Objective: The aim of the study was to assess utilization of labor analgesia and associated factors among obstetric caregivers working at public hospitals of Sidama region.
Result: Among 346 respondents 143 (41.3%) 95%CI (36.1-46.2) were utilize labor analgesic, out of them 82(23.7%) were provide non-pharmacological labor analgesia, 60 (17.3%) were provide both pharmacological & non-pharmacological methods. Statically significant factors for utilization of labor analgesia were adequate knowledge [AOR =2.42, 95% CI (1.4-4.5)], higher qualification [AOR=3.9, 95%, CI (1.8-8.5)], availability of drugs [AOR=3.8, 95%CI (1.5-9.9)] and training on labor analgesia [AOR=3.3, 95%CI (1.8-6)]. The overall practice of labor analgesia was low. Adequate knowledge, high qualification, availability of drugs, and training on labor pain managements were factors significantly associated with the current utilization of labor analgesia in the study area.
Utilization, Obstetric caregivers, Analgesia
AOR: Adjusted Odds Ratio; CI: Confidence Interval; NSAID: Non Steroidal Anti-Inflammatory Drugs; OGS: Obstetric Care Givers; OR: Odds Ratio; SHBD: Show How Bear Down; SWI: Subcutaneous Water Injection; TENS: Transcutaneous Electrical Nerve Stimulation; SPSS: Statically Package for Social Science; WHO: World Health Organization
Pain is a subjective sensory and emotional experience to protect the body from harmful stimuli and it is a common signal of diseases. It is always an unpleasant sensation that caused by either irritation of receptor or nerve damage [1]. Labor pain is as old as human being having complex physiological factors such as uterine contraction, cervical dilation, and effacement and psychological factors such as stress, anxiety, and fear. It is considered that worst type of pain in which most women accompany during their life, despite this its memory disappear with time [1]. It may be visceral which occur in early first stage of labor (contraction of uterus and cervical dilation) and somatic which occur in late first stage of labor and second stage of labor (pressure from fetal presenting part may compress perennial nerves) [2]. Severe pain during labor may result in the stimulation of the sympathetic nervous system leading to increasing maternal blood pressure and increase oxygen consumption affecting utero placental blood flow and finally it causes fetal breathing problem [3]. Labor pain is worst acute pain, in which most women's experience in their lifetime and most laboring mothers need labor analgesia [4]. Pain during labor has a great role on maternal preference on mode of delivery, relieving labor pain decrease laboring mothers decision for CS by 50% [5]. Culturally as laboring mothers get family support during labor at home delivery, poor quality of care including absence of labor analgesia in the health facility is one factor which decreases institutional delivery [3,6,7]. Many pharmacological labor analgesics like non-opioids (diclofenac), opioids, inhaled agents, and epidural agents and non-pharmacological methods like hypnosis, Subcutaneous Water Injection ambulation, Relaxation techniques and massage were developed [8].
Non-pharmacological methods are safe for the mother and the baby over pharmacological methods but their effectiveness is unclear as the study declare (Jones, et al. [8]), Similarly the study conducted in Lublin concluded that most laboring, mothers prefer non-pharmacological pain relief methods and antenatal counseling plays a great role for their preference (Pilewska-Kozak, Klaudia et al. 2017). Administration of labor analgesia in early stage of labor decrease negative impact on the mode of delivery and it improve maternal satisfaction (Landau 2009).
Continuous psychological support for laboring mother improves maternal satisfaction with the service, feto- maternal birth outcome and to decrease negative feeling on birth experience [9]. Labor analgesia decreases episiotomy rate, postpartum blood transfusion and improves neonatal birth outcome and maternal satisfaction [10]. Furthermore it can decrease postpartum depression, anxiety, postpartum fever and post-traumatic stress disorder, However, most of these pain effects are alleviated by effective labor analgesia that may benefit the mother and fetus [11]. Managing labor pain and minimizing the suffering of laboring mother is the main concern of health care provider and client but the practice to relief the pain varies across different countries. In Bangladesh health care providers perceive labor pain is a natural process and recommending labor analgesia is unnecessary but they rely on providing continuous labor support [12]. In India 55% of respondents were provide epidural labor analgesia [13]. Utilization of labor analgesia in different countries of Africa showed 48.4% in Zara Nigeria [14], 49% in Nigeria [15], 44.9% in Egypt [1] and 3.3% in Kenya [16]. In Ethiopia 77% of obstetric care givers agree with the need of labor analgesia [17], but only 54.4% in Addis Ababa [18], 43.3% in Tigri region [19], 40.1% in Amhara region [20] and 37.9% in Kembata Tembaro zone [21] of obstetric care givers were utilize labor analgesia. Different studies identified many factors that affect practice labor analgesia. Negative attitude towards labor analgesia, lack of skill, inadequate knowledge, high patient flow, unavailability of drugs in health facility were factors which affect practice of labor analgesia in tigri region [19]. Another studies conducted in Ethiopia conclude that having Adequate knowledge is one factor which affect practice of labor analgesia [20,22]. The result of this study may help policy makers, stakeholders, and obstetric caregivers to design appropriate intervention in giving safe and comfortable delivery service as well as baseline for further research.
Institutional based cross sectional study was conducted in sidama region public hospitals. Sidama region is the tenth regional state, found in southern part of Ethiopia. Its capital city is Hawassa, which found 275 km from Addis Ababa. The administrative region bounded by Oromia in North, East, and South East, with the Gedeo Zone in the South and Wolayta Zone in the West. The total population lives in Sidama region was 4,369,214. Out of this, 2,201,313 are females. There are 424 obstetric caregivers work in labor ward of public hospitals in Sidama region.
Simple random sampling technique was used to select fourteen public hospitals from eighteen public hospitals and all obstetric caregivers who were work in labor ward of selected hospital were included in the study. The sample size for dependent variable was calculated using single population proportion formula taking prevalence of labor analgesia practice (p) 0.37 from the study conducted in Kembata Tembaro zone (Geltore, et al. [22]). By considering 5% margin of error (d) which gives n = 358.The sample size for factors were calculated using EPI version 7 but the sample size for factors were less than from the sample size for calculated for dependent variable. By adding 5%, non-response rate the final sample size was 376.
Source population were all obstetric caregivers (doctors, health officers IESO, midwives, nurses) working in labor ward of public hospitals. All obstetric caregivers who were work in labor wards of selected public hospitals were study populations.
The data collectors collected data using structured and pre- tested self-administered questioner that was prepared by reviewing different literatures considering the local situations of the study area and purposes of the study. It was developed in English language to be understood by every respondent. Five BSc midwives were requite for data collection and two BSC midwives supervised it. Training was provided for all data collectors and supervisors on the overall steps and procedures of data collection and proper data handling. Pretest was conducted in 5% (19) of study population by administering questioner at Shashemena referral hospital.
Data was entered in computer using Epi-data version 3.1 and exported to SPSS version 22 for recoding and, analysis. Descriptive statistics such as frequency, mean, standard deviation, and percentages were calculated. The result was present with text, table, graph, and figure. Finally, the results were in expressed terms of Adjusted Odds Ratio (AOR) and 95% confidence interval (CI). Finally, variables with p-value less to 0.05 on multivariable analysis were considered as statically significant.
Three hundred forty six (346) skilled obstetric caregivers were included in the study making a response rate of 92%. The mean age of the respondents was 28.46 with standard deviation of (SD = 4.653) years, out of them 245 (70.8%) were in age group of (25-34). Among of the respondents 208 (60.1%) were females. Among the respondents 163 (47.1%) were protestant and 245 (70.8) were midwives. Out of the respondents 213 (61.6%) were BSC and 244 (70.5%) had less than or equal to five (5) years clinical experience at obstetrical care (Table 1).
Table 1: Socio demographic characteristics of skilled obstetric care givers working at labor wards in Sidama Region selected public hospitals, Southern Ethiopia, 2020 (n = 346). View Table 1
Among the total respondents 143 (41.3%) 95%CI (36.1-46.2) were utilize labor analgesia, out of them 82 (23.7%) were utilize non-pharmacological analgesic methods, 60 (17.3%) were utilize both pharmacological and non-pharmacological methods. From the respondents who were utilize labor analgesia, 71 (49.7%) were used routinely, 57 (39.9%) and 15 (10.5%) were used sometimes and as patient request. Diclofenac was widely used pharmacological labor analgesics by 79 (22.8%) of respondents followed by systemic opioids (pethidine) 53(15.3%). Out of the total respondents 56 (16.2%) were used pharmacological labor analgesia methods during instrumental delivery and 55 (15.9%) were to rule out false labor. From non-pharmacological labor analgesic methods SHBD were widely used by 127 (36.5%) followed by psychotherapy 121 (35%) (Figure 1).
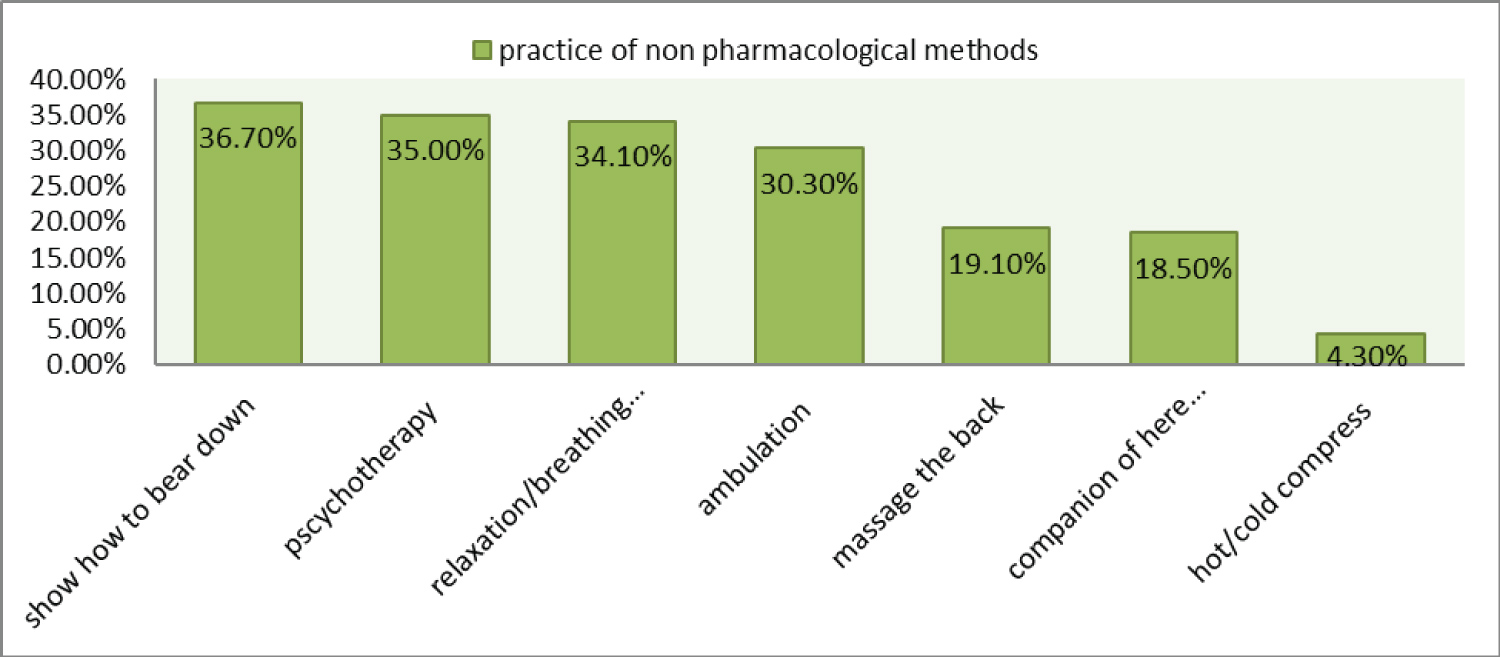 Figure 1: Utilizations of non-pharmacological labor analgesia methods among skilled obstetric care givers in sidama Region selected public hospitals, Southern Ethiopia, 2020 (n = 346).
View Figure 1
Figure 1: Utilizations of non-pharmacological labor analgesia methods among skilled obstetric care givers in sidama Region selected public hospitals, Southern Ethiopia, 2020 (n = 346).
View Figure 1
On bivariable analysis sex, profession, level of education, pain expectation, availability of drug in the hospital, training on labor pain management, knowledge, and attitude were significantly associated with the current utilization of labor analgesia. On multivariable analysis only high qualification, [AOR = 3.9, 95% CI (1.8-8.5)], adequate knowledge [AOR = 2.42, 95% CI (1.4-4.3)], training on labor pain management [AOR = 3.3, 95% CI 1.8-6)] and availability of drugs in hospitals [AOR = 3.8, 95% CI (1.5-9.9)] were significantly associated with current utilization of labor analgesia (Table 2).
Table 2: Bivariable and Multivariable analysis of factors associated with utilizations of labor analgesia Sidama Region selected public hospitals, Southern Ethiopia, 2020 (n = 346). View Table 2
The current over all utilization of labor analgesia at Sidama region public hospitals was 41.3%, 95%CI (36.1-46.2). The finding of the study was in line with studies in Egypt 44.9% [1], Tigri region, Ethiopia 43.3% [19], Amhara Region Ethiopia 40.1% [20] and in Kembata Tembaro zone 37.9% [22]. The finding was less than studies from India which were 55% of respondents used epidural analgesia [13], Zaria Nigeria 48.4% of respondents were utilize labor analgesia [14], in Nigeria 49% of respondents offered labor analgesia which is commonly opioid (41.1%) [15] and in Addis Ababa 54.2% [18]. The difference may be due to difference in socio demographic characteristics of respondents. In addition to this, more than half of the respondents in this study had inadequate knowledge about labor analgesia.
The finding of the study was higher in this study compared to the studies conducted in Ibadan, Nigeria where (34.5%) of respondents' commonly used back massage and psychotherapy [23], in Nigeria 25.9% of obstetricians offered epidural analgesia in [24], in Kenyatta national hospitals 3.3% of respondents used epidural analgesia [16] and in Hawassa city administration 13.8% of respondents were utilized labor analgesia [25]. This difference may be due to attitudinal difference of health care providers from place to place. The other explanation might be the effect availability of analgesic drugs in hospitals. Difference from the study conducted in Hawassa city administration may be in this study, skilled obstetric caregivers who were provide labor analgesia routinely, sometimes, and as maternal request were considered as they were utilize labor analgesia. But, in the study conducted in Hawassa city administration skilled obstetric care givers who were utilize labor analgesia routinely were considered as they were utilize labor analgesia. The odds of labor analgesia utilization among OCGs who had adequate knowledge were 2.4 times higher than the odds of labor analgesia utilization among OCGs who had inadequate knowledge. This finding is consistent with the studies conducted in Durame hospital, southern Ethiopia [21], East Gojam [26] Ibadan Nigeria [23] and in Kenya [27]. But the finding was in contrast to the study conducted in Amhara Region referral hospitals [20] and Kembata Tembaro zone public hospitals [22], which concluded that the odds of labor analgesia utilization among OCGs who had inadequate knowledge were higher than the odds of labor analgesia utilization among OCGs who had adequate knowledge. This difference may be in this study skilled OCGs who had BSc and above level of education were more likely to utilize labor analgesia, professionals who had BSc and above level of education were more likely to have adequate knowledge, they utilize what were they knew. The odds of labor analgesia utilization among skilled OCGs who had high qualification were 3.9 times higher than the odds of labor analgesia utilization among skilled OCGs who had low qualification. This finding of the study is consistent with the study conducted in Tigri region [19]. But, it was in contrast to the study conducted in Amhara region which concluded professionals who had low level of education were more likely to utilize labor analgesia compared to professionals who had high level of education [20]. This difference may be in this study both pharmacological and non-pharmacological methods were utilized but in study conducted in Amhara region only non-pharmacological methods were utilized this may be due to non-pharmacological method are more familiar and utilized by OCGs having low level of education. The other may be OCGs who had high qualification were more likely to have adequate knowledge and skill to utilize labor analgesia compared to low qualification. The odds of labor analgesia utilization among skilled OCGs who were in hospital setting having accessible analgesic drugs were 3.8 times higher than the odds of labor analgesia utilization among skilled OCGs who were in hospital setting accessible have not analgesic drugs. The finding was consistent with the study conducted in kembata tembaro zone, south Ethiopia [22]. The odds of labor analgesia utilization among OCGs who gate any training on labor pain management were 3.3 times higher than the odds of labor analgesia utilization among OCGs who did not gate training on labor pain management; this is because training enhances both knowledge and skill of skilled obstetric caregivers to utilize labor analgesia.
The overall utilization of labor analgesia in this study was low. The major predictors for practicing labor analgesia in this study were adequate knowledge, high qualification, availability of drugs in hospitals and training on labor pain management. We recommend that health organizations and other stakeholders could provide training with task-oriented refreshment course on labor analgesia and to provide required drugs, which will help skilled obstetric caregivers to fulfill the gap of their knowledge on labor analgesia and utilization of labor analgesia, which can be achieved through teamwork by all the stakeholders in the health sectors. Needs to ensure opportunities for educational chance of skilled obstetric care givers especially for those who had low level of education and qualitative study needs to be done on reasons of non-practicing labor analgesia and maternal satisfaction on labor analgesia provision.
Because of limited resource and time, study was conducted using self-administered questioners to assess utilization, which was best to be complemented by observational check list. This study might have been subjected to recall and response bias.
The ethical approval and consent were performed in accordance with the declaration of Helsinki. Ethical clearance and approval was obtained from the Institutional Review Board of Hawassa University College of Medicine and Health Sciences with Registration number IRB/203/2012). Ethical clearance paper was presented to sidama region health office and formal letter of cooperation was written to the respective hospital from the health office to undertake research activities in hospitals. The letter was given for administrative leader of each hospital to gate official permission. After explaining the purpose and aim of the research written informed consent was obtained from each volunteer participants. The participants were informed about the right to refuse to participate in the study or to withdraw consent to participate at any time without reprisal. Every precautions were taken to secure the privacy and keep confidentiality of study participants.
Not applicable.
The datasets used or analyzed during the current study available from the corresponding author on reasonable request.
There is no conflict of interest in between the authors.
YA select the title, develop proposal, prepare the tool, conduct the research, analysis data write the final document and prepare the manuscript. AK, MS, AA, BA and BT give comment on title selection, proposal writing, questioner preparation and throughout all the research process BA supports on manuscript preparation.
No funding.
We would like to forward our gratitude to Hawassa University College of medicine and health science, department of midwifery. Our special thanks go to the supervisors, data collectors, and the respondents and regional health bureau.