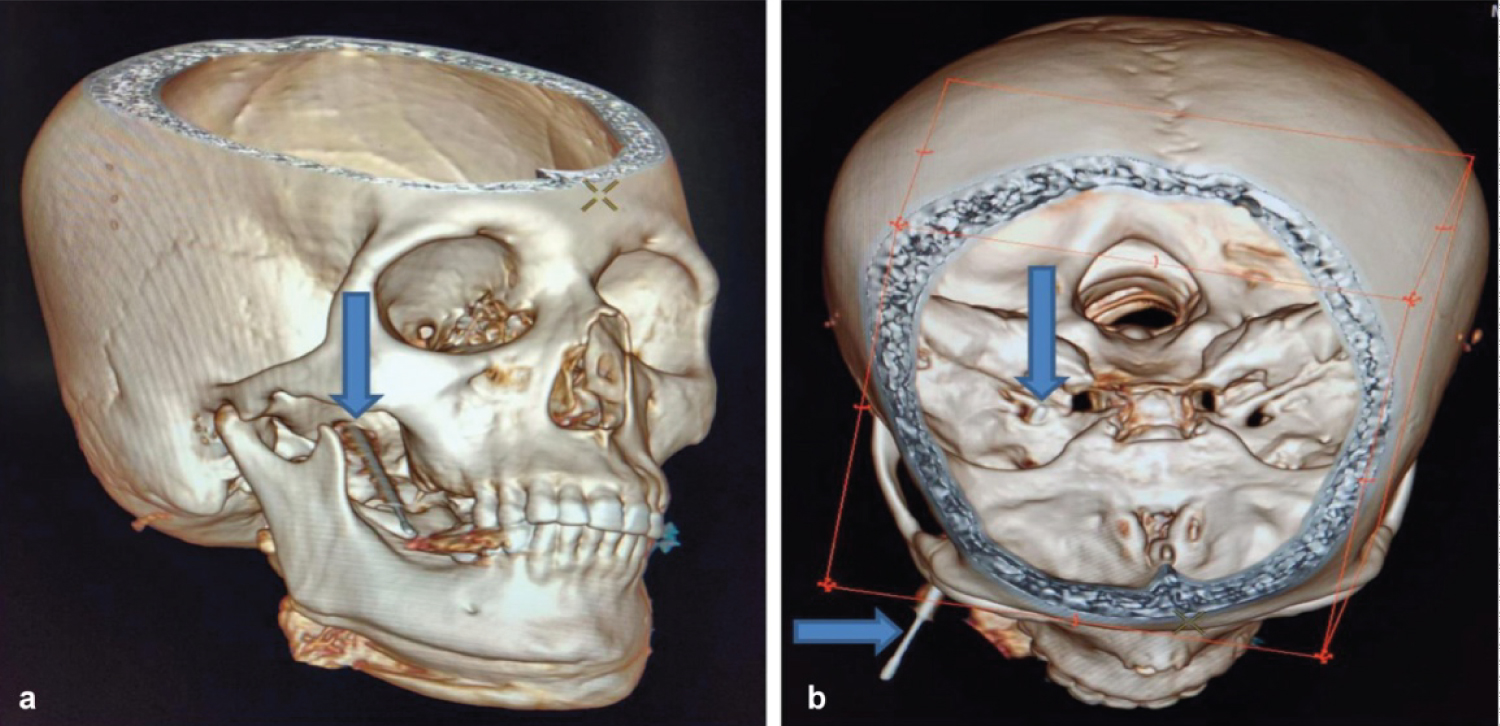 Figure 4: 3D volume rendered (VR) images (a,b) of the skull showing the needle entry point and its tip within foramen ovale (blue arrows).
View Figure 4
Figure 4: 3D volume rendered (VR) images (a,b) of the skull showing the needle entry point and its tip within foramen ovale (blue arrows).
View Figure 4
The patient was relieved entirely of facial pain on the CT table (NRSP - 0) with minimal facial numbness and no sensation loss. There were no immediate procedure-related complications; swelling of the cheek increased at 1-month follow-up (NRSP -2) with a gradual reduction at 3 months follow-up (NRSP- 0). Her overall quality of life has improved, and she can do her day-to-day activities efficiently even after 6 months post-treatment.
“Trigeminal neuralgia (TN) is defined by paroxysmal, sudden, unilateral, brief, electric shock-like, and recurrent pain in the facial region innervated by the trigeminal nerve." Refractory TN can lower a patient's quality of life and cause depression [1]. Antiepileptic medications are used as the first line of treatment for TN, although they are unsuccessful in some patients, and some patients cannot tolerate their adverse effects. Despite the availability of other surgical procedures, a nerve block is a quick and secure percutaneous therapy for TN patients. In the present case report, we reported a case complaining of right-sided severe facial pain diagnosed as trigeminal neuralgia and subjected to a CT-guided percutaneous gasserion ganglion block (CT-GGB) procedure. She was completely relieved of facial pain on the CT table (NRSP - 0) with minimal facial numbness and no sensation loss. There were no immediate procedure-related complications; swelling of the cheek increased at 1-month follow-up (NRSP -2) with a gradual reduction at 3 months follow-up (NRSP- 0). Her overall quality of life has improved, and she can do her day-to-day activities efficiently even after 6 months post-treatment. According to the authors' literature review, only two studies were pertinent to the current investigation. In a prospective study by Lan, et al. [2] involving 28 patients with idiopathic TN who underwent CT-guided percutaneous PRF treatment of the Gasserian ganglion, the researchers discovered that the postoperative NRS score steadily reduced from 7.6 pre-operative to 0.1 postoperative. Recently, Sun, et al. [3] conducted a multicentric retrospective analysis on patients who had received a gasserian ganglion block with CT guidance and suffered from acute or subacute zoster-related trigeminal neuralgia. According to their research, all patients' postoperative NRS scores considerably dropped. At various time points, the acute zoster group's NRS scores were lower than those of the subacute zoster group. The current case uses a local anaesthetic and steroid combination as neurolysis mixture for refractory trigeminal neuralgia. Medically unresponsive trigeminal neuralgia can be treated safely and effectively with CT-guided innovation.
In clinical scenarios with co-morbidities, as discussed above, minimally invasive percutaneous interventional procedures like CT Guided Gasserion Ganglion block can relieve severe facial pain with a low risk of complications. CT guidance during the procedure ensures better accuracy, safety, and favourable response in pain relief. However, future studies must be investigated to determine the ultimate effective and safer choice.
The authors would like to thank the management of Medicover Hospital, Visakhapatnam.
Nil.
Nil.