General information: Uterine fibroids are benign monoclonal neoplasms of the myometrium, representing the most common tumors in women worldwide. To date, no long-term or noninvasive treatment option exists for hormone-dependent uterine fibroids, due to the limited knowledge about the molecular mechanisms underlying the initiation and development of uterine fibroids. This paper comprehensively summarizes the recent research advances on uterine fibroids, focusing on risk factors, development origin, and pathogenetic mechanisms. Finally, future perspectives on uterine fibroids studies are summarized. Deeper mechanistic insights into tumor etiology and the complexity of uterine fibroids can contribute to the progress of newer targeted therapies.
Some studies reported the association between fibroids with uterine inflammation. By considering this hypothesis, the formation and recurrence of uterine fibroids can be prevented by diagnosis and treatment of inflammation, and complications and costs can be reduced. This study aimed to evaluate the association between chronic endometritis and uterine fibroids in non-menopausal women.
Aim: The purpose of this study is to investigate the clinicopathological features of patients with uterine myoma and to analyze and summarize factors affecting patient prognosis.
Methods: This study retrospectively investigated records of uterine myoma patients treated at JSC Central Clinical Hospital between January 2021 and November 2022. A total of 100 patients were included in this study, including the prognosis of the patient, MuClinical and pathological characteristics, including age, average body mass index (BMI), menopausal status, average lesion diameter, presence of hypertension or diabetes mellitus, operation method, myoma type, location, and quantity, number of fibroids, and presence of pelvic adhesion were analyzed via multivariate analysis.
Results: Among different contributing factors, the most common were: the erosion (43%), arterial hypertension (30.2%), anaemia (28.9%), Hepatitis (19.2%). The mean age was 47, with a maximum of 74 and a minimum of 23. Surgical intervention improved the quality of life of patients by 95%. This study showed that age equal to or greater than 60 was a risk factor affecting uterine myoma prognosis. This effect is potentially due to an age-related decline in physical and immune functions that results in a greater risk of endometrial hyperplasia caused by stimulation, as well as in greater physiological impact from surgical intervention.
Conclusion: This study analyzed the pathological characteristics of patients with uterine myoma, which may help improve the accuracy of disease diagnosis. Age, are risk factors affecting the prognosis of uterine mama, and can provide a reference for clinical treatment.
Fibroids, Uterine fibroids, Uterine myoma
Uterine myoma, also known as leiomyoma or fibroids, is the most common benign tumor of the female reproductive system. Uterine myoma patients generally show no initial obvious signs, but aging can bring abnormal uterine bleeding, pelvic compression symptoms, pain, and impacted fertility. Uterine myoma is the main underlying cause for clinical hysterectomy, which in turn has a significant adverse impact on women's reproductive health, social and medical resource consumption, and the health economy at large. At present, the specific pathogenic mechanism of uterine fibroids is not well known but is believed to be related to a variety of factors, including diet, age, hypertension, diabetes, anaemia, and chronic endometritis endometriosis. Uterine myoma is mostly treated with surgery [1], such as open uterine myoma enucleation, laparoscopic uterine myoma enucleation, open total hysterectomy, and laparoscopic total hysterectomy. However, these different surgical methods have different therapeutic effects and different prognoses [2,3]. As such, this study reviewed the clinicopathological features of uterine myoma patients and analyzed factors potentially impacting patient prognosis.
Uterine fibroid lesions were initially known as the “uterine stone.” In the second century AD, they were called scleromas. The term fibroid was first introduced in the 1860s. Uterine fibroids are the most common pelvic tumors among women of reproductive age, affecting more than 70% of women worldwide, particularly women of colour [1-3]. This disease has a profound impact on health care delivery and costs worldwide. Though most women with fibroids are asymptomatic, approximately 30% of them will present with severe symptoms which can include abnormal uterine bleeding, anaemia, pelvic pain and pressure, back pain, urinary frequency, constipation, or infertility. Uterine fibroids are heterogeneous in composition and size among women and within the same individual and vary in number between individuals. In addition, the fibroid pseudo capsule presents as a fibro-neurovascular structure surrounding a uterine fibroid, separating it from normal peripheral myometrium. Although benign, uterine fibroids are associated with significant morbidity; they are the primary indication for hysterectomy, and a major source of gynaecologic and reproductive dysfunction, ranging from menorrhagia and pelvic pain to infertility, recurrent miscarriage, and preterm labor. Uterine fibroids thus represent significant societal health and financial burden.
Other risk factors include older age, premenopausal state, nonparity, family history of uterine fibroids, hypertension, food additives, and frequent consumption of soybean milk. On the other hand, protective factors for uterine fibroids include combined oral contraception or injectable medroxyprogesterone acetate in the depot form, smoking in women of low mass, and parity [1]. Other important risk factors include obesity [4-6]. Individual and environmental risk factors associated with tobacco smoking and alcohol abuse can also contribute to the formation of uterine fibroids [7,8]. More risk factors are associated with a higher probability of uterine fibroid formation and development.
These points require some additional comments. Epidemiologists understand that they must study women from the community to eliminate bias and have a prospective study design with a large sample size and low loss to follow-up to enable the measurement of age-specific incidence and other risk factor-related pathogenesis of uterine fibroids [9]. Improvement of awareness and education for uterine fibroids in the community will help to better understand the risk factors of these diseases. Notably, data from uterine fibroid research in underrepresented groups are lacking [10]. On the other hand, epidemiological studies may reflect both the natural and false effects of a selected factor on the investigated outcome. Findings may be subject to different explanations because they may occur due to random errors, biases, or confounding, which may produce false results. These factors need to be considered at both the design and analysis stage of a study to minimize them. Notably, the same instruments for health outcomes evaluation in exposed and unexposed groups should be applied to avoid misclassification or bias. Studies without including confounding variables from the onset or without matching by age, race, and other factors should always be treated with caution [11].
Increasing age is a significant risk factor for uterine fibroids, especially among women at the premenopausal stage and those ≥ 40 years of age. For instance, 60% of African American women aged 35-49 years reported uterine fibroids, whereas 80% of those aged ≥ 50 have uterine fibroids. Among White women, 40% of those aged ≤ 35 years and 70% aged ≥ 50 years developed uterine fibroids [3]. These tumors have not been detected in prepubertal girls, and only sporadic cases have been reported in adolescents. However, the factor(s) involved in their development at such an early age is unknown. Due to the slight difference in biochemical pathways, uterine fibroids in young women do not exhibit typical uterine fibroid biology. In several cases, adolescent patients had a translocation between chromosomes 12 and 14, which is a confirmed risk factor for uterine fibroids [12,13]. Women at the menopausal stage have shrunk uterine fibroid lesions and decreased sex hormones. Notably, the use of hormonal replacement therapy may cause these lesions to regrow and may induce the first clinical symptoms of uterine fibroids [14].
Obesity is directly related to increased energy consumption and reduced physical activity [15]. Currently, obesity is the fifth leading cause of death [16]. Several studies have found obesity as a significant risk factor for uterine fibroids development, which has been attributed to the metabolic functions of adipose tissues. Adipose tissues produce and release various cytokines and growth factors involved in regulating diverse physiological and pathological processes, including immunity and inflammation. Adrenal androgens are mostly metabolized by aromatase in adipose tissues to estrogens [17]. Obesity and particularly excess visceral fat may be complemented with the reduced production of the sex hormone-binding globulin (SHBG), which binds circulating hormones, disrupting the hormonal activity toward sensitive tissues, and thereby influencing the delicate hormonal balance in the body.
Each kilogram of excessive body weight is correlated with an increased risk of uterine fibroids development. A study conducted in the United States found that women diagnosed with uterine fibroids are heavier than those without uterine fibroids. Moreover, an increase in the body mass index (BMI) by one unit, higher waist-to-hip ratios, and body fat percentage exceeding 30% [18] increase the risk for uterine fibroids. Abdominal visceral fat also enhances this risk.
Obesity is most prevalent among African Americans compared with other racial and ethnic populations in the United States, contributing to the higher risk of developing uterine fibroids in the African American population. Uterine fibroids occur more frequently in obese postmenopausal women and those who have undergone hormonal replacement therapy. Furthermore, obese women diagnosed with type 2 diabetes are more likely to develop uterine fibroids, and this observation has been related to elevated concentrations of insulin-like growth factor (IGF-1). Insulin resistance plays a role in the development of uterine fibroids in obese women.
There is a direct correlation between arterial hypertension and uterine fibroids [19-21]. Increased diastolic blood pressure is associated with a higher risk of uterine fibroids, regardless of use of antihypertensive drugs [20]. Women suffering from hypertension are 5 times more likely to develop uterine fibroids and earlier diagnosis of hypertension is a significant factor. The formation of lesions is attributed to the chronic destruction of the myometrium due to increased blood flow and cytokines secreted by injured myometrial cells [20].
Hormonal disbalance also plays a crucial role in the development of the fibroids, thus the poor liver function and conditions such as hepatitis can also be the contributing factor in the development of the fibroids and endometriosis.
To identify the pathogenesis of uterine fibroids, some studies have reported the association between fibroids with uterus infection and chronic inflammation and it has been stated that with different mechanisms such as Extracellular matrix (ECM) protein increase, cytokine expression, etc., inflammatory conditions in both general and local endometrium can be effective in causing uterine fibroids [22-25].
Ciebiera, et al., [25] reported that TNF-a is one of the most important cytokines that are related to the biology, complaints, and symptoms of uterine fibroids. It has been estimated that there is higher concentration of TNF-a and the existence of inflammation status in women with uterine fibroids.
Chronic endometritis is defined as resistant inflammation in the uterine endometrium. The diagnosis of chronic endometritis in histology is the detection of the presence of plasma cells in the endometrial stroma. Plasma cell identification is performed using haematoxylin-eosin staining on paraffin-impregnated wax-embedded endometrial specimens, which is the gold standard method for the diagnosis of chronic endometritis [26,27]. Song reported that the prevalence of chronic endometritis in non-menopausal women was 24% and higher prevalence was noted in cases of recurrent implantation failure, abnormal uterine bleeding (AUB), endometrial hyperplasia and submucosal fibroids.
In the present study, which aimed to evaluate the association between chronic endometritis with uterine fibroids in non-menopausal women, the overall incidence of chronic endometritis was 43% (43 out of 100).
It has been stated that inflammatory conditions in both general and local endometrium can be effective in causing uterine fibroids with different mechanisms such as increased ECM protein, expression of cytokines, etc. [8-10]. If the uterus had chronic inflammation by inflammatory factors such as injury, infection, menstruation inflammations, etc., it causes the imbalance of the immune system through increased T helper cytokines and decreased function of target cells (Tregs) and the inflammatory response of the immune system leads to fibrosis tissue formation and proliferation. Chronic inflammation increases estrogen and ultimately increases myoma growth [28]. A study in the Netherlands reported that serum levels of cytokine inflammatory factors like interleukin-1 alpha were higher in patients with uterine fibroids than in the control group [29].
Uterine fibroids are associated with heavy menstrual bleeding, abdominal discomfort, subfertility and a reduced quality of life. The present study reported a case series of life-threatening anemia with hemoglobin levels < 2.0 g/dl caused by uterine fibroids and genital bleeding.
Symptomatic leiomyomas represent a major cause of hospitalization, particularly those associated with abnormal uterine bleeding (AUB) and anaemia. The aim of this study was to identify predictors of anaemia in women hospitalized due to uterine leiomyomas and evaluate its impact on treatment management and clinical outcomes.
Results: A total of 100 patients were hospitalized due to uterine leiomyomas during this period. Of those, 28.9% presented with anaemia. Age, obesity, intramural type of leiomyoma and AUB are independent predictors of anaemia (p < 0.001, AUC 0.7056).
Anemia has a significant impact on treatment approaches and clinical outcomes of women hospitalized for uterine leiomyomas. Age, obesity, intramural leiomyomas and AUB are some predictors of anaemia that could represent a risk-stratification opportunity, allowing for its prompt identification and correction, therefore improving patient care.
This study retrospectively investigated records of uterine myoma patients treated at JSC Central Clinical Hospital between January 2021 and November 2022. A total of 100 patients were included in this study, including the prognosis of the patient, MuClinical and pathological characteristics.
Minimal age of the patients were 23 and the maximum was 74, the mean number of age was 47.
• Presence of a complete clinical history and obvious clinical manifestations.
• Uterine myoma diagnosis.
This study was approved by the medical ethics committee of JSC Central Clinical Hospital (Date: 2022 October).
Age, BMI, menopausal status, lesion average diameter, presence of hypertension or diabetes mellitus, operation method, myoma type and location, presence and number of uterine fibroids, and pelvic adhesion information. Data was analyzed using meta analysis statistical software. Counting data were expressed as [n (%)] and compared using χ2 tests, while factors affecting patient prognosis were analyzed by multivariate logistic regression. P values less than 0.05 were considered statistically significant.
Patient age ranged from 23 to 75 years, with an average age of 60.83 ± 8.76 years (Table 1, Figure 1 and Figure 2).
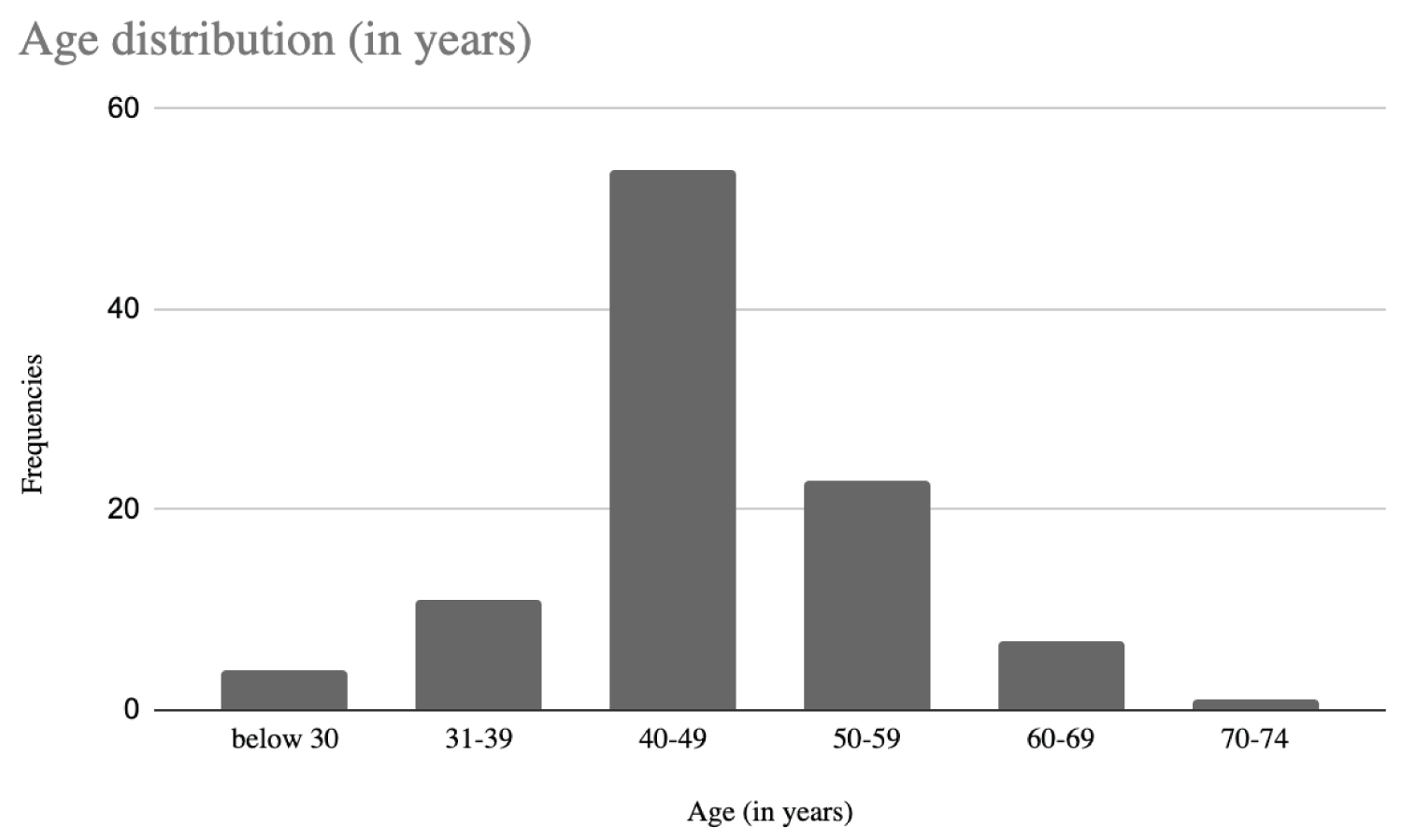 Figure 1: Patient age ranged from 23 to 75 years, with an average age of 60.83 ± 8.76 years.
View Figure 1
Figure 1: Patient age ranged from 23 to 75 years, with an average age of 60.83 ± 8.76 years.
View Figure 1
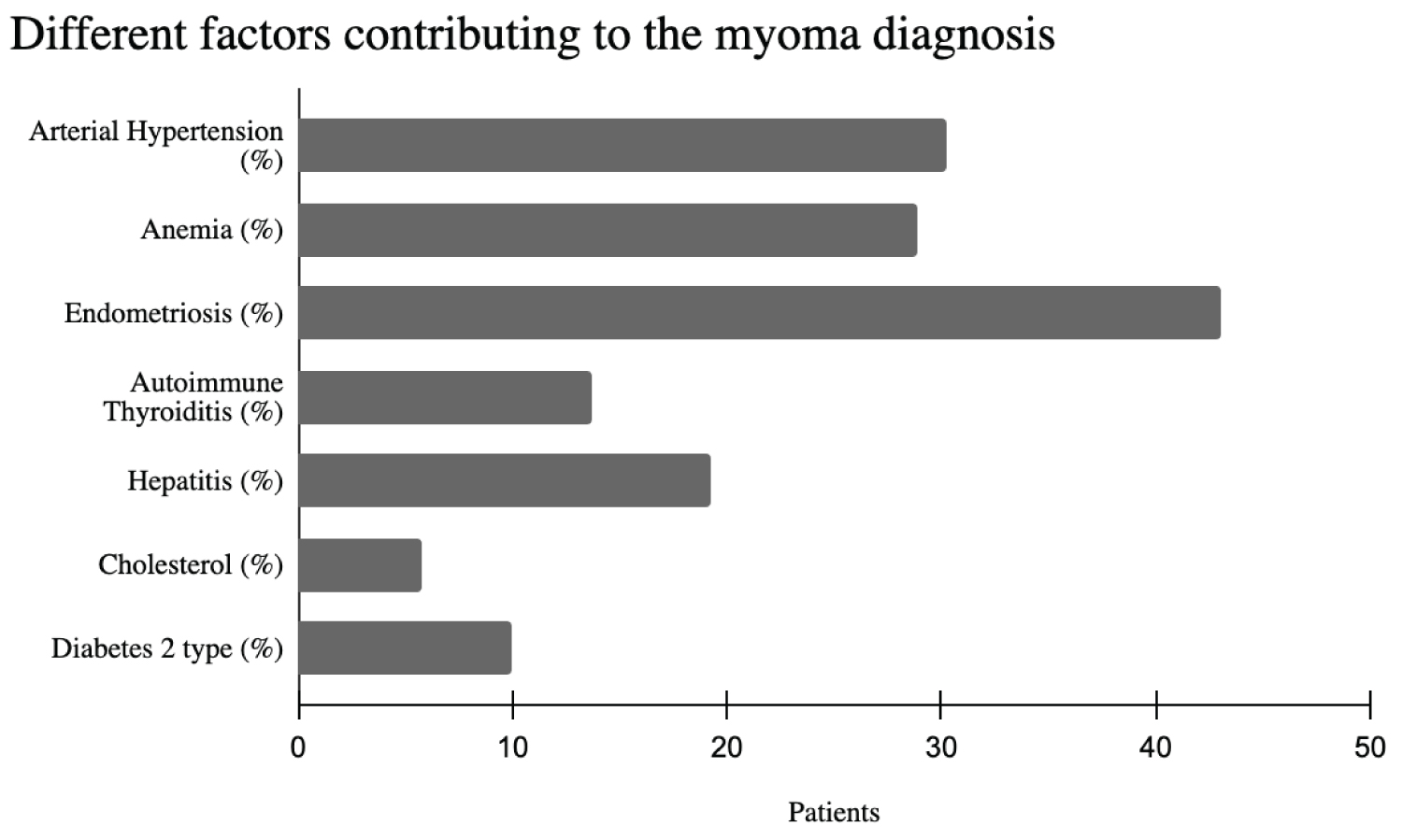 Figure 2: Different Factors Contributing to the myoma diagnosis.
View Figure 2
Figure 2: Different Factors Contributing to the myoma diagnosis.
View Figure 2
Table 1: Of all the patients, 121 had good prognosis and 28 had poor prognosis. View Table 1
This study showed that age equal to or greater than 60 was a risk factor affecting uterine myoma prognosis. This effect is potentially due to an age-related decline in physical and immune functions that results in a greater risk of endometrial hyperplasia caused by stimulation, as well as in greater physiological impact from surgical intervention. Our results are supported by previous studies. Such as, the study of 100 patients with uterine myoma also showed that age was positively correlated with tumor volume, while a study of 100 patients with endometriosis concluded that patient age is an important prognostic factor for endometrial cancer that is independent of other parameters [14].
This investigation shows that pelvic adhesion is a prognostic factor of uterine myoma, which is consistent with previous researchers. Previous study, investigating primary endometrioid carcinoma with and without myometrial infiltration, as well as 20 cases of regional lymph node metastasis found that myometrial infiltration was an independent prognostic parameter of endometrioid carcinoma associated with pelvic and/or paraaortic lymph node metastasis risk [17]. Finally, four or more myomas in a patient were found to be a risk factor, probably due to a fact that in cases of multiple myomas, intervention requires more incisions on the surface of the uterus, leading to higher risk of postoperative adhesions [18].
This study analyzed the pathological characteristics of patients with uterine myoma, which may help improve the accuracy of disease diagnosis. Age is risk factors affecting the prognosis of uterine myoma and can provide a reference for clinical treatment.
None.