Background: Urinary Tract Infections (UTI) are among the most common bacterial infections, and appropriate antimicrobial therapy with agents that minimize resistance is crucial. Despite international concern, adherence to guidelines is still suboptimal. This study aims to determine the effect of the absence of national guidelines and the rate of conformity to international guidelines among physicians in antibiotic prescriptions for the treatment of UTIs in adults; and detect the factors that are associated with a higher rate of non-compliance.
Methods: Patient-related characteristics and the prescribed antibiotics were gathered from patients' medical files, and a questionnaire was directed to physicians to elicit the factors involved in decision-making. Four criteria were evaluated: Molecule conformity, Daily Dose conformity, Duration conformity, and Global conformity.
Results: 37 Lebanese physicians and 185 prescriptions were included. The most prevalent class of antibiotics was fluoroquinolones (30.3%). Global conformity to guidelines was 31.4%, while conformity on drug choice, daily dose, and duration of treatment were 83.2%, 74.7%, and 41.6% respectively. There were no differences in conformity rates according to the physician's specialty (p = 0.135). Physicians who studied in an American system university had an increased risk of non-conformity, (A or = 2.107, p = 0.018). Patients with higher education levels, or presenting with fever or chills, were more likely to get a non-compliant prescription (a OR = 2.140, p = 0.032 and a OR = 4.947, p = 0.033 respectively).
Conclusion: In a country with no local guidelines, non-conformity to international guidelines is high. Larger national studies are needed with immediate interventions to enhance physicians' prescribing practices.
Compliance, Conformity, Antibiotic, Urinary tract infections, Prescriptions, Guidelines
AAFP: American Academy of Family Physicians; ATB: Antibiotic; EAU: European Association of Urology; GEE: Generalized Estimating Equation; IDSA: Infectious Diseases Society of America; LOP: Lebanese Order of Physicians; SD: Standard Deviation; SPILF: Société de Pathologie Infectieuse de Langue Française (French Language Infectious Diseases Society); UTI: Urinary Tract Infection; WHO: World Health Organization
Urinary Tract Infections (UTI) are among the most common bacterial infections in humans [1-5]. Women are significantly more affected than men: One in three women will have at least one episode of UTI by the age of 24, and roughly 50% of women will experience a UTI in their lifetime [3].
UTIs are classified according to the site of infection (pyelonephritis, cystitis, urethritis, prostatitis) and the presence of risk factors for complications [3,6]. While asymptomatic UTIs are left untreated in most cases according to guidelines, the high incidence of symptomatic UTIs that require antibiotics emphasizes the need to ensure appropriate therapy with agents that maximize success and minimize the risk of resistance [4,6].
According to the World Health Organization (WHO), rational drug use requires that patients receive drugs appropriate to their clinical condition, in doses that suit their needs, for an adequate period of time and at the lowest cost for themselves and their community [7].
Additionally, the increasing use of antibiotics (ATB) has an impact on bacterial resistance trends and the WHO has warned that antimicrobial resistance is today one of the biggest threats to global health [8]. Despite this international concern, adherence to guidelines is still suboptimal, with concordance averaging around 30% in many countries [9-15]. Factors related to non-adherence are physician’s specialty, age or patient load, some patient’s characteristic (fever, desire for antibiotics, longer duration of symptoms, insurance type) and healthcare system-related factors (time pressure and policies/guidelines implemented) [16-23].
In Lebanon, ATB resistance levels are high: in particular, Escherichia coli and Klebsiella spp, causing common community-acquired infections, are significantly resistant to many antibiotics, mainly to internationally recommended drugs for empiric treatment of these infections like UTIs and intra-abdominal infections [24,25]. Unfortunately, until 2017, Lebanon had no national directives on UTI treatments [26] and physicians had to rely on international recommendations to guide their choices. Although small studies have been conducted in Lebanon to assess the compliance of ATB prescriptions with some international recommendations, they had multiple limits because, as the data were being collected in pharmacies and not in a doctor’s clinics, physician-related factors and detailed patient characteristics were not assessed [23,27]. This study will be the first to evaluate the conformity of antibiotic prescriptions to guidelines specifically in UTIs at the physician level, and the first to our knowledge to describe the practice of physicians who rely on international guidelines in a country with no local guidelines.
The objectives of our study are thus to determine the prevalence of conformity to international guidelines among Lebanese physicians in ATB prescriptions for the treatment of non-hospitalized acute UTIs in adults and identify the factors that are associated with a higher rate of non-compliance to guidelines.
This is a cross-sectional survey of physicians practicing in Lebanon between March and August 2016. Physicians most likely to treat UTIs were selected: General practitioners, specialists in urology, infectious diseases, gynecology, internal medicine, and family medicine.
We chose to select 5 prescriptions per physician to keep a small cluster size and minimize selection bias. Consequently, with an acceptable margin of error of 7%, a design effect of 1 and an expected frequency of conformity of 35%, a sample size of 185 prescriptions from 37 physicians were required with a confidence level of 95%.
Physicians’ selection: Sampling by convenience from the exhaustive list of specialists provided by the Lebanese Order of Physicians (LOP) was done until we reached the calculated minimum sample size of 37 physicians.
Prescriptions’ selection: Each physician was visited once by the researchers and asked to provide his last 10 antibiotics prescriptions for the treatment of a UTI, The medical records were then reviewed for eligibility criteria, and 5 patients were randomly selected from all eligible records. Eligibility criteria were defined as follows:
• Patients 18-years-old or above;
• Diagnosis of simple or complicated cystitis, simple or complicated pyelonephritis, or prostatitis based on physician’s appreciation and notes in the medical record;
• Outpatient treatment with an oral or intramuscular antibiotic;
• Patient not known to have a psychiatric illness, concurrent infections, sexually transmitted diseases, or candidiasis
Data were collected using a questionnaire which included two sections. The first section was drawn from medical records and comprised the socio-demographic characteristics of patients, their diagnosis, comorbidities, risk factors for resistant UTIs (recent hospitalization, surgery, use of ATB) and symptoms; the doctor's diagnostic methods, and the prescribed antibiotics. The second section was as self-administered questionnaire for doctors, and included their socio demographic characteristics, specialty, practice characteristics (location, number of patients), and factors likely to be involved in decision-making such as their subscription to medical journals or their tendency to prescribe ATB when they are unsure of the diagnosis, as well as some additional factors. The American crowding index was calculated: Crowding occurs if there is more than one person per room; severe crowding occurs if there are more than 1.5 persons per room (excluding bathrooms, balconies, porches, foyers, hall-ways and half-rooms) [28].
In the absence of Lebanese guidelines before 2017, physicians relied on international recommendations to guide their prescriptions, primarily those of the Infectious Diseases Society of America (IDSA) [29], the French Language Infectious Diseases Society (SPILF) [30] and the European Association of Urology (EAU) [6]. Thus, the guidelines adopted by each physician can be different. This is mainly driven by the medical school or hospital they specialized in. For that reason, we compiled the recommendations of the IDSA, the SPILF, and the EAU, and any first-line or second-line antibiotic that was recommended in at least one of those guidelines was considered correct (Appendix 1).
Each prescription was evaluated for compliance of molecule choice, daily dose, and duration of treatment to any of the guidelines. Global conformity was then computed: Treatment was considered generally compliant if all three conformities described above were in accordance with any of the recommendations.
Descriptive data for physicians’ and patients’ characteristics, as well as conformity results, were presented using their mean and Standard Deviation (SD) for quantitative continuous variables and the frequency and percentage for categorical variables. To identify the factors associated with prescriptions’ non-conformity to guidelines, we first performed bi variate analysis using a separate Generalized Estimating Equations (GEE) model for each factor and by taking conformity as reference. GEE was chosen to account for correlation of data coming from the same physician. The independent variables that were associated with non-conformity with a p-value < 0.2 were then included in nested GEE models according to variable groups (physicians’ socio-demographic variables, patients’ socio-demographic variables, patients’ symptoms and medical status, diagnosis and diagnostic modalities). Finally, all the variables associated with non-conformity with a p-value < 0.05 in the different GEE models were included in one final model. Results were presented with their adjusted odds ratio (a OR) and their p-value. Analyses were performed using Statistical Package for Social Sciences (SPSS) software version 22.0. A p-value < 0.05 in the final model was considered statistically significant.
Anonymity and confidentiality were respected throughout the study by codification of identification data. An oral consent was given by participating physicians. There are no conflicts of interest to report. The study was approved by the Institutional Review Board (2020RC-044-LIUSOP).
This study included a total of 37 physicians and 185 patients. Physicians’ and patients’ characteristics are summarized in Table 1 and Table 2. Notably, the distribution of factors involved in the physician decision-making was almost similar for all the included physicians.
Table 1: Characteristics of physicians (n = 37). View Table 1
Table 2: Characteristics of patients (n = 185). View Table 2
In general, almost all physicians relied on the clinical evaluation to establish the diagnosis. While urine analysis and culture were prescribed in 49% and 27% of simple cystitis cases respectively, they were almost universally prescribed for the remaining types of UTIs.
The most frequent diagnosis in our sample was simple cystitis (71.4% of cases), followed by prostatitis (18.9%) (Table 3). While simple cystitis is, normally, only found in women (because a UTI is, by definition, always complicated in men), we note that 20 patients with simple cystitis (15.2%) in our sample were men.
Table 3: Prevalence of each UTI diagnosis in the sample (n = 185). View Table 3
Cultures were positive in 47.6% of cases. The most frequent germ detected was Escherichia Coli (51.2%). The most frequently prescribed antibiotic was Amoxicillin clavulanate, while the most prevalent class was fluoroquinolones (Figure 1 and Appendix 2).
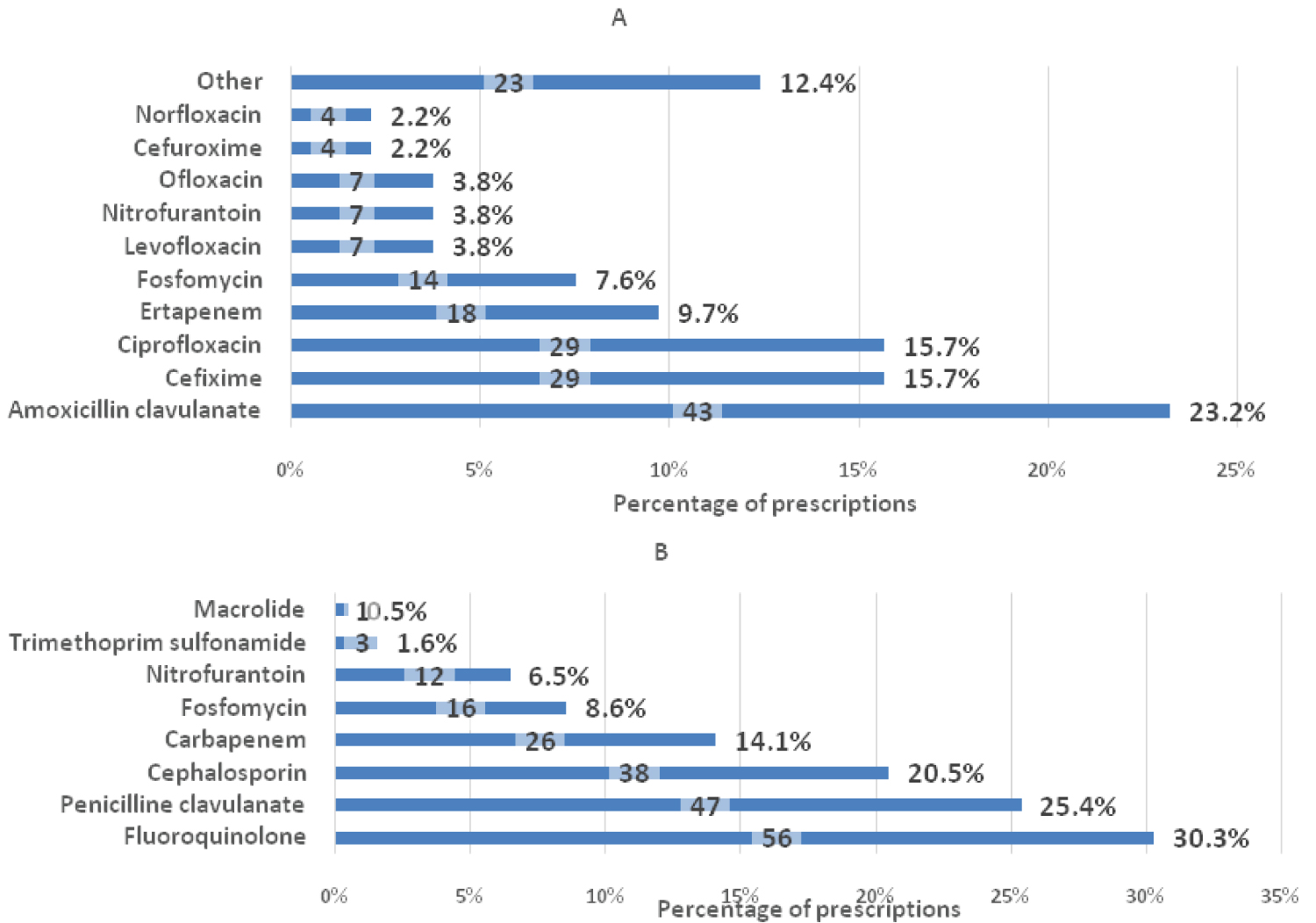 Figure 1: Antibiotics prescribed for UTIs. (A) Percentage of antibiotic regimen prescribed for all UTIs combined. Molecules prescribed in less than 2% of cases were grouped under Other. (B) Percentage of antibiotics prescribed by class. The actual count of prescriptions is indicated in the center of each bar (n = 185).
View Figure 1
Figure 1: Antibiotics prescribed for UTIs. (A) Percentage of antibiotic regimen prescribed for all UTIs combined. Molecules prescribed in less than 2% of cases were grouped under Other. (B) Percentage of antibiotics prescribed by class. The actual count of prescriptions is indicated in the center of each bar (n = 185).
View Figure 1
Prevalence of global conformity to guidelines was 31.4%. In most cases of simple cystitis, the choice of drug was compliant with guidelines (93.9%), while the duration of treatment was correct in 45.2% of cases, with a tendency towards longer treatments. For instance, in simple cystitis, Ciprofloxacin and Nitrofuratoin were prescribed for a longer duration than recommended in 79% and 85.7% of cases respectively. Two molecules were notably prescribed for shorter than recommended durations: Cefixime in simple cystitis (6 days instead of 7 days in 96% of cases), and Ertapenem in prostatitis (7 days instead of 10 to 14 days in 42% of cases). In prostatitis, global conformity was 8.6%, with a drug choice conformity of 57.1% and a duration conformity of 15%. Other conformity results are shown in Figure 2.
 Figure 2: Conformity to guidelines (%).
View Figure 2
Figure 2: Conformity to guidelines (%).
View Figure 2
Results of the bivariate analysis are shown in Appendix 3 and Appendix 4. Physician specialty was significantly associated with non-conformity in the bivariate analysis (p = 0.002): Compared to primary care physicians, the odds of non-conformity were approximately three times higher in urology or nephrology specialists, while they were significantly lower in gynecologists. However, this association disappeared after adjustment for confounding variables in the multivariate analysis (p = 0.135). Non-conformity to guidelines was statistically associated with having studied in an American system university (a OR = 2.107, p = 0.018). All other factors related to physicians had no effect on non-conformity. Similarly, non-conformity was associated to 2 patient-related factors: Patients with a higher education level, as well as patients presenting with fever or chills, were more likely to get a prescription that was not compliant with the guidelines (a OR = 2.140, p = 0.032 and a OR = 4.947, p = 0.033 respectively) compared to others. Multivariate analysis results are presented in Table 4, while detailed results of the nested model multivariate analysis are presented in Appendix 5.
Table 4: Multivariate analysis results for global non-conformity (n =185). View Table 4
This study is, to our knowledge, the first in Lebanon to evaluate the conformity of antibiotic prescriptions to international guidelines, in the absence of local guidelines, specifically in UTIs and at the physician level. Around 70% of all antibiotic prescriptions for UTIs were not compliant with guidelines. Non-conformity was related to the university educational system of the physician, to the educational level of the patient and to the patient presenting with fever or chills. Our results raise several important points and major problems related to the absence of well-defined local guidelines for antibiotic prescriptions and the reliance on international guidelines.
Only 30% of overall prescriptions in our sample were compliant with international guidelines. This rate is similar to the ones found by Saleh, et al. in 2014 and Kabbara, et al. in 2018 when they assessed antibiotic prescriptions in pharmacies [23,27]. It is also concordant with reports from other countries, such as Spain, the USA, and France [11-15]. In Taiwan however, studies that evaluated conformity to the local guidelines in 2007 and 2011 found high percentages of 70% and 80% [31,32].
We note that physicians prescribed confirmatory urine analysis in almost all cases of UTIs except in simple cystitis, where the prevalence of urine analysis was around 50%. This is in accordance with international guidelines, which state that simple cystitis can be diagnosed and treated empirically [6,30]. Specifically, the American Academy of Family Physicians (AAFP) report that women who self-diagnose a UTI may even be treated safely with telephone management [33].
Fluoroquinolone use is still prevalent in Lebanon, despite recommendations to avoid them as a first-line treatment when possible [29]. These results are similar to those found in France, Germany and the USA [34,35]. This may be a remnant of the time when quinolones were first discovered and included in guidelines as first-line antibiotics [36,37]. Additionally, as these molecules are recommended today as the first-line treatment in pyelonephritis, some physicians may be prescribing them in virtually all cases of cystitis to feel more secure by covering an eventual unsuspected pyelonephritis.
We found that molecule conformity was elevated (83%), which is higher than previous reports from Lebanese pharmacies (35% to 61%) [23,27]. While this number may seem encouraging, it may be artificially elevated because our compilation of multiple international guidelines included more treatment options than each guideline separately and because second-line agents were also considered appropriate for the lack of a detailed medical history. Indeed, molecule conformity rates are less than 50% in France, Lebanon and the USA in studies that only consider first-line agents [11,23,36].
In general, our results suggest that physicians in Lebanon tend to choose antibiotics with broader indications and coverage. This could be due to most medical training being made in in-hospital settings, or to extrapolation from other infection types with similar pathogens for which more data are available in Lebanon. Indeed, since our data collection was completed, local guidelines by the Lebanese Society of Infectious Diseases and Clinical Microbiology were published and they confirmed the appropriateness of broad-spectrum antibiotics in UTIs other than simple cystitis in Lebanon, because of the local epidemiology of third-generation-cephalosporin-resistant organisms [24,26].
When the drug choice was appropriate, dose conformity was generally high, ranging from 71% to 100% according to the diagnosis. This is similar to the 2018 Lebanese study [23] and could be explained by the fact that most drugs, like Fosfomycin, nitrofurantoin, or ertapenem have one standard dosing regimen thus errors are inexistent in that case. Dose conformity was lowest in simple cystitis, mainly driven by prescriptions of Ciprofloxacin and Levofloxacin. While they are recommended as second-line antibiotics at low doses (250 mg twice a day), they were prescribed in 100% of cases at a standard daily dose of 500 mg twice a day.
Duration conformity, which is the lowest of all 3 conformities, follows the same trend. In most cases, treatment durations were too long. Ciprofloxacin and Levofloxacin, which should be prescribed for 3 days only in simple cystitis, were given for up to 7 to 15 days in many cases; nitrofurantoin was given for 7 days instead of 5 in two-thirds of cases. One notable exception is cefixime, which, in almost all cases (21 of 25 prescriptions), was given for a total of 6 days instead of 7 days. Upon looking into the brands available in Lebanon, it appeared to us that the most common brand is sold in boxes of 6 pills. Because in Lebanon, drugs are sold to the patient in full boxes and not as an exact number of pills like other countries, it seems that physicians take this point into account and prefer giving the drug for one day less, instead of letting the patient buy an additional box to use one additional pill only.
In prostatitis, it is recommended to initiate treatment for at least 2 weeks, then the patient should be reassessed for the need of prolonging the course for up to 6 weeks [6,30]. Therefore, initial empiric prescription should be for 2 weeks only. In our sample, more than 50% of prescriptions were for 3 weeks or more. Interestingly, of the 12 prescriptions of ertapenem, 5 (41.7%) were given for a noticeably short duration of 7 days. While we had to count them as non-compliant with guidelines, it is possible that, due to the high price of this molecule in Lebanon (around 50 USD per dose) [38], physicians asked the patients to buy a limited number of ampoules while awaiting the urine culture results because there was a chance they would be able to change it or de-escalate treatment later.
These results concur with international literature and previous Lebanese findings; treatment duration of UTIs is inappropriate in many parts of the world [14,17,23,27,36,39,40]. In particular, a big cohort of 654,432 women in the USA showed that > 75% of prescriptions were written for non-recommended treatment durations [11]. Explanations may be the same as described above: partial knowledge of the guidelines, multiplicity of guidelines, extrapolation from other infections where standard treatment is around 7 to 10 days, sense of security of the physicians when they prescribe longer treatment courses, or regulation problems that lead to dispensing full boxes of drugs instead of the exact number needed.
Our results found that presence of fever and chills was one of the most determinant associated factors for non-conformity, with an odds ratio of approximately 5. This is higher than what was found in other studies focusing on respiratory tract infections, where the OR were around 3 [19,21,22]. Physicians seem to be more prone to give inappropriate prescriptions when patients present with more severe features; although these symptoms are usually diagnostic criteria of pyelonephritis or prostatitis which raises the possibility of inappropriateness being linked to the diagnosis and not to fever itself.
Physicians from an American system university were at risk of non-conformity with an OR of 2.1. As this multiplicity of educational systems in Lebanon is somehow rare in other countries, it is difficult to establish comparisons with other studies. However, we think that this association can be the result of the difference in guidelines between Europe and the USA, as in some cases, American guidelines and reviews adopt a different classification of UTIs where any infection extending beyond the bladder is considered complicated (i.e. there is no uncomplicated pyelonephritis) [29,41]. Additionally, American system universities included in our study have 2 or 3 university hospitals for training, while physicians from French system universities, especially the Lebanese University, are scattered across a multitude of small to middle-sized hospitals. Therefore, it is possible that the big American hospitals report their susceptibility patterns more frequently and have more standardized internal prescribing guidelines, so that physicians already know which antibiotics would be more recommended in their settings while the other physicians must stick to the international recommendations due to not having any standardized guide common to the many hospitals that they train in.
In our adjusted model, physician’s specialty, gender, and other intrinsic factors were not associated with conformity. Our results are almost identical to those described in the systematic review by Rodrigues, et al., and corroborate the conclusion of Veninga, et al. who commented that non-conformity in antibiotic prescriptions are mostly due to factors unrelated to the physicians themselves [16,42]. Interestingly, patients with higher educational degrees in our sample were more at risk of receiving inappropriate prescriptions than others. We think that they may tend to search for information about their symptoms and treatments, and to insist on getting more potent antibiotics, although physicians stated that they do not let themselves be influenced by a patient’s request.
This is an observational study that included a small number of participants and a high refusal rate of physicians; it may not be powered enough to identify the factors associated with poor adherence to guidelines. The sampling that had to be completed by convenience introduced a selection bias although post-hoc comparison showed that the distribution of physicians from French- and American-system universities is similar to the Lebanese physicians’ population [43,44]. A confounding bias may be present, due to some factors affecting conformity not taken into consideration. Finally, our compilation of multiple international guidelines may have led to artificially increasing our conformity rates, while the lack of information on the patients’ infectious history may have decreased these rates by labeling an informed prescription (which should have thus been excluded) as non-compliant with empiric guidelines.
The strengths of our study lie in the fact that, to our knowledge, this is the first Lebanese study to evaluate the rationality of antibiotic prescriptions for UTIs in doctors' outpatient clinics and not from prescriptions collected in pharmacies. Doctors from all specialties who treat UTIs were included, unlike many studies that evaluated compliance only among general practitioners or emergency room doctors. For our conformity criteria, and despite the drawbacks described earlier, we considered the most prominent recommendations that are followed in Lebanon and created a global conformity-appraisal algorithm that takes them all into account, instead of relying on only one specific guideline; this allowed us not to over-estimate the prevalence of non-conformity.
Non-conformity of Lebanese-physicians to international guidelines is high, and a majority of UTIs is still treated with fluoroquinolones. Now that Lebanese guidelines are available, national studies are needed to compare the results and assess the impact of their publication. Because suboptimal antibiotic prescribing can result in decreased efficacy, prolonged patient morbidity, and increased healthcare costs, there is a crucial need for immediate interventions in countries with no local guidelines to enhance physicians’ prescribing practices.
Not applicable.
The authors certify that they have NO affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
The study was approved by the Institutional Review Board (2020RC-044-LIUSOP). All methods were conducted in accordance with the ethical standards of the declaration of Helsinki. Each physician was informed of the course of the study and gave an oral consent for their inclusion and use of the data.
Not applicable.
The datasets generated and/or analyzed during the current study are available in the Mendeley repository, with the DOI: 10.17632/98p49gmm5v.1.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
All authors participated equally to this study. JK was the main investigator, he did the statistical analysis and wrote the main manuscript text. NS, NL and MH supervised the study progress and coordinated the data collection. MH, NS and PM participated in writing the study protocol. All authors reviewed the manuscript.