Sierra Leone is a country with an extremely high maternal mortality ratio (MMR) with over 1000 maternal deaths per 100,000 live births. We analyzed data from the national maternal death surveillance and response system to describe the trend and determine the burden of maternal deaths in Sierra Leone.
We conducted secondary data analysis of maternal deaths in Sierra Leone from 2017 to 2020. Data were obtained from the District Health Information System 2 (DHIS 2) database and the National MDSR line list. Data were analyzed using SPSS Version 20 to determine proportions and associations.
We reported 2255 maternal deaths between 2017 and 2020. The MMR decline from (187/100,000 live births) in 2017 to (169/100,000 live births) in 2020. Women aged 20-34 years accounted for 66% (1,492) of those who died. Maternal deaths after delivery accounted for 63% (1421), and 81% (1157) of them died within the first 7 days of delivery. Health facility deaths accounted for (1,733; 77%). Among women admitted, 45% (790/1733) died within 24 hours and 11% (188/1733) died less than 1 hour. Of the 1,948 deaths, 55% (1083/1948) occurred during the day. Direct and indirect obstetric causes accounted for 78% (1765) and 17% (385) of deaths, respectively. Postpartum hemorrhage and anemia accounted for (37%; 660/1765) and (15%; 58/385) of maternal deaths, respectively.
Though the MMR is still high, we observed a decline in the trend. Main cause of death were age group 20-34 years, anemic pregnant women and postpartum hemorrhage. We recommend health authorities to provide health education for pregnant women and prompt referral system for severe cases.
Maternal mortality rate, Maternal death, Trend, Sierra Leone
According to current estimates, about 810 women die from complications of childbirth every day [1]. The risk of death from pregnancy complications impacts women in every country across the globe to varied degrees. A pregnant woman from a developing nation is 36 times more likely than a pregnant woman from a developed country to experience pregnancy-related problems [2].
Globally, an estimated 295,000 maternal deaths were reported in 2017. Approximately 66% of these deaths occurred in Sub-Saharan Africa. Furthermore, the maternal mortality ratio (MMR) in Sub-Saharan Africa (542 maternal deaths per 100,000 live births) was more than two times higher than the global average [1]. MMR, which is expressed as the number of maternal deaths per 100,000 live births, is a critical performance indicator that is globally-recognized for the international comparisons of maternal health.
Sierra Leone has made progress in reducing maternal mortality, with the MMR dropping from 2,480 maternal deaths per 100,000 live births in 2000 to 1,120 per 100,000 live births in 2017, with an overall reduction of 55% between 2000 and 2017 [3]. Despite these gains, Sierra Leone was still estimated as one of the three countries with an extremely high MMR in 2019, recording the highest MMR (717 maternal deaths per 100,000 live births) in West Africa [4]. Moreover, the Sierra Leone Demographic and Health Survey conducted in 2013 reported that a woman in Sierra Leone faces a 1 in 7 (about 14%) lifetime risk of dying from pregnancy or childbirth. The same survey reported that maternal deaths account for 36% of all deaths among women aged 15-49 with a MMR of 1165 maternal deaths per 100 000 live births [5]. To address this problem, the country in collaboration with partners established the Maternal Death Surveillance and Response (MDSR) system in 2015 to accurately document and reduces the high maternal mortality.
The aim of the MDSR system is to provide information that can be used to determine the true magnitude and causes of maternal deaths and provide timely response mechanisms [6]. This involves identifying, reporting, investigating, and reviewing every maternal death, and analyzing the data at both national and district levels. Furthermore, the WHO urged countries to keep newborn and maternal monitoring efforts to reduce both child and maternal deaths [7]. Also, WHO in 2015 released the strategies for ending preventable maternal mortality (SPMM), urging all member countries to reduce preventable maternal deaths [8]. The only way to achieve this is by counting every maternal death and using the information from dead to protect the living.
Even though national maternal deaths data are being analyzed annually, there is no published report on maternal deaths, particularly, a nationally aggregated data analyzed for multiple years since the inception of the MDSR system. We therefore analyzed the MDSR national data from 2017 to 2020, to describe the trend, and determine the causes of maternal deaths in Sierra Leone.
We conducted a descriptive study using secondary MDSR data in Sierra Leone from January 2017 to December 2020.
Sierra Leone is located in the West Coast of Africa with an estimated area of 71,740 km2, and is bordered by Guinea to the northeast and Liberia to the southeast. It has a projected population of 8,100,318 as at 2020 with 1,798,271 being women of childbearing age [9]. The country has five administrative regions with 16 districts [10]. The health infrastructure is tiered into tertiary hospitals, secondary (district) hospitals and peripheral health units (PHUs). The PHUs provide primary health care services and include Community Health Centers (CHCs), Community Health Posts (CHPs) and Maternal and Child Health Posts (MCHPs) [11].
Data source: Maternal deaths in Sierra Leone are captured through the parallel surveillance systems of the MDSR system and the National Disease Surveillance Programme (NDSP) of the Ministry of Health and Sanitation (MoHS). The data analyzed in this paper is based on maternal deaths captured by the MDSR system. The MDSR system was established in 2015 and was fully implemented in 2016, and has now expanded to cover the entire country. All maternal death cases reported at the national level from all the 16 districts during the study period, were included in the study.
We collated reported maternal death cases in the country from 2017-2020, which were entered into Excel database for program monitoring purpose. All reported cases of maternal deaths are suspected maternal deaths unless properly examined and evaluated to identify the causes and circumstances surrounding the deaths, and this includes methods designed for reviewing deaths that occur in both health-care facilities and communities. Medical causes and contributing factors were also determined. A suspected maternal death was defined as the death of a woman from any cause related to pregnancy or its management, or within 42 days of the termination of pregnancy, irrespective of the duration and the site of the pregnancy, but not from accidental or incidental causes. The maternal death review committee reviews the circumstances and confirm maternal deaths (i.e. whether the death was "related to or aggravated by the pregnancy and its management") [12].
Data in excel spreadsheet was cleaned and double-checked with data extracted from the DHIS2 for completeness and consistency, before analysis. We analyzed the demographic characteristics, obstetric characteristics, place of death (community, health facility or in transit), facility type were death occurred (Government hospital, CHC, CHP, MCHP, Private and Faith-based health facility), time (in hours) of death and cause of death. Causes of maternal death were classified into two broad categories (direct and indirect). Direct obstetric causes referred to as obstetric complications that occurred during pregnancy at or after delivery, including obstetric hemorrhage, eclampsia, abortion, ectopic pregnancy and puerperal infection. Indirect obstetric cause referred to a disease that existed before or developed during pregnancy, unrelated to obstetric causes, but was aggravated by the physiological effects of pregnancy.
Live births from 2017 to 2020 were obtained from the projected population (2016 to 2022) for the Expanded Programme for Immunization (EPI), MoHS [13].
We calculated the maternal mortality ratio as the number of maternal deaths per 100,000 live births for the period under review. Median and range were computed for continuous variables, whilst frequencies and proportions were computed for categorical variables. Data were presented in tables and charts.
Permission for the MDSR data analysis was obtained from the Directorate of Reproductive and Child Health of the Sierra Leone MoHS. All the data used in this study were captured from the National MDSR database and no further information were obtained from patients' relatives. Patient names were excluded during data analysis to ensure confidentiality.
A total of 2,255 maternal deaths were reported from January 2017 to December 2020. Table 1 summarizes the sociodemographic and obstetric characteristics of the maternal death cases for key variables. The median age at death was 27 years (range, 13-50 years), with most women, 66% (1,492) between 20-34 years-old at the time of death. The median parity was 2 (range, 0-13). Most maternal deaths, 42% (940) occurred in women who had normal spontaneous vaginal delivery. About 63% (1421) of the maternal deaths occurred after delivery, 81% (1157/1421) of which died within the first 7 days of delivery. Twelve percent (262) of women never attended an antenatal care clinic before delivery. Majority of the maternal deaths (1733; 77%) occurred in the health facility, with government hospitals (1281/1733; 74%) accounting for the larger proportion of facility deaths. Among women admitted, 45% (790/1733) died within 24 hours, and 11% (188/1733) died less than 1 hour of admission. Of the 1,948 deaths for which time of death (in hours) was recorded, 55% (1083/1948) occurred during the day between 6:01 am and 18:00 (Table 1).
Table 1: Sociodemographic and Obstetric characteristics of MDs, Sierra Leone, 2017-2020. View Table 1
Trends in maternal mortality ratio from 2017 to 2020 are presented in Figure 1. We identified an overall decline in the maternal mortality ratio between 2017 (187/100,000 live births) and 2020 (169/100,000 live births).
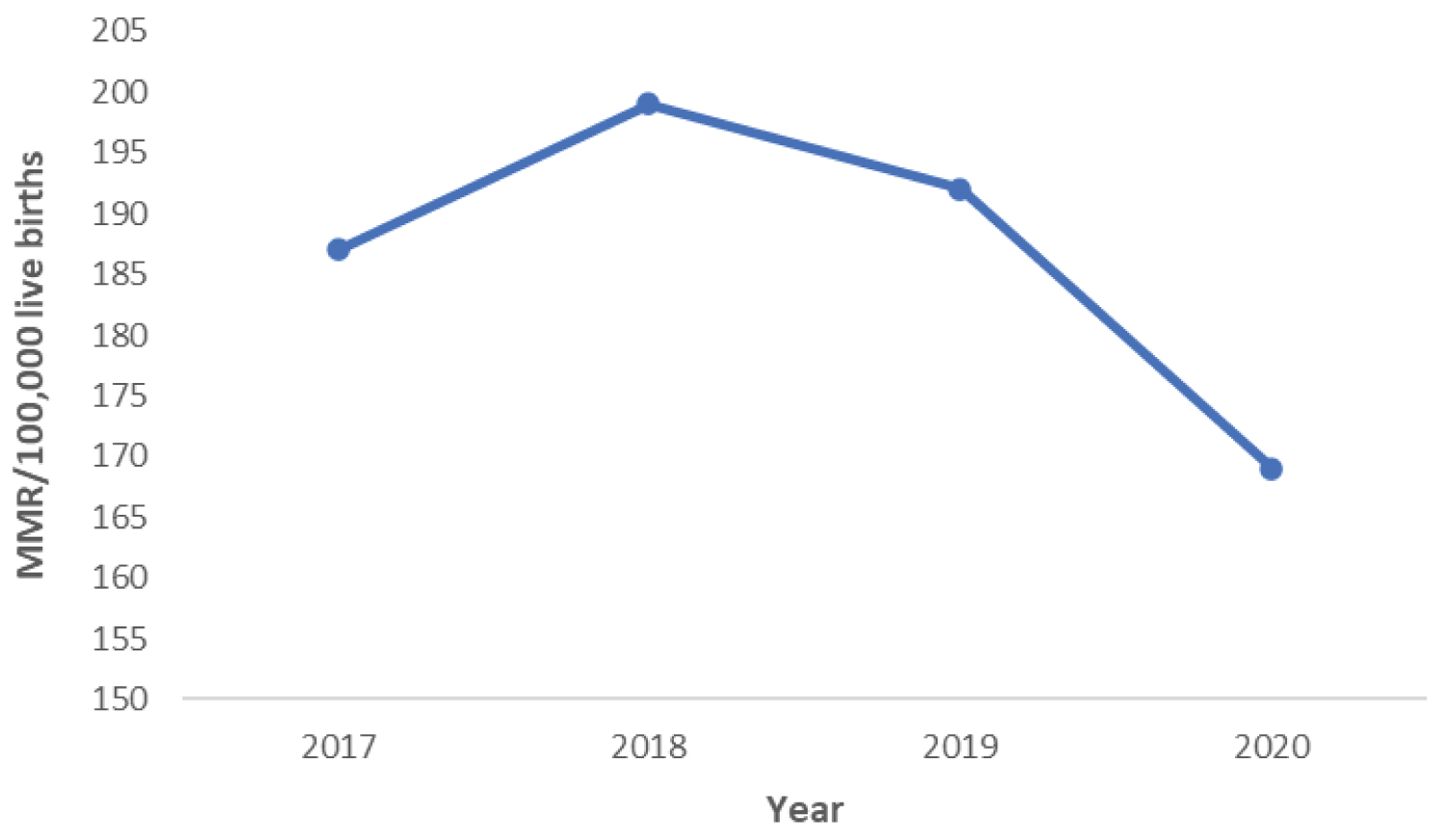 Figure 1: Yearly trends in maternal mortality ratio, Sierra Leone, Jan 2017 to Dec 2020.
View Figure 1
Figure 1: Yearly trends in maternal mortality ratio, Sierra Leone, Jan 2017 to Dec 2020.
View Figure 1
Overall, Kambia district recorded the highest MMR between 2017 and 2020 (252/100,000 live births), and Kailahun district had the lowest MMR (77/100,000 live births). In addition, there was a consistent reduction in the maternal mortality ratio for Kono (Figure 2).
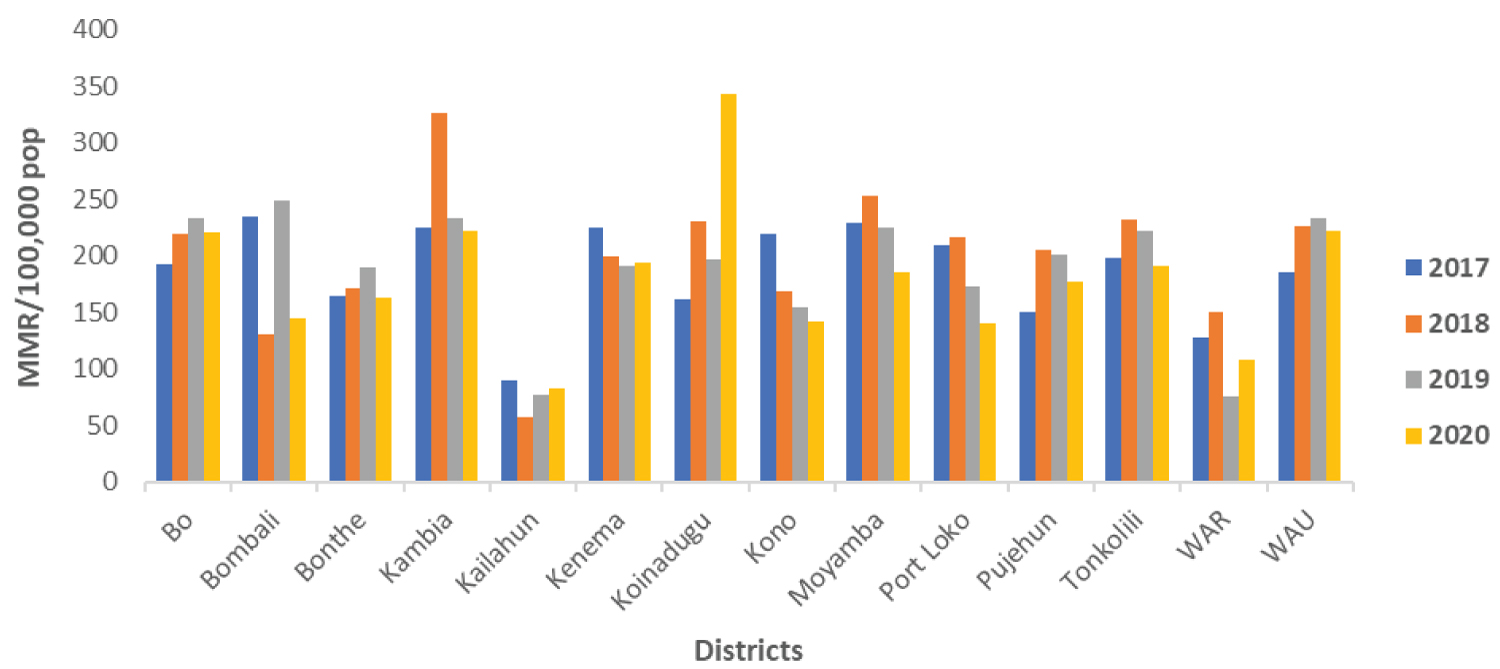 Figure 2: Trends in maternal mortality ratio by districts, Sierra Leone, Jan 2017-Dec 2020.
View Figure 2
Figure 2: Trends in maternal mortality ratio by districts, Sierra Leone, Jan 2017-Dec 2020.
View Figure 2
Of the total 2255 maternal deaths reported during the period under review, 2150 (95%) had evidence of cause of death of which 1765 (82%) deaths were due to direct obstetric causes and 385 (18%) were due to indirect obstetric causes. However, the cause of death for 105 (5%) of the total death reported was not documented. Postpartum hemorrhage (37%; 660/1765) and anemia (15%; 58/385) remained the leading causes of maternal deaths due to direct and indirect obstetric causes. Of the 1053 (47%) MDs for which contributory factors were recorded, delay in referral (33%; 346/1053) was the major health facility-related contributory factor, while the major patient contributory factor identified was delay in seeking health care (16%; 172/1053) (Figure 3).
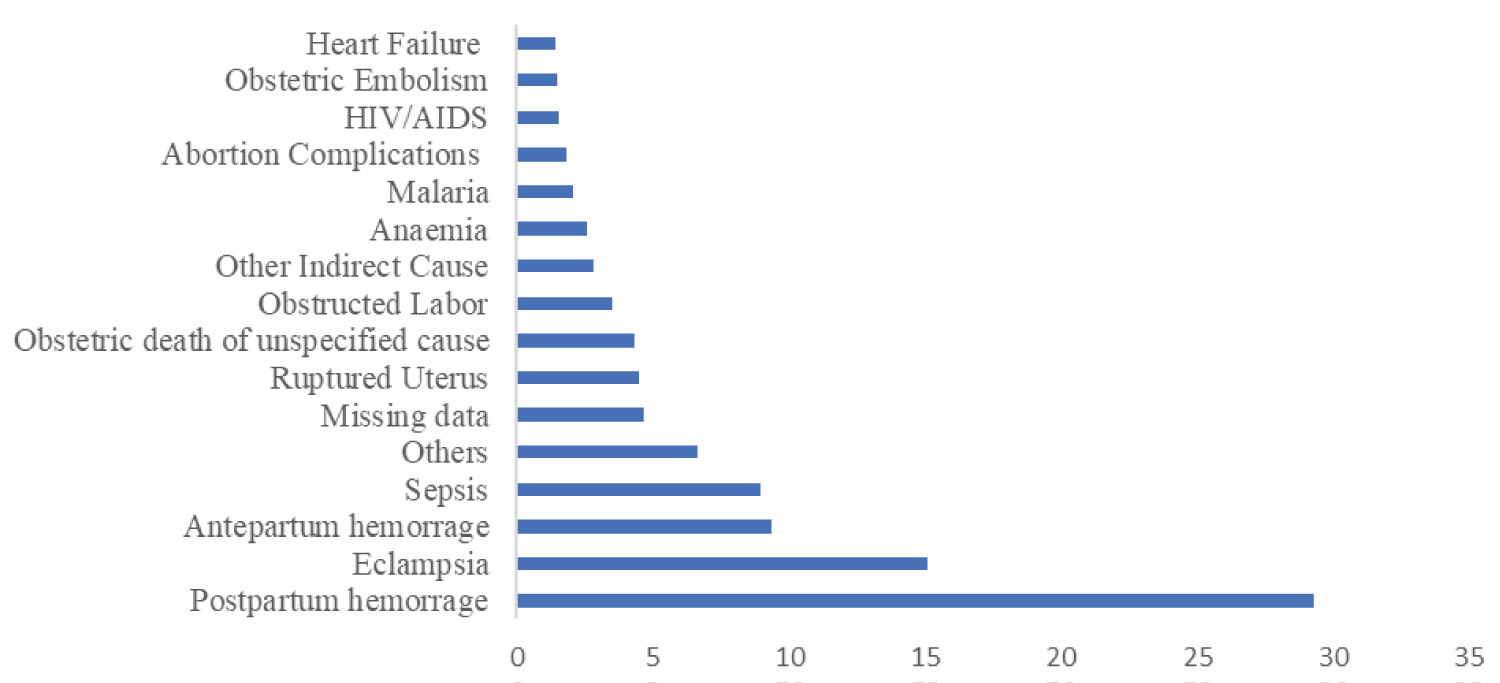 Figure 3: Causes of maternal deaths in Sierra Leone, Jan 2017-Dec 2020.
View Figure 3
Figure 3: Causes of maternal deaths in Sierra Leone, Jan 2017-Dec 2020.
View Figure 3
This study was conducted to assess maternal mortality in Sierra Leone between 2017 and 2020. Generally, there was apparent progress in reducing MMR in Sierra Leone compared to the DHS 2013 [5]. Beyond the Ebola outbreak, Sierra Leone has made great efforts in strengthening the health sector. The country initiated a free healthcare system in 2010 for pregnant women, lactating mothers, and children under the ages of five years. The Free Health Care Initiative (FHCI) resulted in more safe maternal deliveries in health facilities, and more women receiving antenatal care – thus contributing to reducing maternal deaths [14]. Despite this decrease in maternal deaths, the progress to reduce maternal mortality has been slow. Therefore, more efforts are required to meet the Sustainable Development Goals (SDGs).
Our study found that most women were between 20-34 years-old at the time of death. This finding was similar to the findings of a study conducted by Leonardo Antonio [15], but was in discordance with the findings of a study conducted on adolescent mothers (20-24 years) in 144 countries, where the mortality risk was lower among this group compared with mothers older than 30 years [16].
Furthermore, 14% of the maternal deaths were observed among teenagers (15-19 years). This shows that there are a large number of teenage pregnancies which may be attributed to none use of contraceptives, lack of knowledge, or lack of access to teenage-friendly health services.
Approximately, 78% of maternal deaths occurred in health facilities; tertiary facilities (hospitals) contributed the most, and this finding is similar to a study conducted in Mozambique, where the majority of the facility deaths (53%) occurred in tertiary hospitals [15]. In another study conducted in Tanzania over ten years, there was an increase in maternal deaths in public hospitals [17]. The high rate of maternal deaths in hospitals might be attributed to long travel distance from remote areas which resulted in poor outcomes. This can also be explained due to the fact that the worst cases are normally referred to tertiary healthcare facilities. This is evident as delay in seeking health care was the major patient contributory factor identified from our study including challenges with transportation. The current study shows community deaths were low as compared to facility-based deaths. This could be due to less sensitivity of the surveillance system where some community deaths are not detected and reported to the health system. This is consistent with findings from a study conducted in Mutare district, Zimbabwe [18]. So, more efforts are necessary to detect maternal deaths in the community which will prevent future deaths [6]. Our study clearly showed that most maternal deaths (55%, 95% CI: 45.2, 64.5, P-value = 0.317) occur during the day than at night. However, the difference is not statistically significant. Study conducted in Mexico reported that the maternal death was increased during the night shift, which was explained by understaffing particularly doctors and nurses [19].
The study also revealed substantial disparities in maternal deaths across districts. Kambia district in the North-west region of Sierra Leone had the highest MMR in the period of study. The high MMR might be attributed to the location of the district, which shares border with Guinea and has border communities with limited access to healthcare.
This study also revealed that direct obstetric deaths were still the major cause of maternal deaths in Sierra Leone. This result was in agreement with other study that reported that direct obstetric causes were the main causes of maternal death in the worldwide [20]. Another study conducted in Ethiopia reported a similar finding [21]. In addition, the major facility-related contributory factor identified in this study was delay in referral. A similar finding was observed in a study conducted in Ethiopia, where delaying in care in remote health facilities was one of a leading cause for maternal death [22].
In determining trends in the causes of maternal deaths, the proportion of direct obstetric deaths was increasing in all districts. This finding is consistent with a study conducted in the United State of America where obstetric/pregnancy-related deaths increased over time [23]. Postpartum hemorrhage remains the leading cause of direct obstetric deaths in our study which is consistent with other studies in Mozambique and Ethiopia [15,21]. Postpartum hemorrhage is a very serious condition, especially among pregnant women suffering from anemia and can lead to mothers' death after delivery. Pregnant women suffering from anemia should be diagnosed and receive treatment before delivery. Studies indicated that factors associated with postpartum hemorrhage caused maternal deaths in hospitals [24]. Furthermore, the majority of the maternal deaths occurred after delivery which might be attributed to poor postnatal care. The high number of women who died from postpartum hemorrhage might explain that hemorrhage is the leading cause of maternal deaths after delivery.
Indirect obstetric cause contributed to about 17% of the maternal death rate, and this includes anemia, Malaria, HIV and heart failure. The proportion of indirect causes in this study was higher than a study conducted in Nigeria, where anemia alone accounted for up to 32% of indirect obstetric maternal deaths, and where the indirect obstetric cause 1% [25]. This finding is also in discordance with a study conducted in Brazil which reported a low rate of indirect obstetric maternal deaths which was less than 10% [26]. The difference can be explained due to the fact that Sierra Leone's health system has been affected by natural and man-made disasters including the 2014 Ebola outbreak [27]. Reducing maternal deaths requires more efforts to prevent and manage maternal complications as most maternal deaths are preventable, if necessary, interventions are provided at the right time. A limitation of this study is that we used routinely collected data - in some variables were missing in the national MDSR system database. Some of these missing variables limited the depth and types of analyses we conducted.
Though the MMR is still high, we observed a decline in the trend of MMR in Sierra Leone. Kambia district, age group 20-34 years, pregnant women with anemia had the highest burden, with postpartum hemorrhage being the main cause death. We recommend the reproductive program in the MoHS to conduct a regular data quality assessment for the maternal deaths database to maintain completeness of the data. Also, the government should support the reproductive health program to take holistic action to reduce maternal deaths in Sierra Leone. Health authorities need to provide health education and promotion on the antenatal care issues for pregnant women. Prompt referral system for severe cases, and staff training in emergency obstetric care should be improved and maintained.
The authors declare no conflict of interest.
KNK, performed the research. KNK, GG, designed the research study. KNK, AHE drafted the paper and wrote the paper. GG, JSS, JSK, AHE, ZJB Review and edit the paper.