Objectives: Venous thromboembolism (VTE) is a rare but potentially life-threatening complication of superficial endovenous treatment. Use of VTE risk assessment to guide pharmacological prophylaxis could mitigate this danger. However, currently there is no accepted management of VTE risk in these, usually fit, ambulatory patients.
Methods: We retrospectively reviewed our use of Worcester score (VTE risk assessment tool) in all patients who underwent endovenous thermal ablation using the bipolar radiofrequency device (radiofrequency induced thermal therapy, RFITT) from January 2013 to December 2018. All cases were performed by a single Vascular consultant at a single NHS trust. Patient demographics, treatment parameters and VTE prophylaxis method were retrospectively analysed from a prospectively collected database.
Results: 481 patients who underwent RF ablation between 2013 and 2018 were assessed. There were no clinical or duplex detected DVTs. 436 patients (90.6%) had a Worcester score of '0' and were not given any additional pharmaco-prophylaxis. 42 patients (8.8%) had positive scores and were treated with extended anticoagulation. Of the 42 patients, 18 (40%) scored 1 and were given 7 days of additional prophylaxis and 24 (60%) scored 2 or more and were treated for two or more weeks.
Conclusions: VTE is a life-threatening complication of ambulatory endovenous treatment. The current state of pharmacological thromboprophylaxis practice is highly variable and subjective. A selective VTE prevention strategy which involves risk-assessing all patients for VTE and managing those at increased risk with additional anticoagulant prophylaxis extended into the post-procedure period is a safe and effective strategy based on our experience.
Varicose vein, Endothermal ablation, Deep venous thrombosis, Venous thromboembolism
Venous thromboembolism (VTE) presents a serious threat to some patients undergoing ambulatory thermal ablation for superficial venous incompetence. VTE most commonly presents as deep venous thrombosis (DVT) however, rarely, VTE can present as pulmonary embolism (PE) or paradoxical stroke [1]. These serious complications can result in the death of relatively young, fit patients thereby attracting media coverage [2,3]. In the UK all periprocedural deaths are investigated by the Coroner and lack of evidence of VTE risk assessment and of VTE risk having been discussed with the patient will lead to scrutiny of the clinician's practice [4].
It is difficult to accurately quantify patient's VTE risk. Because VTE occurs infrequently events may be absent from some case series purely on the bases of chance. Another issue is that clinicians with higher VTE rates are less likely to publish their results or be involved in clinical trials. Historically, DVT incidence has been reported to be as high as 16% however more recent data suggests an incidence of between 0.5% and 4.4% [5-8]. There is a reported mortality of up to 1% when DVT occurs [6].
The logical approach to managing VTE risk would be to risk-assess all patients with the aim of identifying those who have increased VTE risk factors for targeted anticoagulant prophylaxis. Currently there is no guidance for such VTE risk management in this group of ambulatory, relatively fit patients who nevertheless, on rare occasions, die after these minimally invasive procedures.
Several patient factors have been reported to increase VTE risk after varicose veins procedures. However existing publications are confusing and conflicting as to what the important risk factors may be, and global VTE guidelines from the likes of UK's NICE and USA's ACCP do not address VTE risk management after ambulatory venous intervention [9,10]. Unsurprisingly there is no agreement amongst clinicians on which risk factors to use to identify high risk patients, or what diagnostic criteria should guide thromboprophylaxis practice. This uncertainty has resulted in some clinicians failing to manage and others even failing to acknowledge VTE risk in these patients.
On this confused background the aim of this study was to assess our use of a local VTE risk scoring assessment (The Worcester Score) in patients undergoing ambulatory endovenous thermal ablation, with the hope of increasing debate and research in this important aspect of endovenous practice [11].
In the absence of any simple practical VTE risk assessment model we have proposed a tool specifically directed at ambulatory patients undergoing endovenous procedures under local anaesthesia. We have used two VTE risk factor categories in this Worcester score as follows (Table 1): A high risk factor group consisting of a history of VTE, known thrombophilia and target limb immobility each scoring 2 points, and a moderate risk factors group of obesity, relevant hormone therapy (Combined hormonal contraception or Oral oestrogen treatment in menopause) and a history of superficial vein thrombosis, each scoring 1 point. Any history of a pre-existing pro-thrombotic systemic conditions such as cancer, inflammatory arthritis, or inflammatory bowel diseases is classified as high risk and also scores 2 points. A patient's overall VTE risk score is then classified simply as low, moderate or high risk based on total scores of 0, 1 or ≥ 2, and then managed accordingly (Table 2).
Table 1: VTE risk factor categories in this Worcester score, note that patients with a history of cancer or inflammatory conditions like IBD or rheumatoid arthritis are automatically classified as high risk. View Table 1
Table 2: Patient categories based on their Worcester score. View Table 2
We retrospectively reviewed our use of the Worcester score in all patients who underwent endovenous thermal ablation using the bipolar radiofrequency device (radiofrequency induced thermal therapy, RFITT) from January 2013 to December 2018. All patients were managed in a single vascular consultant's NHS practice. Patients underwent radiofrequency endothermal ablation of saphenous truncal veins in a single NHS Hospital Trust. No phlebectomy was performed in this cohort of patients, however, those who had treatment for C5 and C6 disease had additional foam sclerotherapy to the venous plexus related to the active ulcer or healed ulcer bed. Post procedure, treated legs were dressed by application of compression bandaging that was exchanged for compression hosiery after 48 hours, with instruction for this to be worn for a minimum of two weeks. C6 patients continued with their pre-intervention compression regime after 48 hours. All procedures were ambulatory and patients were discharged home within 30 min of returning to the ward, with instructions advising immediate and frequent ambulation. No analgesia was prescribed but patients were advised, if required, to take paracetamol, then add Co-codamol and then ibuprofen as required and tolerated. Patients were reviewed after 6 weeks (2 weeks if they were part of the 3RF randomised trial protocol [12]. DUS was not routinely performed except in the 3RF trial patients. Patient demographics, treatment parameters and VTE prophylaxis management were collected on a prospective database and analysed retrospectively for this report.
For descriptive statistics, quantitative variables were expressed as mean and standard deviation; qualitative variables were expressed as frequencies and percentages. All data analyses were performed using SPSS (version 22, IBM®) and Excel (version 2011, Microsoft®).
The study was conducted as part of an audit of clinical practice and the study was approved by the institution’s Audit and Quality Improvement department.
Database records of four hundred and eighty one patients who underwent RF ablation between 2013 and 2018 and were assessed. Their mean age was 54.40 years (SD 14.58) and 269 (56%) were women. Patient's CEAP classes were as follows: 70% C2, 7% C3, 16% C4, 6% C5 and 1% C6.
Patients had ablation to Great Saphenous (85%), Small Saphenous (9%) and Anterior accessory Saphenous (6%) veins. Mean diameters and mean lengths were GSV: 7.4 mm (SD 2.1) and 32.6 cm (SD 10.7), SSV: 6.6 mm (SD 1.6) and 23.4 cm (SD 6.9) and AASV: 6.4 mm (SD 1.6) and 18.3 cm (SD 8.4).
There were no clinical or duplex detected DVTs in this series. Three patients presented to their general practitioner complaining of discomfort and ipsilateral leg swelling. In all cases this occurred in the week after compression had been discontinued. All underwent duplex scanning in the general imaging department without reference to the vascular team. No DVT was diagnosed however in every case the treated truncal vein was misdiagnosed as superficial vein thrombosis (SVT) and patients were commenced on Apixaban. This treatment was stopped as soon as the vascular department was made aware of their presentation.
436 patients (90.6%) scored '0' and were not given any additional anticoagulant medication. 42 patients (8.8%) had positive scores and were given additional extended anticoagulant prophylaxis. Another 3 (0.6%) patients who scored zero, two long haul pilots returning to work within 2 weeks and one woman with polycystic ovary disease (PCOD) and a BMI of 29, were treated “out of protocol” with additional anticoagulant prophylaxis (Figure 1).
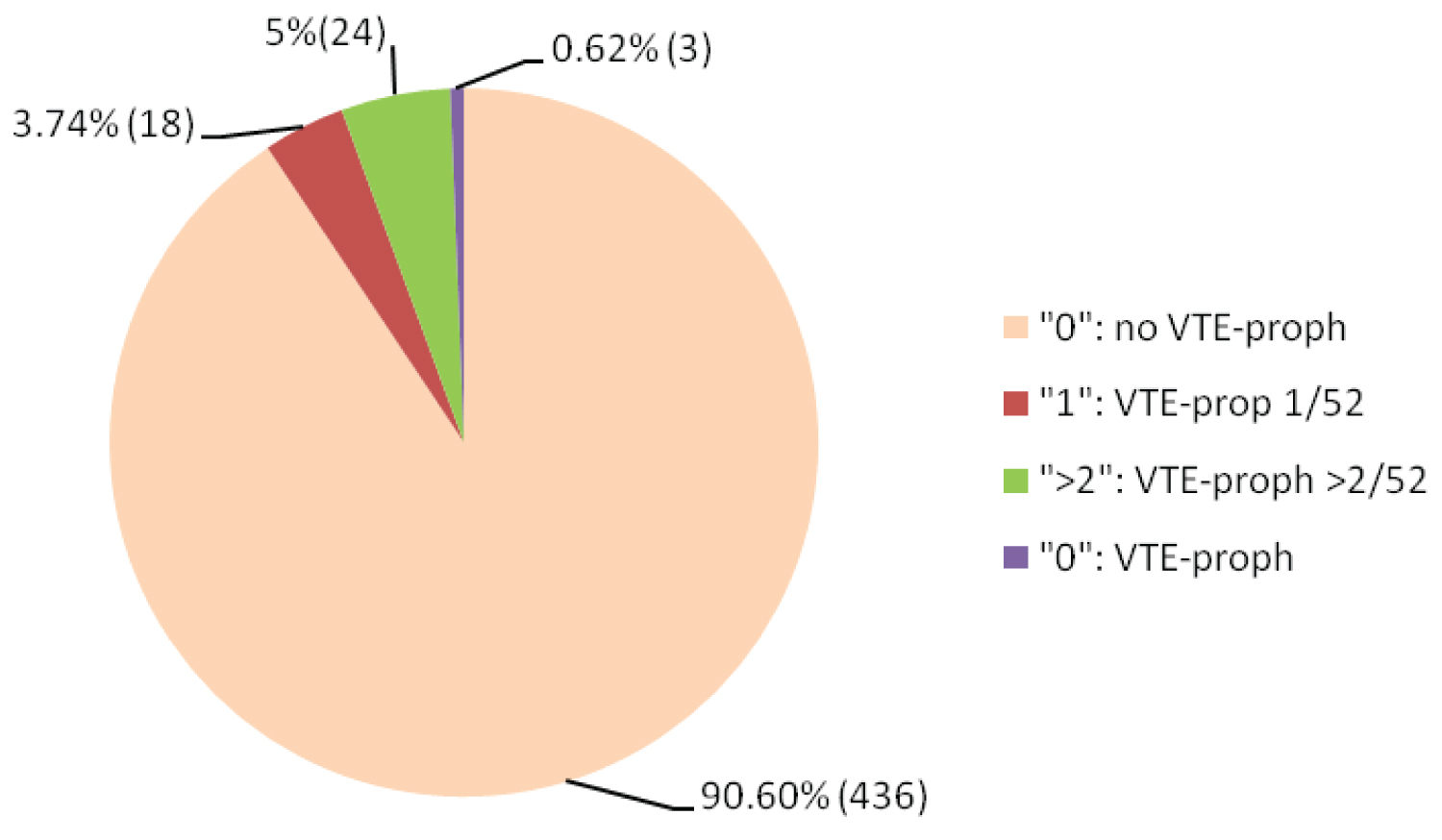 Figure 1: Worcester score of the patients in our series and their VTE prophylaxis.
View Figure 1
Figure 1: Worcester score of the patients in our series and their VTE prophylaxis.
View Figure 1
Overall there were 71 scoring risk factors in 42 patients (Figure 2). Target limb immobility was the most common high risk factor and obesity (BMI ≥ 30) was the commonest intermediate risk factor. From the high risk factor group there were 6 patients with previous history of DVT, 2 with Factor V Leiden and 16 with ipsilateral calf pump compromise (Table 3 and Table 4). From the intermediate risk group 9 patients had had SVT, 19 were clinically obese and 7 were on relevant hormonal therapy (4 on oral oestrogen based HRT, 3 were on combine oral contraception therapy) (Table 3). Of the 8 patients with past malignancy 3 had had breast, 2 cervical, 2 prostate and one colonic cancer, and for those with inflammatory condition 3 had ulcerative colitis and one had Crohn's disease.
 Figure 2: Risk category using the worcester score.
View Figure 2
Figure 2: Risk category using the worcester score.
View Figure 2
Table 3: Breakdown of the risk factors (n = 71) among the scoring patients. View Table 3
Table 4: Causes of calf pump dysfunction in patients with reduced target limb mobility. View Table 4
Of the 42 scoring patients who were given low-molecular weight heparin (LMWH) 18 (40%) scored 1 and were given 7 days of additional anticoagulation prophylaxis and 24 (60%) scored 2or more and were treated for two or more weeks. In addition the patient with PCOD had two weeks of LMWH and the two long haul pilots were given multiple courses of LMWH (3 days each) to cover flights during the first 3 weeks.
VTE remains a rare but real threat to patients undergoing ambulatory endovenous treatment and is likely to remain problematic because endovenous treatments for SVI continue to rise [13,14]. A report from the voluntary US Manufacturer & User Database to which only a minority of clinicians contribute recorded 123 DVTs, 30 PEs, and 7 deaths after thermal ablation procedures over a 12 year period [15]. Further proof of serious VTE events in this patient group comes from O'Donnell's report from another US healthcare database that recorded DVT rates of 3 and 4.4% after laser and RF ablation respectively. Mortality was approximately 1% in those who developed DVT [6].
Currently, the decision as to whether patients undergoing superficial endovenous treatment should receive anti-VTE pharmacoprophylaxis tends to be based on individual clinician preference and may be perpetuated from historical or anecdotal practice rather than objective criteria, due to absence of relevant guidelines [4,16].
There is no specific tool with which to stratify VTE risk in patients undergoing endovenous treatment to superficial veins. Existing global risk assessment tools such as those by Caprini or UK Department of Health are not specific for ambulatory patients undergoing endovenous procedures under local anaesthesia [10,17]. Most of their scoring risk factors best apply to in-patients and those undergoing major surgical intervention under general anaesthesia. The search for more relevant risk factors in ambulatory endovenous patients has proved challenging. Currently no agreement exists as to which risk factors best identify high risk patients, nor on diagnostic criteria to guide thromboprophylaxis practice. Puggioni reported large GSV diameter, previous SVT and the addition of phlebectomies to be significant VTE risk factors but he did not find previous DVT to be significant [18]. In direct contrast Jacobs found previous history of DVT to be the only predictive risk factors for VTE but not age, gender, Factor V Leiden, hormonal therapy or vein diameter [19]. Chi initially identified female gender, hyperlipidaemia, a history of DVT and SVT to be predictive however following step-wise logistic regression analysis only age, female gender and a history of SVT remained predictive [20]. Lurie identified only large GSV diameter to be a risk factor. He found no significant association with age, obesity, or family history of VTE [21]. International Phlebology guidelines variably list previous DVT, cancer, thrombophilia, obesity, SVT, immobility, age and the hormonal therapy as relevant risk factors. However they provide no relative stratification or scoring system for using these to define VTE risk in an individual patient. Further, they all go on to make relatively weak recommendations for treatment even when VTE risk factors exist [22-24].
Our retrospective review has shown that in using the Worcester score approximately 10% of patients undergoing endovenous treatment had one or more VTE risk factors. However the vast majority (90%) scored zero and were not given additional anticoagulant prophylaxis. The Worcester score produces two predetermined categories of elevated risk (moderate risk and high risk) that we used to inform duration of prophylaxis management. However, this study did not compare the impact of one risk factor over another or the effect of multiple co-existing risk factors beyond the basic combinations described. Also, our extended prophylactic management regime (one week for moderate risk and ≥ 2 weeks for high risk) has no published evidential bases from endovenous practice because no such evidence exists. What is known is that giving patients single dose heparin prophylaxis as exemplified by the case of major paradoxical stroke reported by Spinedi does not provide effective protection and is not recommended by haematologists [1]. This common UK approach likely reflects learned historic vascular practice that was originally promoted to aid medico-legal defence rather than providing effective clinical benefit for the patient. In a recent UK survey that asked about treatment intentions 52% of clinicians indicated that they would offer only single dose LMWH to patients who had been risk stratified as moderate risk [25].
There is indirect evidence to support prolongation of VTE prophylaxis beyond the immediate peri-procedure period in publications that have shown that incidence of post-operative VTE is prolonged beyond the immediate peri-operative period. Using data from the Million Women Study, Sweetland showed that the post-operative risk of VTE after a day-case procedure remains elevated for up to 6 weeks [26]. Similar delayed presentation has been shown by Pannucci in a report from plastic surgery cases, where DVTs presented out to 40 days post-procedure [27]. After varicose veins intervention Sutton's study from NHS Hospital Episode statistics data showed a median time to presentation for the 126 patients who developed DVT to be 11 days and Barker's analysis also from NHS data showed that following superficial venous intervention, the majority of VTEs presented within 30 days of intervention [7,28]. These studies all suggest that once a patient has been risk-assessed and selected for additional VTE prophylaxis treatment should be continued into the post-operative period to improve VTE protection. However, currently there is no direct evidence to indicate optimum duration for this prophylaxis. The impact of duration of VTE prophylaxis on VTE prevention in patients who present with symptomatic SVT has been reported by Cosmi in the Steflux study [29]. Patients presenting with symptomatic SVT were randomised to receive intermediate dose LMWH for 10 days or for 30 days, or low dose LMWH for 30/7.Steflux showed that 30 day treatment with LMWH (intermediate or low dose) was more effective than 10 day treatment with intermediate dose LMWH. In a recent non randomised retrospective study from ambulatory endovenous laser ablation practice Keo compared 3 days prophylaxis using fondaparinux or Rivaroxaban with10 days of Rivaroxaban with the clinician deciding on which strategy to use for each patient [30]. There were 3 DVTs in the group who had 3 day treatment and none in those who were treated for 10 days.
However this difference disappeared when the authors applied Propensity Score Matching to their data.
The limitations inherent in this study are that this is a retrospective case series review from a single consultant's practice in a single UK NHS trust. We are reporting findings from our scoring system that will require independent validation. However, despite these limitations we feel that the contents of this paper will add to debate in this area which has been limited by lack of relevant publications. Lack of debate has led to this important subject receiving scant attention in the venous literature, and the continuation of poor practice.
Endovenous thermal procedures may be complicated by serious VTE events including death. The current state of pharmacological thromboprophylaxis practice remains patchy and subjective. A logical way to mitigate VTE risk in these ambulatory patients, undergoing apparently low risk intervention, is for clinicians to employ a selective VTE prevention strategy. This involves risk-assessing all patient's for VTE and managing those at increased risk, who have no bleeding risk, with additional anticoagulant prophylaxis. When giving prophylaxis, treatment should be extended into the post-procedure period to improve its effectiveness.
None.