Fundal abnormally invasive placentae (AIP) rate is not precisely known, though, it is thought to be infrequent. Acute abdomen due to uterine rupture is an atypical and an extremely rare presentation. Hereby, we report the case of a 33-year-old G3P2002 who presented at 21-weeks with acute abdomen. CT-Scan and color-Doppler ultrasound showed massive hemoperitoneum with a fundal placenta actively bleeding into the abdominal cavity. At laparotomy, the uterus had a 3 cm dent in its left fundal area through which villi were protruding and actively bleeding. Uterine rupture due to non-previa AIP should be considered in the differential diagnosis of pregnant patients presenting to ED with acute abdomen. Current strategies of referring only patients with placenta previa or placentas covering previous cesarean scars for screening by expert sonographers will not enable prenatal identification of this uncommon yet dangerous AIP.
Abnormally invasive placentation, Acute abdomen, CT-scan, Massive hemoperitoneum, Non-previa placenta
Abnormally invasive placenta (AIP) refers to abnormal invasion of placental villi into the myometrium due to deficient decidua basalis [1]. General practice consist of screening this condition in high-risk patients who have low-lying placenta (previa) covering a previous cesarean scar, and confirm it later in the third trimester by ultrasound or MRI [2-4]. Nevertheless, placentae located in the uterine fundus can be an AIP. Unfortunately, most of these cases are not diagnosed prenatally and are encountered in the postpartum period as retained placentae and hemorrhage at attempts of manual removal or infrequently might present in the antenatal period as acute abdomen due to uterine rupture and hemorrhagic shock [5]. This is a serious and challenging condition which requires proper instant diagnosis and prompt management. Hereby, we report a case of fundal AIP who presented with acute abdomen at 21 weeks' gestation and describe the findings of Computed Tomography scan (CT-scan) and ultrasonography. A brief review of recent literature was also done to underscore the importance of prenatal diagnosis.
A 33-year-old woman, G3P2002, presented to the emergency department (ED) at 21 weeks of gestation complaining of acute diffuse abdominal pain of 1 day duration. She had a history of 2 previous uncomplicated low segment transverse cesarean delivery (CD). During this pregnancy, she was regularly followed at a private clinic with reportedly smooth antenatal course, normal fetal morphology scan and a placenta located high at the fundus of uterus. Clinical examination revealed an apprehensive but pale patient with diffuse abdominal tenderness, rebound tenderness, guarding, and generalized dullness. Vital signs showed tachycardia of 120 beats per minute, tachypnea of 20 breaths per minute, a blood pressure of 100/60 mmHg, and a temperature of 36.7 ℃. Intravenous fluid therapy was started. Laboratory tests showed a hemoglobin of 7.3 g/dl, marked leukocytosis of 27,000 cells/mm3, creatinine of 1.3 mg/dl, and normal liver function tests.
A Computed Tomography scan (CT-scan) was done by the ED team to rule out common and serious causes of acute abdomen. It showed a moderate amount of free fluid in the abdomen, a 2 × 2 cm exophytic vascular mass bulging through the left fundal area where the placenta was located with indentation of the adjacent myometrium suggestive of placenta percreta (Figure 1). Following these findings, the obstetrical team was urgently consulted. A rapid assessment with a bed-side ultrasound showed an intrauterine fetal death and a fundal placenta with adjacent myometrial thinning. Using color-flow Doppler, an eccentric spurting vessel at the outer border of the uterus was seen jetting blood into the peritoneal cavity. A vaginal exam showed a fully dilated cervix. A decision to perform an urgent laparotomy to control the bleeding was made. Unexpectedly, the patient vaginally delivered a dead macerated male fetus weighing 575 grams on the operative room table. At laparotomy, about 4 liters of fresh blood and clots were evacuated. Exploration of the abdomen showed a 3 × 2 cm of the placenta bulging through a dent in the left parasagittal anterior surface of the uterine fundus with active bleeding. Hysterectomy was performed to secure hemostasis. Intraoperatively, the patient received a total of 8 units of packed red cells and 4 units of fresh frozen plasma. She was transferred to the intensive care unit for close observation. Finally, she was discharged home on the third postoperative day in a stable condition. Histopathologic examination confirmed the diagnosis of placenta percreta.
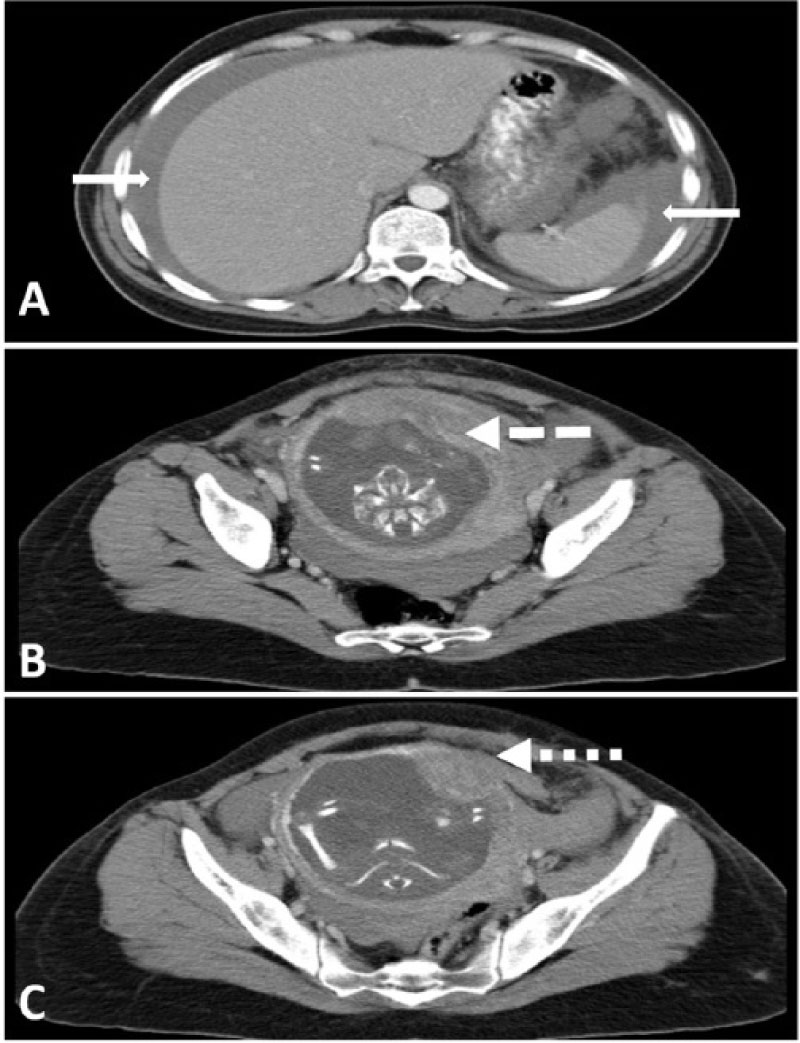 Figure 1: CT-scan of the abdomen and pelvis showing signs of uterine rupture due to fundal placenta percreta; A) Hemoperitoneum around the liver and spleen (solid white arrows); B) Fundal insertion of the placenta (dashed white arrow); C) Placental invasion of the myometrium at the left fundus level (dotted white arrow).
View Figure 1
Figure 1: CT-scan of the abdomen and pelvis showing signs of uterine rupture due to fundal placenta percreta; A) Hemoperitoneum around the liver and spleen (solid white arrows); B) Fundal insertion of the placenta (dashed white arrow); C) Placental invasion of the myometrium at the left fundus level (dotted white arrow).
View Figure 1
Placenta previa and CD are the strongest risk factors for previa-AIP. The incidence of previa-AIP increases exponentially with increasing number of CD. It can reach up to 67% in women with previous 4 CD or more compared to 3% in women with no previous CD [2]. Similar trend has been reported in women with non-previa AIP. Women with more than 6 previous CD had an incidence of 4.7% of non-previa accreta compared to 0.03% in women with no previous CD [2,6,7]. In our case, the absence of placenta previa decreased the suspicion of AIP despite the presence of two previous cesarean deliveries. Findings on CT scan have pointed directly to the etiology and allowed a timely management. In fact, cases with non-previa AIP are rarely diagnosed prenatally and the vast majority will have either a postpartum retained placenta or rarely might develop focal uterine perforation, as in our case, or even uterine rupture with possible hemorrhagic catastrophes.
Little is known about the exact incidence, risk factors, best diagnostic imaging modality or the optimal management of non-previa AIP. Even when these cases were highly suspected, no clear guidelines exist concerning the best modality of prenatal management or timing and route of delivery [3,8,9]. A search in Medline database was done using the following terms: ["fund*" AND ("abnormal placenta*" OR placenta percreta" OR "placenta accrete" OR "placenta increta")]. The search was limited to articles published in English. The reference list of each relevant article was also searched. In total, we found 113 cases with similar clinical presentation to the present case.
CT-scan was used to orient management in only 8 cases (Table 1) [10-15]. This imaging modality is not usually used during pregnancy except in emergency situations at ED. It is considered the modality of choice owing to its availability, effectiveness and the ease of use without lengthy preparation. It is the gold-standard imaging tool used in EDs worldwide [16]. Although, during pregnancy, some obstetricians have restrictions related to radiation exposure, CT-scan can be used especially when benefits outweigh risks to evaluate non-obstetric causes of acute abdomen with excellent accuracy [17]. In 3 out of 8 cases, CT-scan identified the site of rupture as in our case, however, in the 5 remaining cases, there were indirect signs such as floating fetus in the cavity, hemoperitoneum and high attenuation collection near the uterus.
Table 1: Characteristics and CT-Scan findings of the 9 cases of fundal placenta percreta complicated by uterine rupture. View Table 1
The presence of placenta previa in patients with previous cesarean deliveries raises the suspicion of AIP and these cases are referred to specialized centers for assessment of abnormal placentation. Whereas, in non-previa (fundal-located placentae), AIP is usually not suspected and hence such patients might experience serious adverse outcome.
In patients with previous uterine surgical intervention (including cesarean delivery), meticulous assessment of placentae, irrespective of their location, should be performed searching for abnormal sonographic features or vascular patterns that are usually associated with AIP [18].
In conclusion, AIP rate will continue to escalate in parallel with the ever-increasing rate of CD. More awareness, enhanced imaging accuracy and better surgical experience with handling of previa-associated AIP have resulted in curbing hemorrhagic complication rates. No large series or studies exist to date to guide on the diagnosis and the optimal management of non-previa AIP both in the antenatal or peripartum periods. Acknowledgement of increased risk for non-previa. AIP in association with any uterine surgical intervention or anomaly, searching for the common sonographic features and abnormal hypervascularity pattern during first or second trimester and judicious intervention appropriate with the family planning of the patient might be of value in ameliorating the dismal outcome of these serious cases.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
The Authors declare that there is no conflict of interest.