Presented is a literature review on Multisystem inflammatory syndrome (MIS) which can occur following recovery from the initial phase of COVID-19 infection. Because of the predominance of gastro-intestinal symptoms MIS can mimic an acute abdomen. We present a series of two cases of MIS-A occurring over a six month period at a single institution. The rationale for this work was to highlight MIS-A as an emerging syndrome and reduce associated morbidity and mortality.
The primary objective of the study was to review the literature. Further, we describe the presentation, investigation and management of two cases of MIS-A which occurred at a single centre.
A literature search was conducted through Ovid with the keywords 'MIS', 'COVID-19', and 'post COVID'. The records of two cases of MIS-A that occurred at our health service were identified and reviewed.
MIS-A was diagnosed in two female patients (median age 30.5 years). Both patients presented with abdominal pain, fever, and localized abdominal tenderness. Computed tomography showed intestinal wall thickening (1/2) and mesenteric lymphadenopathy (2/2). Complications included ischemic changes on electrocardiogram (2/2), myocarditis on cardiac MRI (1/2), cardiogenic shock (1/2), and vasopressor requirement (1/2). Median length of admission was 11.5 days.
General surgeons should have a high index of suspicion for MIS in any surgical patient that presents with an acute abdomen two to six weeks after COVID-19 infection. Test for cardiac dysfunction early if MIS-A is suspected, and involve the infectious disease team early so that treatment is not delayed.
Peri-operative COVID, Acute abdomen, MIS, COVID-19, ICU
1. MIS should be a differential diagnosis for any patient presenting with an acute abdomen two to six weeks after COVID-19 infection.
2. Test for cardiac dysfunction early if MIS-A is suspected. This should include blood tests (cardiac troponin and B-Type natriuretic peptide), electrocardiogram, and echocardiogram. Cardiac MRI can be helpful for assessing for myocarditis, and can be performed after the initial period of recovery from MIS.
3. Involve the infectious disease team early so that treatment is not delayed.
4. A small proportion of MIS patients may present with concurrent surgical pathology that may require operative management. This is especially the case in MIS-C (< 21 years of age) patients, who can present with concurrent acute appendicitis.
5. Treatment should be guided by the infectious disease team, but usually consists of intravenous corticosteroid and sometimes Intravenous immune globulin (IVIG).
Since the start of the COVID-19 pandemic there have been approximately 671 million cases worldwide and 6.84 million deaths attributed to this disease [1]. The causative virus is severe acute respiratory syndrome coronavirus 2 virus (SARS-CoV-2) [2]. Peaks in incidence continue to occur and despite preventative efforts, the morbidity and mortality associated with the disease is considerable [3] (Figure 1).
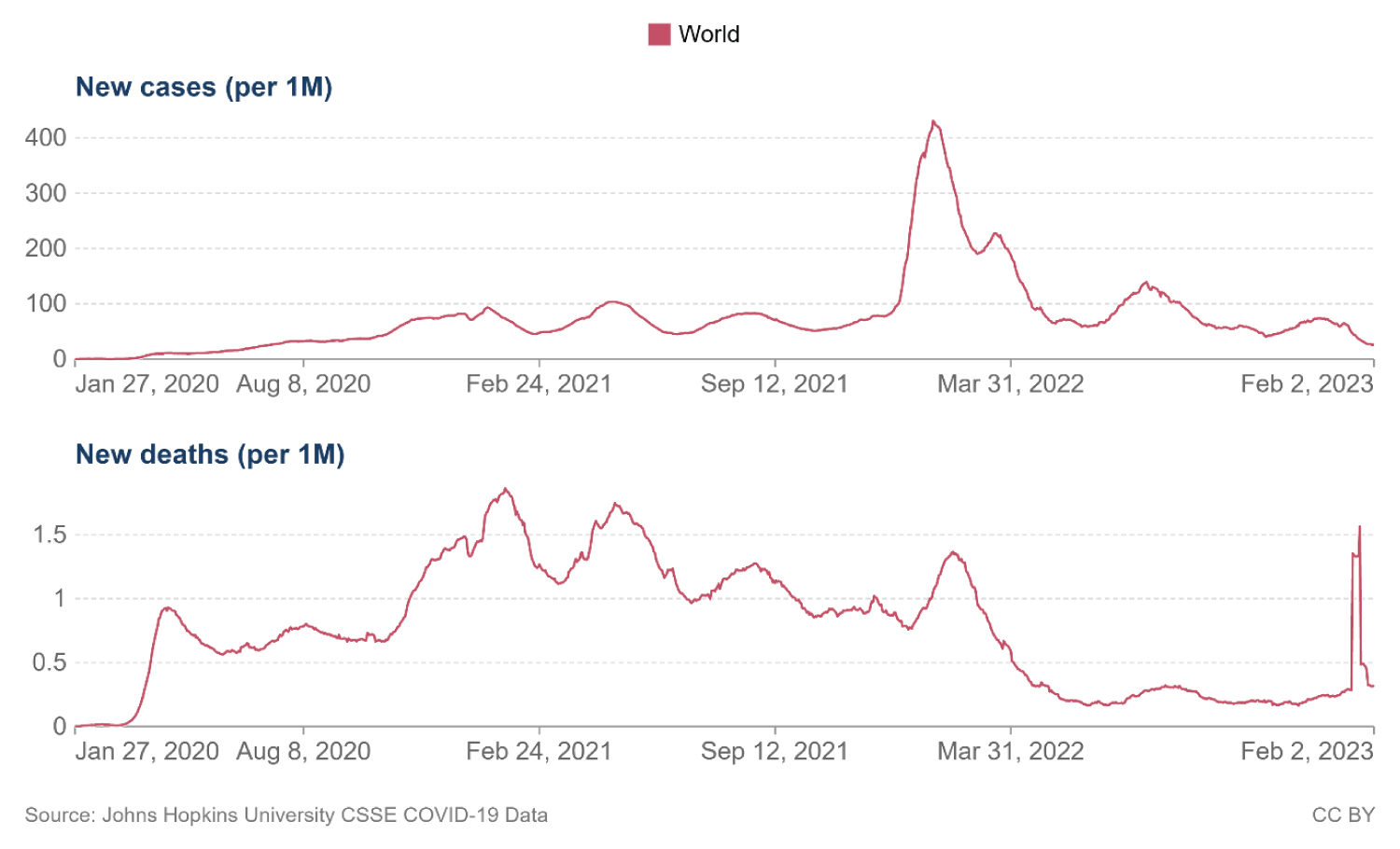 Figure 1: Prevalence and mortality rate for COVID-19 from 01/27/2020 to 02/02/2023 [1].
View Figure 1
Figure 1: Prevalence and mortality rate for COVID-19 from 01/27/2020 to 02/02/2023 [1].
View Figure 1
Several syndromes can occur following recovery from the acute phase of COVID-19 infection [4]. Multisystem inflammatory syndrome (MIS) is one of these. This syndrome is potentially fatal. It can occur in children and adolescents less than 21 years of age (MIS-C), and also in adults 21 years or older (MIS-A) [5]. The clinical manifestations of MIS can include fever, abdominal pain, and localized abdominal tenderness [6]. As patients can present with non-specific gastrointestinal symptoms, they can be misdiagnosed as an acute surgical abdomen [7].
This syndrome is thought to occur largely due to a dysregulated host immune response, however the pathogenesis is not completely understood [5]. To date there have only been a few systematic reviews on the topic, and although the syndrome is rare, the exact incidence is unknown [8]. It is thought MIS-C is more prevalent than MIS-A based on case numbers reported to the United States centers for disease Control and prevention (CDC). As of mid-2021, approximately 150 MIS-A cases and 3700 MIS-C cases have been reported to the CDC [9].
Here we present a literature review on MIS and a case series on MIS-A. The rationale for this work was to highlight key take home messages about the syndrome for the general surgeon, in the attempt to improve early recognition and to reduce associated morbidity and mortality.
A literature search was conducted through Ovid with the keywords 'MIS', 'COVID-19', and 'post COVID'.
The records of two cases of MIS-A were identified at our health service in 2022 and reviewed. These patients were included as they met the current CDC case definition (Table 1). This consists of: Recent evidence of COVID-19 infection in the form of a Reverse transcription polymerase chain reaction (RT-PCR) test, antigen test or serology, along with fever plus at least three of the clinical criteria, of which at least one must be a primary criteria [10]. The primary criteria consist of severe cardiac illness or rash with conjunctivitis. The secondary criteria consist of: Neurologic signs or symptoms, hypotension or shock; vomiting or diarrhoea, abdominal pain, and thrombocytopenia. Data regarding clinical presentation, investigation, intervention, and outcomes was obtained.
Table 1: MIS-A CDC case definition. View Table 1
A summary of clinical features, investigation results, interventions, and outcomes are presented in Table 2. The median age of the patients was 30.5 years. Both patients were females. Both patients had American Society of Anaesthesiology (ASA) scores of 2 (mild systemic disease). Both patients presented with abdominal pain and fevers, as well as tenderness in the right iliac fossa. Both had an absence of respiratory symptoms. Case one had a positive RT-PCR test at the time of admission. Case two had a negative RT-PCR at the time of admission, but had evidence of a positive RT-PCR documented from two months prior.
Table 2: Collated demographics and clinical findings for the case series. View Table 2
Both patients had a rise in C-reactive protein (CRP), cardiac troponin, and B-Type natriuretic peptide. Computed tomography (CT) scans for both patients showed enlarged right sided mesenteric lymph nodes and evidence of intestinal inflammation. Case one was admitted from the emergency department under the surgical team with undifferentiated abdominal pain for investigation. Diagnosis of MIS occurred on day eight of admission. Case two was admitted from the emergency department under the internal medicine team with prompt surgical review on the day of admission. The diagnosis was suspected from day one of admission, resulting in early input from the internal medicine and infectious disease teams.
There was an earlier diagnosis and treatment for case two compared with case one. Only case one required ICU admission and vasopressor support. Further, only case one showed systolic dysfunction on echocardiogram. However, case two showed new t-wave inversion on Electrocardiogram (ECG) and also had evidence of myocarditis on cardiac MRI that was performed many weeks after recovery. Both patients were treated with immunosuppressive agents (corticosteroid) and intravenous antibiotics. In addition, case two was treated with Intravenous immune globulin (IVIG). No in-patient mortality occurred. The mean duration of inpatient stay was 11.5 days.
MIS is a well described syndrome in children and adolescents, only recently has it been described in adults [5,11,12]. One of the first case reports was published in the Lancet and described the condition as a 'Kawasaki-like illness' because the afflicted patient met the American heart association criteria for Kawasaki disease [13]. The patient presented with fever, rash, and diarrhoea, having been exposed to COVID-19 two weeks earlier. Importantly the patient did not present with a predominance of respiratory symptoms.
The most common clinical features in MIS-A include: Fever, skin rash, hypotension, cardiac dysfunction, shortness of breath, abdominal pain, and diarrhoea [5,8]. However, as there is a wide spectrum for presentation the syndrome can be misdiagnosed. Both our cases had CT findings of intestinal inflammation and mesenteric lymphadenopathy as seen in Figure 2 [6]. Interestingly in our centres experience, the treating team's involvement with case one likely resulted in early recognition and referral to the appropriate medical team for case two. This likely resulted in prompt diagnosis and treatment. Case one however proved to be a diagnostic dilemma. Despite the involvement of multiple teams, this patient was planned for a diagnostic laparoscopy until the patient was tested for cardiac troponin, which revealed cardiac dysfunction. Echocardiogram was performed which showed systolic dysfunction. The patient was then diagnosed with MIS-A.
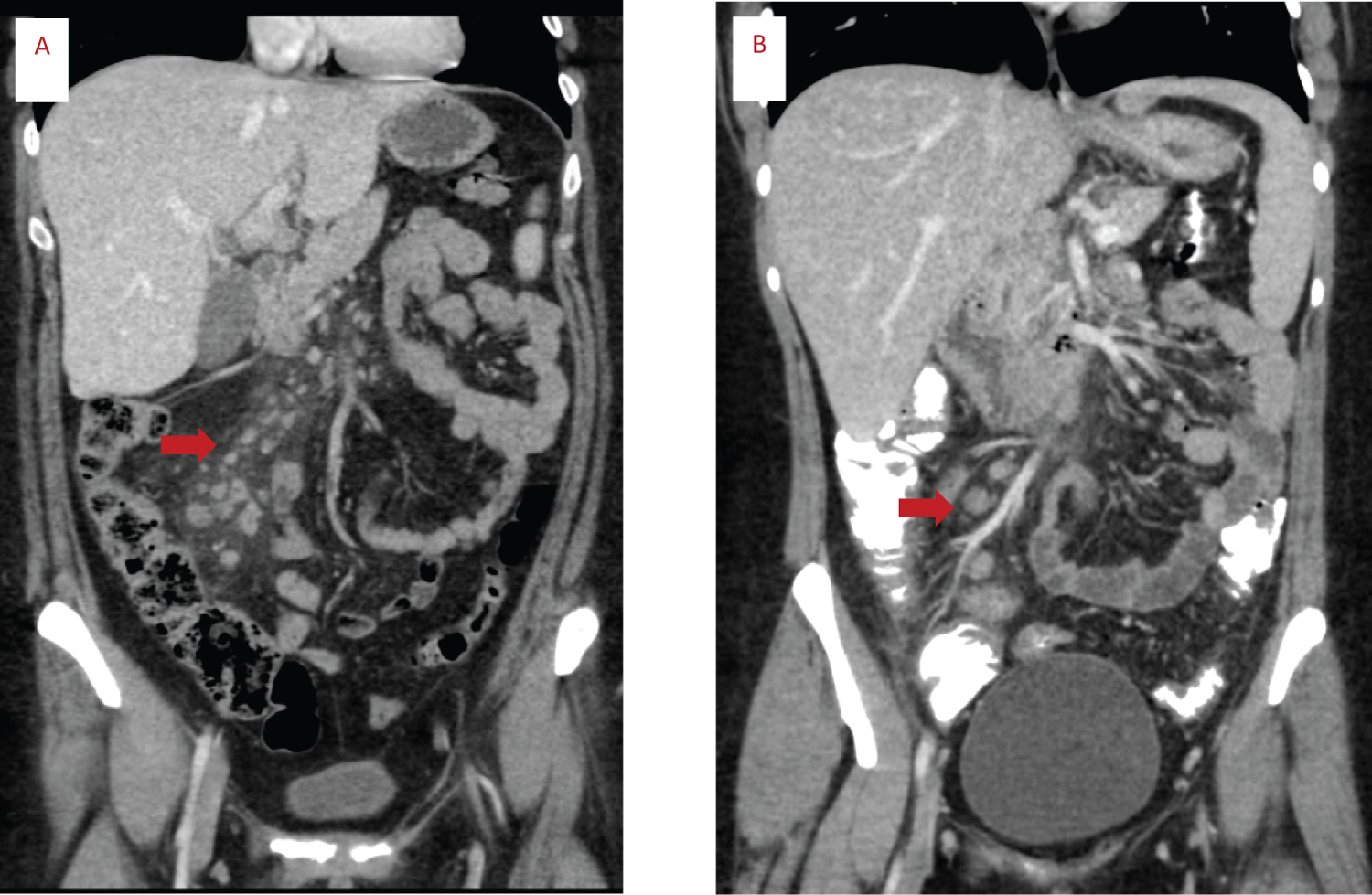 Figure 2: CT abdominal scans of case one (A) and two (B). Red arrow shows mesenteric lymphadenopathy.
View Figure 2
Figure 2: CT abdominal scans of case one (A) and two (B). Red arrow shows mesenteric lymphadenopathy.
View Figure 2
Because of the predominance of gastro-intestinal symptoms MIS can mimic an acute abdomen. In a recent systematic review 18.7% of MIS-C cases presented as an acute abdomen [7]. Approximately half of these patients underwent laparotomy which proved unnecessary in half of cases. In the other half of patients, the laparotomy proved necessary almost always for concurrent acute appendicitis. It is thought acute appendicitis is related to MIS due to the vasculitis and lymphocytic inflammation which can occur in MIS and lead to thrombus and ischaemic necrosis in the intestinal wall [7]. As appendicitis is more likely to occur in the younger MIS-C population compared to the MIS-A population, it may be reasonable to assume MIS-A patients are even less likely to require laparotomy for true surgical pathology.
As demonstrated in our series MIS-A patients can progress to multi-organ failure including heart failure requiring vasopressor support. It is not known whether early treatment for case two prevented the need for this support. In a recent systematic review it was shown that 51% of MIS-A patients required vasopressor support for shock [8]. The mortality rate for MIS-A ranges from 5-10% in the literature [5,8,9].
Many of the findings in our series are consistent with other case series and systematic reviews [5,9]. MIS-A is found to occur in young adults with a mean age of 32 years in a recent systematic review [5]. Furthermore most patients develop this syndrome within two to six weeks following exposure to COVID-19. In one review the mean time for MIS-A symptom onset following exposure to COVID-19 was 31.61 +/- 14.34 days [5]. Case one developed MIS-A symptoms three to four weeks following exposure to COVID-19, compared to two to three weeks for case two. Both patients also had a high C-reactive protein (CRP) level and deranged liver function tests which is commonly identified in studies [8].
Patients with MIS-A will have evidence of recent infection on RT-PCR and/or serology [10]. Some may still have a positive RT-PCR test despite being recovered from the acute phase of illness [9].Most cases have an absence of severe respiratory features [6]. Therefore, it is thought that this syndrome is a separate entity from the acute phase of the illness and is thought to explain why patients have recovered from their initial phase of infection by the time they develop MIS-A.
The pathophysiology of MIS is only partly understood. The SARS-CoV-2 virus primarily targets the Angiotensin-converting enzyme 2 (ACE2) receptor, which is a cell surface receptor on most bodily organs [2]. This extensive distribution of ACE2 receptor as well as the inflammatory response to the virus is thought to partly explain the extra-pulmonary manifestations of the acute illness [8]. MIS shares similarities with Kawasaki disease, Macrophage activation syndrome (MAS), and cytokine release syndrome [8]. It is thought to involve a dysregulated immune response to the virus. Potential mechanisms include: Reduced levels of neutralising antibodies and auto-reactive antibodies that promote inflammation [14]. Similarly, the mechanisms of myocardial injury are not understood, but coronary artery abnormalities may develop [6].
Further research into MIS-A is needed. There are no consensus guidelines for treatment. Treatment recommendations are based on expert recommendations for MIS-C [15]. However, most recommendations suggest immunosuppressant and immune modulator drugs. The most commonly used agents in the literature includes: corticosteroids, IVIG, biologics, anticoagulants, and antiplatelets [9]. As most patients have a similar presentation to those with sepsis, most are also treated with intravenous antibiotics initially.
It is worth noting that the timing of these cases was likely not by chance. This relatively rare syndrome occurred a few months after a peak in COVID-19 case numbers in January 2022 due to emergence of the new Omicron variant that evaded pre-existing population immunity [16]. Data shows that most MIS-C peaks occurred two to five weeks following COVID-19 peaks [9]. Although we are likely to continue to see sporadic cases we should maintain high suspicion following major surges in transmission with emergence of new variants that have significant antigenic variation from existing circulating variants. Furthermore, case one was not up to date with COVID-19 vaccination, and higher levels of protective antibodies are thought to be protective against this syndrome. This is based on the finding that more cases occur in unvaccinated individuals [9]. There is no evidence to date that shows COVID-19 vaccination can lead to MIS [9].
We present this series of this rare syndrome with a review of the literature to raise awareness of this potentially fatal condition. Our case series highlights the importance of early diagnosis and prompt management. Take home messages for the surgical team are to have a high index of suspicion for this condition in any surgical patient that presents with unexplained abdominal pain two to six weeks after COVID-19 infection. Test for cardiac dysfunction early in these patients. Involve the medical teams early so that treatment is not delayed.
There were no conflicts of interest from any author to declare. There was no financial or material support.
No funding was received for this work.
A.B. and R.K. conceived of the presented idea. A.B. wrote the manuscript with input from R.K, H.T, J.M, A.T, and J.Y.