Bariatric Surgery and Surgical Oncology Consultant, King Saud University, Saudi Arabia
Abstract
Background
Thyroid cancer is one of the most common endocrine malignancies secondary to ovarian cancer. Its incidence has surged swiftly than that of any other malignancy in recent years. Well-differentiated thyroid cancers (WDTC) are relatively common and usually slow-growing tumors with a good prognosis, including three types: Papillary, follicular, and Hürthle cell carcinoma. The first metastatic sites of these types of cancer typically involve lymph nodes, lungs, brain, and bones.
Aim
To address the unusual sites of metastasis of well-differentiated thyroid cancer, which were not discussed in the literature before.
Methods
The PICOT included adult men and women of 18 years and above, with the primary WDTC metastasized to unusual sites. MEDLINE, CINAHL, Cochrane Library, PubMed, Web of Science, Scopus, NCBI/PUBMED, Google Scholar were systematically screened for English language citations on human studies from 1990 to 2016.
Results
The case reports found in literature were summarized in the form of tables including 8 cases of choroid plexus metastases, 22 cases of retropharyngeal node metastases, 5 cases of ovarian metastases, 22 cases of renal metastases, 6 cases of breast metastases, 8 cases of pancreatic metastases, 21 cases of choroid metastases, 10 cases of pituitary metastases, 54 cases of cardiac metastases, and one case of testicular metastases.
Conclusion
Rare metastases of WDTC have been reported on distant sites such as kidneys, ovaries, heart, eyes, pancreas, pituitary, and testes. Major cases of uncommon metastases have been reported after several years of diagnosis of WDTC. Careful clinical diagnosis, along with advanced imaging techniques and immune-histopathological assays, can help to diagnose the type of tumor cells in host organs, which is essential for the development of treatment strategies.
Keywords
Well-differentiated, Rare, Metastasis, Hürthle cell, Thyroid
Introduction
Thyroid cancer is the second most common endocrine malignancy after ovarian cancer. Well-differentiated thyroid cancers (WDTC) are slow growing that have a good prognosis with proper treatment. It includes three entities, namely, papillary thyroid carcinoma (PTC), follicular thyroid carcinoma (FTC), and Hürthle cell carcinoma (HCC) [1]. The common metastasis sites for these types of cancer usually involve lymph nodes with 80% occurrence, lungs (49%), brain (0.4-1.2%), and bones (25%). In this systematic review, the unusual sites of metastasis of WDTC were addressed, which were not discussed in the literature previously. We reviewed the relevant literature of rare metastases in WDTC according to the methodology, treatment strategies, disease burden, mechanism of metastasis, genetic predisposition/SNPs predisposing to early metastasis, and pharmacotherapeutic strategies aiming at targeting early metastasis [2].
Methodology
The designed PICOT consisted of adult men and women age 18 years and above with primary WDTC metastasized to unusual sites. MEDLINE, CINAHL, Cochrane Library, PubMed, Web of Science, Scopus, NCBI/PUBMED, Google Scholar were systematically screened for English language citations on human studies from 1990 to 2016. Complete case reports, clinical studies, reviews, and full-text articles were included.
Search strategy
We searched the electronic databases to identify relevant literature using the search terms: 'Papillary thyroid carcinoma', 'follicular thyroid cancer', 'follicular thyroid carcinoma', 'follicular thyroid neoplasm', 'papillary thyroid cancer', 'unusual site of metastasis of well-differentiated thyroid cancer', 'Hürthle cell thyroid cancer', 'distal metastasis of well-differentiated thyroid cancer', 'rare metastasis', 'uncommon metastasis' and 'unusual course of well-differentiated thyroid cancer' Bibliography of relevant papers was also searched. Studies were screened according to pre-defined inclusion and exclusion criteria. Adults with WDTC metastasizing to sites other than lungs, brain, and bones were included. Patients of pediatric age group, undifferentiated thyroid cancer, or well-differentiated types that metastasize to bone, brain, lung, and/or metastasize to rare lymph nodes were excluded from the review. Two investigators independently reviewed the extracted studies, and a third reviewer was consulted for disagreements, if any.
Review process
Our literature search resulted in 654 articles. Two levels of screening were done that resulted in the inclusion of 105 and exclusion of 549 studies. The studies reporting common metastases and reviews of common metastatic sites were excluded. The studies reporting sites with less than 2% frequency of metastases from WDTC, providing a direct reference of original case reports with sufficient data of uncommon metastasis, were included in the review. Of the 549 excluded studies, 210 studies were excluded by the title, 305 by reading the abstract, and 34 were excluded after reading the full text (Figure 1).
A secondary reference was used to state cardiac metastases. Total studies cited were 105 that included 103 original case reports, one secondary reference for cardiac metastases, and one review article. The case reports found in the literature were summarized in the form of tables including eight cases of choroid plexus metastases, 22 cases of Retropharyngeal Node metastases, five cases of ovarian metastases, 22 cases of renal metastases, six cases of breast metastasis, eight cases of pancreatic metastases, 21 cases of choroid metastases, ten cases of pituitary metastases, 54 cases of cardiac metastases, and one case of testicular metastases.
Choroid plexus metastasis
Papillary carcinomas of thyroid origin are well-differentiated tumors, preferably using the lymphatic route for invasion, whereas vascular route for metastases and invasion is uncommon. Distant metastases in the case of PTC are rare and usually involve breasts and lungs, affecting the prognosis negatively [1]. Metastatic invaders use the hematogenous route to choroid plexus. The tumors reported for choroid plexus metastases are renal cell carcinomas and adenocarcinomas of lung [3]. Choroid plexus metastases from thyroid neoplasm especially in case of PTC are very rare. Eight cases of choroid plexus metastases have been reported by 2016. Table 1 summarizes the case reports reporting choroid plexus metastases from PTC.
Table 1: Literature review of 8 cases of choroid plexus metastasis from thyroid cancer. View Table 1
PTCs are characterized histopathologically based on the growth pattern, stromal attributes, and cell types. Brain metastases from PTC account for 0.1-5%, with a median survival rate of 12.4 months. Choroid plexus metastases are usually from the neoplasms that depict slow growth patterns, as shown by eight studies summarised in Table 1. However, aggressive variants of PTC are more prone to metastasize in uncommon sites. The seed and soil hypothesis of metastases and biological nature of metastatic invaders seems to play a role in choroid plexus metastases from well-differentiated slow-growing PTC.
Retropharyngeal node (nodes of Rouvière) metastasis
Metastatic invaders prefer the lymphatic route for traveling to the distant sites from thyroid neoplasm. Therefore, lymph node invasion and metastasis are not rare, but metastasis to retropharyngeal node (RPN) is uncommon, with a total number of 94 cases reported. Of these, 31 have been reported in the literature as comprehensive case studies, since 1970 and four of the case reports were for RPN metastases originated from medullary and anaplastic thyroid neoplasms. The majority of the cases reported papillary thyroid tumor mass as the primary tumor type. No clue was provided for RPN metastases either by the histopathological characterization or the size of the primary tumor. There were reports of microscopic tumors to aggressive papillary macro masses of thyroid tumors in the literature for RPN metastases. Table 2 summarises the comprehensive case reports from the literature regarding RPN metastases from thyroid carcinomas of classical variance.
Table 2: Review of published case series of RPN metastases from thyroid cancer. View Table 2
Ovarian metastasis
Papillary thyroid carcinomas rarely establish distant metastasis, and the ovarian metastasis is even rarer. Twenty cases have been reported in the literature, and among them, only four cases have been reported with detailed case reports and related information from 1929 to 2016. All the cases were unilateral in metastatic sites with only one exception. According to the seed and soil hypothesis, it is unusual for the follicular cancer cells to establish metastasis in ovaries compared to the papillary cells. The ovarian metastasis is usually reported decades after the primary tumor diagnosis leading to poor prognosis. Solitary ovarian metastasis is even rarer. Case reports of ovarian metastasis extracted from the literature are summarized in Table 3.
Table 3: Literature review of ovarian metastasis from thyroid carcinoma. View Table 3
Renal metastasis
Twenty-six cases of renal metastasis of WDTC have been reported in the literature so far. However, data is not available for four patients. Ahmed, et al. reported only one case of kidney metastasis out of 3500 patients tested from December 1975 to September 2005 [36]. Multimodal imaging was used to detect renal metastases of WDTC. Table 4 summarizes 22 cases of renal metastases.
Table 4: Characteristics and related data of patients with renal metastases from well-differentiated thyroid carcinoma. View Table 4
Breast metastasis
The occurrence of breast metastasis for WDTC is 1-2%. However; the solitary metastasis to the breast is very rare with one unusual case of the male patient, while all other cases were of female patients. In male patients, the breast metastasis, a rare occurrence has been diagnosed as invasive ductal carcinoma. To diagnose the cancer type before surgery, careful diagnosis and complete immune-histochemistry analysis can be helpful. However, it was neglected in this unique case. Table 5 summarises the case reports of breast metastases in WDTC and related details.
Table 5: Review of literature of breast metastasis from thyroid carcinoma. View Table 5
Pancreatic metastasis
Pancreatic cancer is a rare manifestation of thyroid carcinoma, which is often asymptomatic and usually presented as an abdominal ache. Ten cases of pancreatic metastasis from WDTC were found in the literature. However, the data is available for eight cases only, which is mentioned in Table 6. Additionally, the follicular variant of PTC has been reported for pancreatic cancer so far.
Table 6: Cases of pancreatic metastasis secondary to papillary thyroid carcinoma reported from 1991 to 2016. View Table 6
Choroid metastasis
Metastasis of WDTC to choroid and orbit does not occur frequently and mostly presented as long-term disease-associated survival and synchronous metastasis to various body sites. Choroid metastasis is mostly associated with papillary carcinoma, followed by medullary and follicular carcinomas. Ultrasonography, transillumination, computed tomography (CT), and/or magnetic resonance imaging (MRI) scanning are the main techniques used to diagnose choroid metastasis clinically. A summary of case reports of choroid metastasis from WDTC is described in Table 7.
Table 7: Choroid metastasis from well-differentiated thyroid cancer. View Table 7
Pituitary metastasis
Although lung cancer in men and breast cancer in women are associated with pituitary metastasis, yet pituitary metastasis is a rare complication of WDTC. Sufficient information about the use of imaging techniques for pituitary metastasis was not found in the literature. The diagnosis of this type of metastasis is generally delayed because the non-specific systemic symptoms (fatigue, nausea, and weight loss) of underlying malignancy and TSH suppression therapy hide hypopituitarism. Case reports have been summarized in Table 8 from literature reporting pituitary metastasis with WDTC.
Table 8: Pituitary metastases from thyroid malignancy. View Table 8
Cardiac metastasis
Cardiac metastasis from WDTC with a frequency of 0-2% has been associated with anaplastic thyroid carcinoma (ATC), closely followed by FTC, including HCC, & PTC. In the previous 130 years, 54 cases of WDTC have been reported with cardiac metastasis, which are summarized in Table 9 [104]. Follicular carcinoma, followed by papillary carcinoma, presents the major types for direct tumor invasion involving heart via the venous system.
Table 9: Cardiac metastasis from thyroid malignancy. View Table 9
Testicular metastasis
Testicular metastasis is not a common complication of WDTC, with only a single case report presented in 2014. The invasion of the testis by medullary thyroid cancer has not been reported before or after 2016. A 73-year-old Caucasian man was recommended for urologic surgery due to a nodule in the right testis. Histopathological and immune histopathological examinations revealed that lesions were due to WDTC metastasis [105].
Conclusion
Lungs and lymph nodes are usually overlooked as they are not the common sites of rare metastases. Therefore, major cases of rare metastasis are diagnosed late, which results in poor prognosis. Hence, it is essential to document and review the statistics, including their economic burden from time to time. The relevant data may be used to update guidelines for diagnosis and treatment. The rare metastases have been reported in kidneys, ovaries, eyes, pancreas, pituitary gland, heart, and testes in addition to the most common sites. It is imperative to look for the early clinical signs to rule out the involvement of the above-mentioned systems. Future research may help to predict rare instances of metastases and pave the way for early intervention.
Competing Interests Statement
Author declares no conflict of interest regarding this paper.
Funding Source
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
-
Koizumi J, Takano K, Obata K, Yamamoto K, Murayama K, et al. (2016) A clinical review of thyroid cancer at Sapporo Medical University Hospital. Adv Otorhinolaryngol 77: 88-91.
-
Ferrer GJ, Merino TJ, Ponce MJ, Piñón SF (2002) Unusual metastasis of differentiated thyroid carcinoma. An Med Interna 19: 579-582.
-
Wasita B, Sakamoto M, Mizushima M, Kurosaki M, Watanabe T (2010) Choroid plexus metastasis from papillary thyroid carcinoma presenting with intraventricular hemorrhage: Case report. Neurosurgery 66: E1213-E1214.
-
Heery CR, Engelhard HH, Slavin KV, Michals EA, Villano JL (2012) Unusual CNS presentation of thyroid cancer. Clinical Neurology and Neurosurgery 114: 1107-1109.
-
Kitagawa Y, Higuchi F, Abe Y, Matsuda H, Kim P, et al. (2013) Metastasis to the choroid plexus from thyroid cancer: Case report. Neurol Med Chir 53: 832-836.
-
Manzil FFP, Bender LW, Scott JW (2014) Evaluation of rare choroid plexus metastasis from papillary thyroid carcinoma with multimodality imaging. Clin Nucl Med 39: 551-553.
-
Healy AT, Otvos B, Schroeder J, Hamrahian AH, Angelov L, et al. (2014) Hurthle cell carcinoma presenting as a single choroid plexus metastasis. J Clin Neurosci 21: 1448-1450.
-
Sharifi G, Bakhtevari MH, Alghasi M, Nosari MA, Rahmanzade R, et al. (2015) Bilateral choroid plexus metastasis from papillary thyroid carcinoma: Case report and review of the literature. World Neurosurg 84: 1142-1146.
-
Wang X, Xu Z, Wu Y, Liu S, Yu Y (2012) Surgical management of parapharyngeal lymph node metastasis of thyroid carcinoma: A retrospective study of 25 patients. Chin Med J 125: 3635-3639.
-
Andrews GA, Kwon M, Clayman G, Edeiken B, Kupferman ME (2011) Technical refinement of ultrasound‐guided transoral resection of parapharyngeal/retropharyngeal thyroid carcinoma metastases. Head Neck 33: 166-170.
-
Kainuma K, Kitoh R, Yoshimura H, Usami S (2011) The first report of bilateral retropharyngeal lymph node metastasis from papillary thyroid carcinoma and review of the literature. Acta Otolaryngol 131: 1341-1348.
-
Kim JH, Kim MS, Yoo SY, Lim SM, Lee GH, et al. (2010) Stereotactic body radiotherapy for refractory cervical lymph node recurrence of nonanaplastic thyroid cancer. Otolaryngol Head Neck Surg 142: 338-343.
-
Kaplan S, Mandel S, Muller R, Baloch Z, Thaler E, et al. (2009) The role of MR imaging in detecting nodal disease in thyroidectomy patients with rising thyroglobulin levels. AJNR Am J Neuroradiol 30: 608-612.
-
Ma QD, Grimm K, Paz BI, Maghami E (2009) Transoral surgical approach for retropharyngeal node involvement in I-131-negative 18-fluoro-2-deoxyglucose positron emission tomography-positive recurrent thyroid cancer. Skull Base 19: 431-436.
-
Laccourreye L, Breheret R, Rohmer V, Dubin J, Bizon A (2008) Transoral resection of thyroid cancer metastasis to retropharyngeal lymph node. Ann Otolaryngol Chir Cervicofac 125: 309-312.
-
Le T, Cohen JI (2007) Transoral approach to removal of the retropharyngeal lymph nodes in well‐differentiated thyroid cancer. Laryngoscope 117: 1155-1158.
-
Otsuki N, Nishikawa T, Iwae S, Saito M, Mohri M, et al. (2007) Retropharyngeal node metastasis from papillary thyroid carcinoma. Head Neck 29: 508-511.
-
Shellenberger T, Fornage B, Ginsberg L, Clayman GL (2007) Transoral resection of thyroid cancer metastasis to lateral retropharyngeal nodes. Head Neck 29: 258-266.
-
Tomoda C, Matsuzuka F, Miyauchi A (2005) Parapharyngeal metastasis from papillary thyroid carcinoma: A case diagnosed by thyroglobulin measurement in peroral fine-needle aspiration of a cystic metastatic lymph node. J Laryngol Otol 119: 155-157.
-
Desuter G, Lonneux M, Plouin-Gaudon I, Jamar F, Coche E, et al. (2004) Parapharyngeal metastases from thyroid cancer. EJSO 30: 80-84.
-
Lombardi D, Nicolai P, Antonelli AR, Maroldi R, Farina D, et al. (2004) Parapharyngeal lymph node metastasis: An unusual presentation of papillary thyroid carcinoma. Head Neck 26: 190-196.
-
Erdem T, Miman M, Oncel S, Mizrak B (2003) Metastatic spread of occult papillary carcinoma of the thyroid to the parapharyngeal space: A case report. KBBID 10: 244-247.
-
Aygenc E, Kaymakci M, Karaca C, Ozdem C (2002) Papillary thyroid carcinoma metastasis to the parapharyngeal space. Eur Arch Otorhinolaryngol 259: 322-324.
-
Thomas G, Pandey M, Jayasree K, Pradeep V, Abraham E, et al. (2002) Parapharyngeal metastasis from papillary microcarcinoma of thyroid: Report of a case diagnosed by peroral fine needle aspiration. Br J Oral Maxillofac Surg 40: 229-231.
-
Ducci M, Bozza F, Pezzuto R, Palma L (2001) Papillary thyroid carcinoma metastatic to the parapharyngeal space. J Exp Clin Cancer Res 20: 439-441.
-
Leger A, Baillet G, Dagousset F, Vincenot M, Izembart M, et al. (2000) Upper retropharyngeal node involvement in differentiated thyroid carcinoma demonstrated by 131I scintigraphy. Br J Radiol 73: 1260-1264.
-
Imai T, Tanaka Y, Matsuura N, Takahashi M, Torii S (1999) Successful surgical treatment of a solitary parapharyngeal metastasis from thyroid cancer, using the mandibular swing-transcervical approach: Report of a case. Surg Today 29: 378-381.
-
Saydam L, Kalcioglu T, Demirkiran A, Gurer M (1999) Occult papillary thyroid carcinoma presenting as a parapharyngeal metastasis. AJO 20: 166-168.
-
Sirotnak JJ, Loree TR, Penetrante R (1997) Papillary carcinoma of the thyroid metastatic to the parapharyngeal space. Ear Nose Throat J 76: 342-344.
-
Ferrario F, Roselli R, Macchi A (1995) Occult thyroid carcinoma presenting as a parapharyngeal mass. J Laryngol Otol 109: 1204-1206.
-
Carrau RL, Myers EN, Johnson JT (1990) Management of tumors arising in the parapharyngeal space. Laryngoscope 100: 583-589.
-
Young RH, Jackson A, Wells M (1994) Ovarian metastasis from thyroid carcinoma 12 years after partial thyroidectomy mimicking struma ovarii: Report of a case. Int J Gynecol Pathol 13: 181-185.
-
Logani S, Baloch ZW, Snyder PJ, Weinstein R, Li Volsi VA (2001) Cystic ovarian metastasis from papillary thyroid carcinoma: A case report. Thyroid 11: 1073-1075.
-
Brogioni S, Viacava P, Tomisti L, Martino E, Macchia E (2007) A special case of bilateral ovarian metastases in a woman with papillary carcinoma of the thyroid. Exp Clin Endocrinol Diabetes 115: 397-400.
-
Corrado G, Pomati G, Russo A, Visca P, Vincenzoni C, et al. (2014) Ovarian metastasis from thyroid carcinoma: A case report and literature review. Diagnostic pathology 9: 1.
-
Ahmed M, Aslam M, Ahmed J, Faraz HA, Almahfouz A, et al. (2006) Renal metastases from thyroid cancer masquerading as renal angiomyolipoma on ultrasonography. J Ultrasound Med 25: 1459-1464.
-
Borde C, Basu S, Kand P, Arya S, Shet T (2010) Bilateral renal metastases from papillary thyroid carcinoma on post 131I treatment scan: Flip-flop sign, radioiodine SPET, 18F-FDG PET, CECT and histopathological correlation. Hell J Nucl Med 14: 72-73.
-
Malhotra G, Upadhye TS, Sridhar E, Asopa RV, Garde PS, et al. (2010) Unusual case of adrenal and renal metastases from papillary carcinoma of thyroid. Clin Nucl Med 35: 731-736.
-
Djekidel M, Gordon M, Shah RB, Gross MD, Avram A (2010) Renal metastasis from hurthle cell thyroid carcinoma and its evaluation with hybrid imaging. Thyroid 20: 429-433.
-
Luo Q, Luo QY, Sheng SW, Chen LB, Yu YI, et al. (2008) Localization of concomitant metastases to kidney and erector spinae from papillary thyroid carcinoma using 131I-SPECT and CT. Thyroid 18: 663-664.
-
Von Falck C, Beer G, Gratz KF, Galanski M (2007) Renal metastases from follicular thyroid cancer on SPECT/CT. Clin Nucl Med 32: 751-752.
-
Kumar A, Nadig M, Patra V, Srivastava DN, Verma K, et al. (2005) Adrenal and renal metastases from follicular thyroid cancer. Br J Radiol 78: 1038-1041.
-
Iwai H, Ohno Y, Ito H, Kiyokawa T, Aoki N (2005) Renal rupture associated with a poorly differentiated follicular thyroid carcinoma metastasizing to the thigh muscle, lung and kidney. Intern Med 44: 848-852.
-
Liou MJ, Lin JD, Chung MH, Liau CT, Hsueh C (2005) Renal metastasis from papillary thyroid microcarcinoma. Acta Otolaryngol 125: 438-442.
-
Inahara M, Mikami K, Tobe T, Suzuki H, Itou H (2002) A case of thyroid cancer metastasizing to the bilateral kidneys. Hinyokika kiyo 48: 315-317.
-
Smallridge RC, Castro MR, Morris JC, Young PR, Reynolds JC, et al. (2001) Renal metastases from thyroid papillary carcinoma: Study of sodium iodide symporter expression. Thyroid 11: 795-804.
-
Garcia-Sanchis L, Lopez-Aznar D, Oltra A, Rivas A, Alonso J, et al. (1999) Metastatic follicular thyroid carcinoma to the kidney: A case report. Clin Nucl Med 24: 48-50.
-
Benchekroun A, Lachkar A, Alami M, Iken A, Soumana A, et al. (1998) Thyroid cancer metastasizing to the kidney. Report of a case. Annales d'urologie.
-
Lam KY, Ng WK (1996) Follicular carcinoma of the thyroid appearing as a solitary renal mass. Nephron 73: 323-324.
-
Graham LD, Roe SM (1995) Metastatic papillary thyroid carcinoma presenting as a primary renal neoplasm. Am Surg 61: 732-734.
-
Ro H, Ha H, Kim H, Shinn K (1995) Renal metastasis from thyroid carcinoma visible as a hyperdense lesion on unenhanced CT. AJR Am J Roentgenol 165: 1018.
-
Tur GE, Asanuma Y, Sato T, Kotanagi H, Sageshima M, et al. (1994) Resection of metastatic thyroid carcinomas to the liver and the kidney: Report of a case. Surg Today 24: 844-848.
-
Sardi A, Agnone C, Pellegrini A (1992) Renal metastases from papillary thyroid carcinoma. JLSMS 144: 416-420.
-
Marino G, Cocimano V, Taraglio S, Testori O (1990) Metastasis of thyroid carcinoma. A rare case of secondary renal tumor. IJN 43: 85-88.
-
Johnson M, Morettin L, Sarles H, Zaharopoulos P (1982) Follicular carcinoma of the thyroid metastatic to the kidney 37 years after resection of the primary tumor. J Urol 127: 114-146.
-
Davis RI, Corson JM (1979) Renal metastases from well differentiated follicular thyroid carcinoma. A case report with light and electron microscopic findings. Cancer 43: 265-268.
-
Takayasu H, Kumamoto Y, Terawaki Y, Ueno A (1968) A case of bilateral metastatic renal tumor originating from a thyroid carcinoma. J Urol 100: 717-719.
-
Al-Abed Y, Gray E, Wolfe K, Watters GW, Philpott JM (2008) Metastatic hurthle cell carcinoma of the thyroid presenting as a breast lump: A case report. Int Semin Surg Oncol 5: 14.
-
Angeles-Angeles A, Chable-Montero F, Martinez-Benitez B, Albores-Saavedra J (2009) Unusual metastases of papillary thyroid carcinoma: Report of 2 cases. Ann Diagn Pathol 13: 189-196.
-
Chisholm RC, Chung E, Tuckson W, Khan T, White JE (1980) Follicular carcinoma of the thyroid with metastasis to the breast. J Natl Med Assoc 72: 1101-1104.
-
Vizcaino I, Torregrosa A, Higueras V, Morote V, Cremades A, et al. (2001) Metastasis to the breast from extramammary malignancies: A report of four cases and a review of literature. Eur Radiol 11: 1659-1665.
-
Farmer P, Bonnefoi H, Becette V, Tubiana-Hulin M, Fumoleau P, et al. (2005) Identification of molecular apocrine breast tumours by microarray analysis. Breast Cancer Research 7: 1.
-
Cristallini EG, Bolis GB, Francucci M (1989) Diagnosis of thyroid metastasis of colonic adenocarcinoma by fine needle aspiration biopsy. Acta Cytol 34: 363-365.
-
Zhu Z, Gandhi M, Nikiforova MN, Fischer AH, Nikiforov YE (2003) Molecular profile and clinical-pathologic features of the follicular variant of papillary thyroid carcinoma. Am J Clin Pathol 120: 71-77.
-
Sugimura H, Tamura S, Kodama T, Kakitsubata Y, Asada K, et al. (1991) Metastatic pancreas cancer from the thyroid; clinical imaging mimicking non functioning islet cell tumor. Radiat Med 9: 167-169.
-
Jobran R, Baloch ZW, Aviles V, Rosato EF, Schwartz S, et al. (2000) Tall cell papillary carcinoma of the thyroid: Metastatic to the pancreas. Thyroid 10: 185-187.
-
Borschitz T, Eichhorn W, Fottner C, Hansen T, Schad A, et al. (2010) Diagnosis and treatment of pancreatic metastases of a papillary thyroid carcinoma. Thyroid 20: 93-98.
-
Chen L, Brainard JA (2011) Pancreatic metastasis from papillary thyroid carcinoma diagnosed by endoscopic ultrasound-guided fine needle aspiration. Acta Cytolog 54: 640-644.
-
Alzahrani AS, AlQaraawi A, Al Sohaibani F, Almanea H, Abalkhail H (2012) Pancreatic metastasis arising from a BRAF V600E-positive papillary thyroid cancer: The role of endoscopic ultrasound-guided biopsy and response to sorafenib therapy. Thyroid 22: 536-541.
-
Tunio MA, Al Asiri M, Riaz K, AlShakweer W (2013) Pancreas as delayed site of metastasis from papillary thyroid carcinoma. Case reports in gastrointestinal medicine.
-
Ritland J, Eide N, Walaas L, Høie J (1999) Fine‐needle aspiration biopsy diagnosis of a uveal metastasis from a follicular thyroid carcinoma. Acta Ophthalmol Scand 77: 594-596.
-
Scott AW, Cummings TJ, Kirkpatrick JP, Mruthyunjaya P (2007) Choroidal metastasis of follicular thyroid adenocarcinoma diagnosed by 25-gauge transretinal biopsy. Ann Ophthalmol 40: 110-112.
-
Slamovits TL, Mondzelewski J, Kennerdell JS (1979) Thyroid carcinoma metastatic to the globe. Br J Ophthalmol 63: 169-172.
-
Arat YO, Boniuk M (2007) Red lesions of the iris, choroid, and skin secondary to metastatic carcinoma of the thyroid: A review. Surv Ophthalmol 52: 523-528.
-
Seneviratne DR, Stavrou P, Good P (2011) Late-stage metastasis to the choroid from follicular thyroid carcinoma-case report. Optometry 82: 215-217.
-
Dutton JJ, Barbour HL (1994) Hürthle cell carcinoma metastatic to the uvea. Cancer 73: 163-167.
-
Biswas J, Kumar SK, Shanmugam MP, Raghavendran SR (2000) Clear cell thyroid carcinoma metastatic to choroid: Clinicopathological study of a case. Eye 14: 394-395.
-
Avram AM, Gielczyk R, Su L, Vine AK, Sisson JC (2004) Choroidal and skin metastases from papillary thyroid cancer: Case and a review of the literature. J Clin Endocrinol Metab 89: 5303-5307.
-
Anteby I, Pe'er J, Uziely B, Krausz Y (1992) Thyroid carcinoma metastasis to the choroid responding to systemic 131I therapy. Am J Ophthalmol 113: 461-462.
-
Ahmadi MA, Nicholes D, Esmaeli B (2001) Late choroidal metastasis secondary to papillary thyroid carcinoma. AJO 132: 796-798.
-
Bucerius J, Meyka S, Bangard M, Biersack H, Eter N (2008) Papillary thyroid carcinoma with an uncommon spread of hematogenous metastases to the choroid and the skin. J Natl Med Assoc 100: 104-107.
-
Tran K, Bigby KJ, Hughes BG, Lee L, Allison R (2011) Clinicopathological report: Bilateral choroidal metastases from papillary thyroid cancer. Asia Pac J Clin Oncol 7: 11-14.
-
Singh U, Kaushik S, Pandav SS, Dogra MR, Powari M, et al. (2003) Papillary carcinoma thyroid presenting as a choroidal metastasis. Report of a case and brief review of literature. Indian J Ophthalmol 51: 81-83.
-
Yunta Abarca PJ, Ponce JL, Prieto M, López-Aznar D, Sancho-Fornos S (1999) Papillary thyroid carcinoma that metastasised to the choroid. Eur J Surg 165: 998-999.
-
Søndergaard Pedersen JH, Schaffalitzky De Muckadell O (2007) Choroidal metastases in multiple endocrine neoplasia type 2B. Acta Ophthalmol Scand 85: 120-121.
-
Shields JA, Shields CL, Perez N (2002) Choroidal metastasis from medullary thyroid carcinoma in multiple endocrine neoplasia. Am J Ophthalmol 134: 607-609.
-
Rosário F, Garrao A, Laranjeira J, Bugalho M, Limbert E, et al. (2005) Choroidal metastasis from sporadic medullary thyroid carcinoma. Thyroid 15: 1401-1402.
-
Bianciotto CG, Demirci HY, Shields CL, Shields JA (2008) Simultaneous eyelid and choroidal metastases 36 years after diagnosis of medullary thyroid carcinoma. Ophthalmic Plast Reconstr Surg 24: 62-63.
-
Yildiz I, Sen F, Tuncer S, Kilic L, Basaran M, et al. (2011) Optic disc and choroidal metastasis from sporadic medullary thyroid carcinoma: Case report and review of the literature. ORT 34: 630-633.
-
Palm SE, Paridaens D (2007) Posterior uveal metastases from medullary thyroid carcinoma. Retina 27: 115-116.
-
Ozpacaci T, Mulazimoglu M, Tamam MO, Leblebici C, Yildiz K, et al. (2012) Intraocular and orbital metastasis as a rare form of clinical presentation of insular thyroid cancer. Ann Endocrinol 73: 222-224.
-
Puri P, Motwani N, Pande M (2001) Squamous carcinoma of the thyroid metastatic to the choroid: A report. Eur J Cancer Care 10: 63-64.
-
Bell CD, Kovacs K, Horvath E, Smythe H, Asa S (2001) Papillary carcinoma of thyroid metastatic to the pituitary gland. APLM 125: 935-938.
-
Chrisoulidou A, Pazaitou-Panayiotou K, Flaris N, Drimonitis A, Giavroglou I, et al. (2004) Pituitary metastasis of follicular thyroid carcinoma. HRP 61: 190-192.
-
Palosi R, Romaldini J, Massuda L, Reiss L, Franca L (1977) Panhipopituitarismo por metástase de carcinoma papilifero da tiroide, com tromboflebite secundária de seio cavernoso leptomeningite purulenta. Rev Ass Med Brasil 23: 277-280.
-
Sziklas JJ, Mathews J, Spencer RP, Rosenberg RJ, Ergin M, et al. (1985) Thyroid carcinoma metastatic to pituitary. JNM 26: 1097.
-
Masiukiewicz US, Nakchbandi IA, Stewart AF, Inzucchi SE (1999) Papillary thyroid carcinoma metastatic to the pituitary gland. Thyroid 9: 1023-1027.
-
Trunnell J, Marinelli L, Duffy Jr B, Hill R, Peacock W, et al. (1949) The treatment of metastatic thyroid cancer with radioactive iodine: Credits and debits. J Clin Endocrinol Metab 9: 1138-1152.
-
Johnson PM, Atkins HL (1965) Functioning metastasis of thyroid carcinoma in the sella turcica. J Clin Endocrinol Metab 25: 1126-1130.
-
Kistler M, Pribram HW (1975) Metastatic disease of the sella turcica. American Journal of Roentgenology 123: 13-21.
-
Ochiai H, Nakano S, Goya T, Wakisaka S, Kinoshita K (1992) Pituitary metastasis of thyroid follicular adenocarcinoma-Case report. Neurologia Medico-Chirurgica 32: 851-853.
-
Yilmazlar S, Kocaeli H, Cordan T (2004) Sella turcica metastasis from follicular carcinoma of thyroid. Neurol Res 26: 74-78.
-
Simon N, Quyyumi SA, Rothman JG (2004) Follicular thyroid cancer presenting as a sellar mass: Case report and review of the literature. Endocr Pract 10: 62-66.
-
Catford SR, Lee KT, Pace MD, Marasco SF, Longano A, et al. (2011) Cardiac metastasis from thyroid carcinoma. Thyroid 21: 855-866.
-
Appetecchia M, Barnabei A, Pompeo V, Sentinelli S, Baldelli R, et al. (2014) Testicular and inguinal lymph node metastases of medullary thyroid cancer: A case report and review of the literature. BMC Endocr Disord 14.
Citation
Alqahtani A (2021) Unusual Sites of Metastasis of Well-Differentiated Thyroid Cancer: A Systematic Review. Int J Surg Res Pract 8:122. doi.org/10.23937/2378-3397/1410122
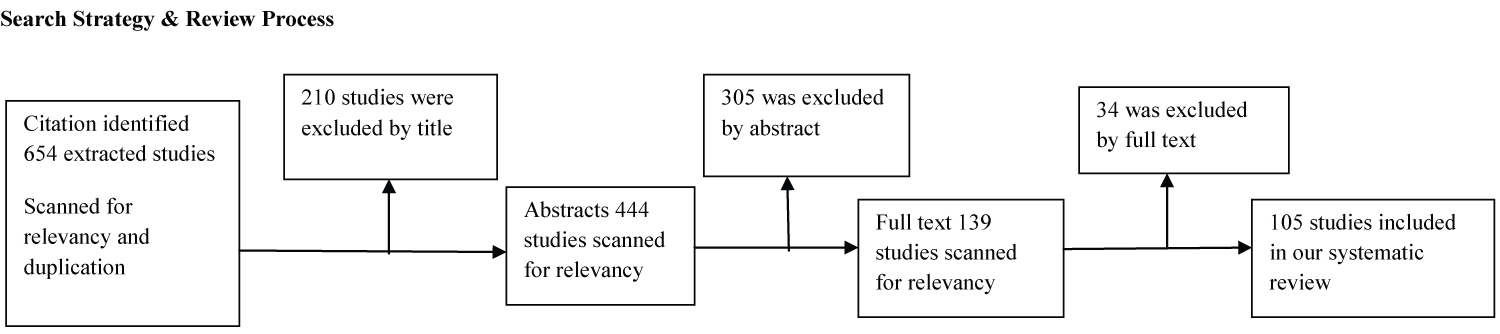 Figure 1: Review process algorithm.
View Figure 1
Figure 1: Review process algorithm.
View Figure 1