Background: Accessory breast tissue is residual breast tissue that persists from normal embryologic development. This is an uncommon clinical finding and a clinical concern for patients and diagnostic challenges for physicians. Our objective was to report the clinical, mammographic, and ultrasonographic features of our department.
Methods and results: This retrospective study included patients diagnosed with accessory breast tissues. Demographic data, complaints, physical examination findings, and mammographic and/or ultrasonographic features were analyzed. Ten female patients were enrolled in this study. All accessory breast tissues were localized to the axilla. Two patients were asymptomatic, eight complained of axillary swelling, three of which were bilateral, and two were accompanied by milk discharge. One patient presented with an axillary nipple with an areola. All symptomatic patients were concerned about the malignancy and cosmetic disfigurement. Six of the patients were classified as class IV according to the Kajava classification. Ultrasound showed a normal appearance of breast tissue in nine patients, and a cyst was seen in one patient. No invasive procedures were performed and the patients were reassured.
Conclusion: Accessory breast tissue is considered a normal variant, rather than an abnormality. It can be asymptomatic and mostly presents as an axillary mass. Mammography and ultrasound are identical to those of the normal glandular parenchyma, and all breast pathologies can be found in accessory breast tissue.
Accessory breast tissue, Axillary, Mammography, Ultrasound
Accessory breast tissue is residual breast tissue which persists from normal embryologic development [1]. It includes both aberrant breast tissue, which is an island of breast tissue, and supernumerary breasts (polymastia), which may vary in their components of the nipple, areola, and ductal tissue and may have an organized duct system communicating with the overlying skin [2]. Accessory breast tissue is an uncommon clinical finding, with a reported incidence of 0.4-6% [3]. This represents a clinical concern for patients and diagnostic challenges for physicians. Our objective was to report the clinical, mammographic, and ultrasonographic features in our department.
This retrospective study was carried out in our department “La vita per Te, Akbaraly Foundation” between 2016 and 2023, including all patients diagnosed with accessory breast tissue. The following items were analyzed: Demographic data, complaints, physical examination findings, and mammographic and/or ultrasound features. We used digital mammography and Logiqxp portable ultrasound with a 7 Mhz linear probe.
Ten female patients were enrolled in this study. The mean age was 40.2 years. All accessory breast tissues were localized to the axilla. Two patients were asymptomatic; eight complained of axillary swelling (Figure 1a and Figure 1b), three of which were bilateral and two were accompanied by milk discharge. One patient presented with an axillary nipple with areola (Figure 1c). All 8 symptomatic patients were concerned about malignancy and cosmetic disfigurement. According to the Kajava Classification [4]: Six out of ten patients were classified as class IV: Only glandular tissue, 3 as class II: Gland with a nipple and one as class I: Glandular tissue and areola nipple. Three out of ten patients underwent mammography, which revealed a small amount of dense fibroglandular tissue in the axilla separated from the main breast tissue (Figure 2a, Figure 2b and Figure 2c). Ultrasound showed a normal appearance of breast tissue (Figure 3a) in 9 patients with fibroductal tissue and lobules of fat, a cyst was seen in one patient (Figure 3b). No invasive procedures, such as biopsy or surgery, were performed, and the patients were reassured.
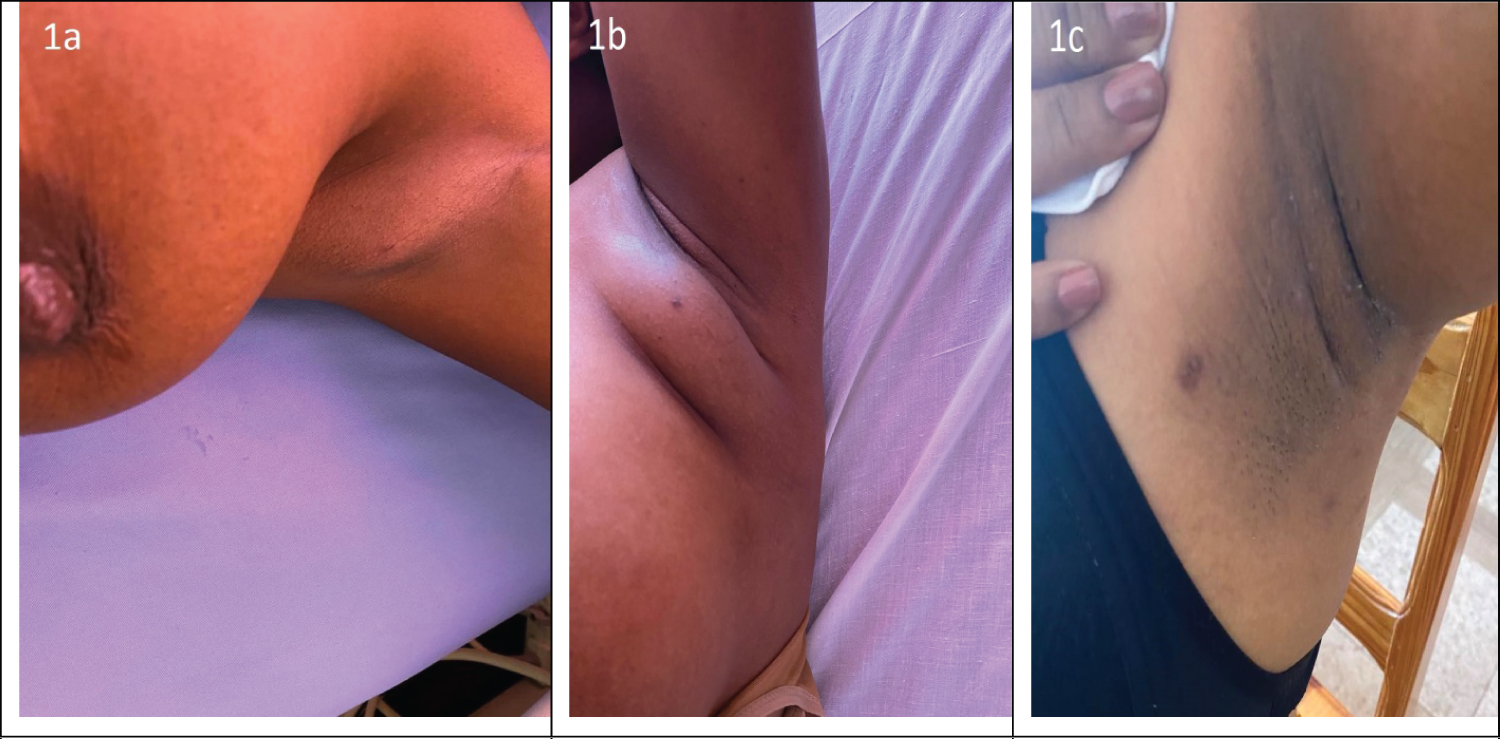 Figure 1: (a, b & c) Axillary accessory breast tissue.
View Figure 1
Figure 1: (a, b & c) Axillary accessory breast tissue.
View Figure 1
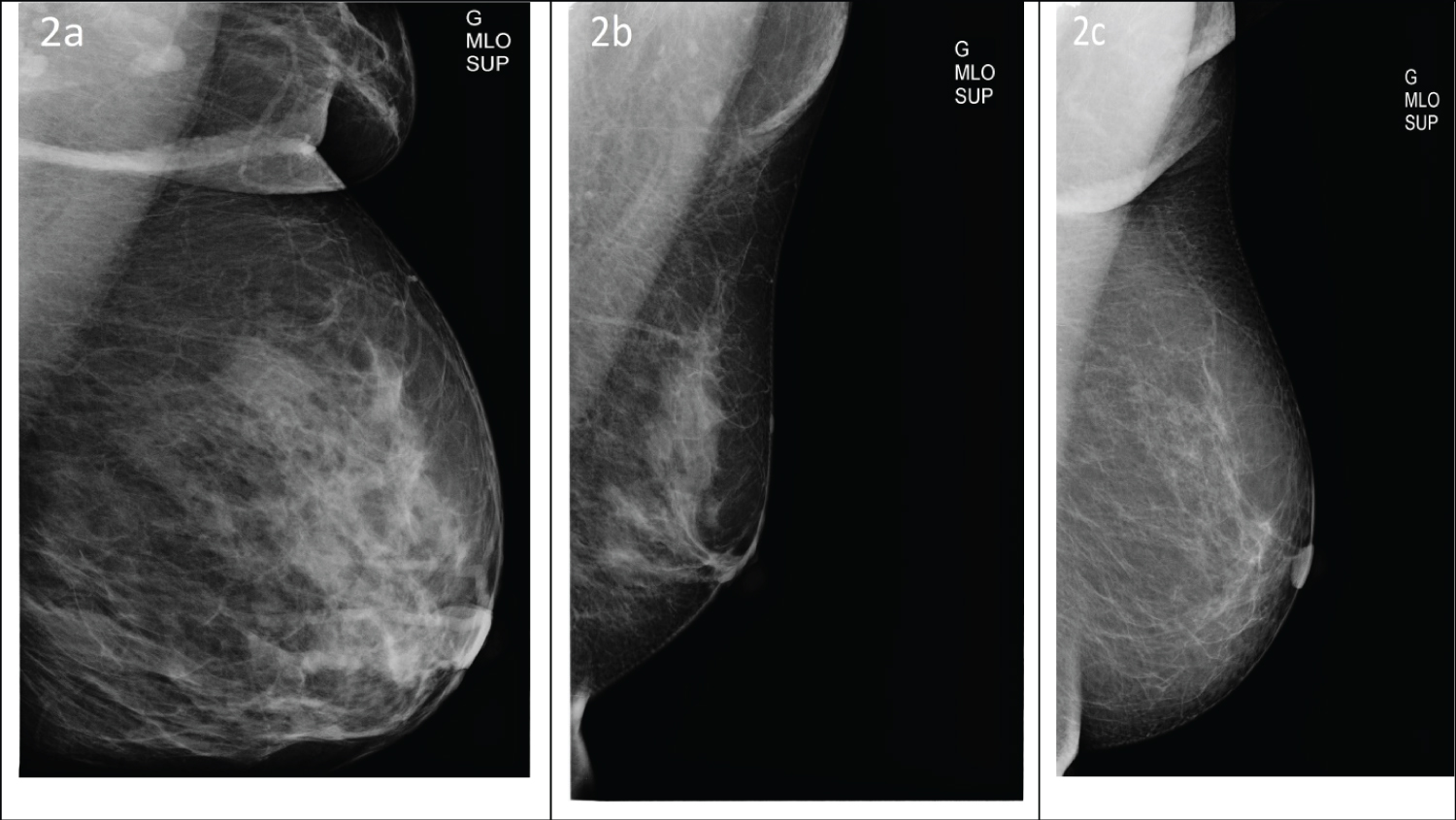 Figure 2: (a, b and c) Mammography medio-lateral oblique views showing dense fibroglandulary tissue in the axilla.
View Figure 2
Figure 2: (a, b and c) Mammography medio-lateral oblique views showing dense fibroglandulary tissue in the axilla.
View Figure 2
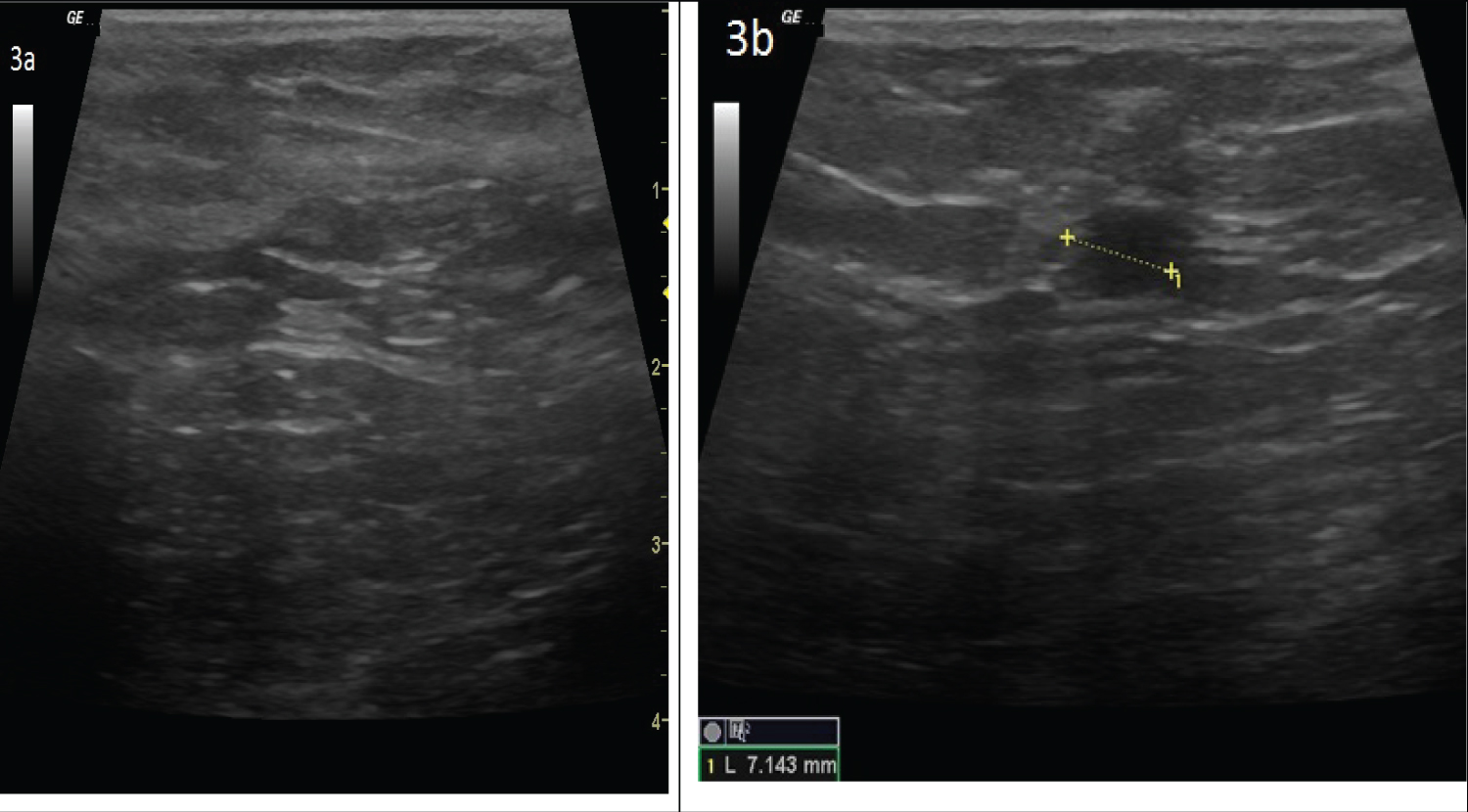 Figure 3: (a) Normal gray scale ultrasound showing fibro glandular tissue and lobule of fat; (b) A cyst as round and anechoic structure within axillary accessory breast.
View Figure 3
Figure 3: (a) Normal gray scale ultrasound showing fibro glandular tissue and lobule of fat; (b) A cyst as round and anechoic structure within axillary accessory breast.
View Figure 3
All physicians, especially those who potentially deal with breast pathology, such as general practitioners, gynecologists, radiologists, and surgeons, must be aware of accessory breast tissues. Knowledge about this entity has considerable implications for patient care: If it is not recognized for what it is, as a normal variant, it might be misdiagnosed as an abnormality [5]. The symptomatic cases in this study were concerned with malignancy and cosmetic disfigurement. It can also cause anxiety, pain, and restriction of arm movements [3]. Other clinical presentations have been reported, including pain or discomfort, milk secretion, and local skin erythema, which may be more pronounced during pregnancy and lactation [1]. Most of the referrals were suspicious axillary masses or lipomas. In the literature, the most common presumptive diagnoses are lipoma, lymphadenopathy, hidradenitis, sebaceous cysts, vascular malformations, and malignancy [6]. If doubt exists regarding the nature of the tissue, ultrasound is usually the first-choice imaging modality; mammography, MRI, needle biopsy, or surgical biopsy of the area should be undertaken [5,7].
The present study is consistent with the literature regarding the localization of accessory breast tissue, with the axilla being the most common site [8]. However, other localizations have been reported along the mammary ridge or milk line and can occur on the cheek, neck, shoulder, thigh, or buttock [9]. Here, we report a fibrocystic lesion within accessory breast tissue, but both benign and malignant diseases of accessory breast tissue, such as adenoma or invasive carcinoma, have been described [10,11].
On mammography, similar to ultrasound, accessory breast tissue in the axilla is identical to the normal glandular parenchyma and is separate from the breast, unlike the axillary tail of the spence, which is a normal direct extension toward the axilla from the main breast tissue. It varies from a small to large amount of fibroglandular elements and densities interspersed with fat on mammography. Ultrasound reveals fibroductal tissue and lobules of fat [5,7]. There was no invasive procedure realized in this study, such as biopsy or surgery; they were reassured most of the time due to financial issues. Surgical excision is the treatment of choice for symptomatic accessory axillary breast tissue. Cosmestic problems are the main indication in most cases. Tissue removal will relieve physical discomfort and confirm the diagnosis. Liposuction as an alternative if this option is feasible [3,7]. Management of accessory breast tissue cancer should follow the recommendations set forth for pectoral breast cancer of parallel TNM classification [6].
Accessory breast tissue is considered a normal variant, rather than an abnormality. It can be asymptomatic and mostly presents as an axillary mass. Mammography and ultrasound are identical to those of the normal glandular parenchyma and all breast pathology can be found in accessory breast tissue.
These authors contributed equally in this article.