Tinea corporis is a common pruritic rash that is frequently seen by family medicine physicians. Tinea incognito is an exacerbation of a dermatophyte infection due to topical corticosteroid use that is commonly prescribed to alleviate pruritis. We present a case of a 73-year-old male with an itchy rash on his chest worsened by previously prescribed topical corticosteroids, with skin scrapings consistent with tinea incognito. We herein review clinical features, diagnostic techniques, and proper treatment of tinea incognito to prevent progression of infection, as well as proposed solutions to challenges that family physicians may face in the diagnosis of tinea incognito.
Tinea corporis is a pruritic fungal infection of the skin commonly caused by Trichophyton rubrum and is treated with topical antifungals. The lifetime risk of acquiring a tinea infection is between 10 and 20 percent [1]. Pruritic rash is a common chief complaint for family physicians, with topical corticosteroids frequently prescribed for pruritis. Tinea incognito is an exacerbation of a dermatophyte infection due to topical corticosteroid use [2]. The wide variety of clinical presentations deems tinea incognito a great imitator, mimicking common dermatological diagnoses such as nummular eczema, granuloma annulare, and psoriasis [1]. The treatment for these common conditions is topical corticosteroids, highlighting the importance of correct diagnosis and treatment by family medicine physicians to prevent further exacerbation of tinea infections.
A 73-year-old immunocompetent male presented to the dermatology clinic with a 3-month history of itchy rash on his chest. The lesion was an erythematous, annular plaque with minimal scaling on the periphery (Figure 1). Physical exam was additionally remarkable for subungual debris with dystrophy and discoloration of the toenails on the right foot. The patient denied a prior history of similar rash and reported self-treatment with prescription-strength topical steroid cream for one month. The patient noted that the rash had expanded following treatment with the steroid, prompting evaluation. Scrapings of the peripheral scaling of the lesion were obtained and prepared for microscopic examination with potassium hydroxide. Light microscopy revealed branching hyphae consistent with dermatophyte infection (Figure 2), confirming the diagnosis of tinea incognito. The patient was advised to discontinue the use of topical steroids and was prescribed a 3-week course of 1% butenafine hydrochloride cream, after which he reported complete resolution of the rash.
 Figure 1: Erythematous, annular plaque on left upper chest.
View Figure 1
Figure 1: Erythematous, annular plaque on left upper chest.
View Figure 1
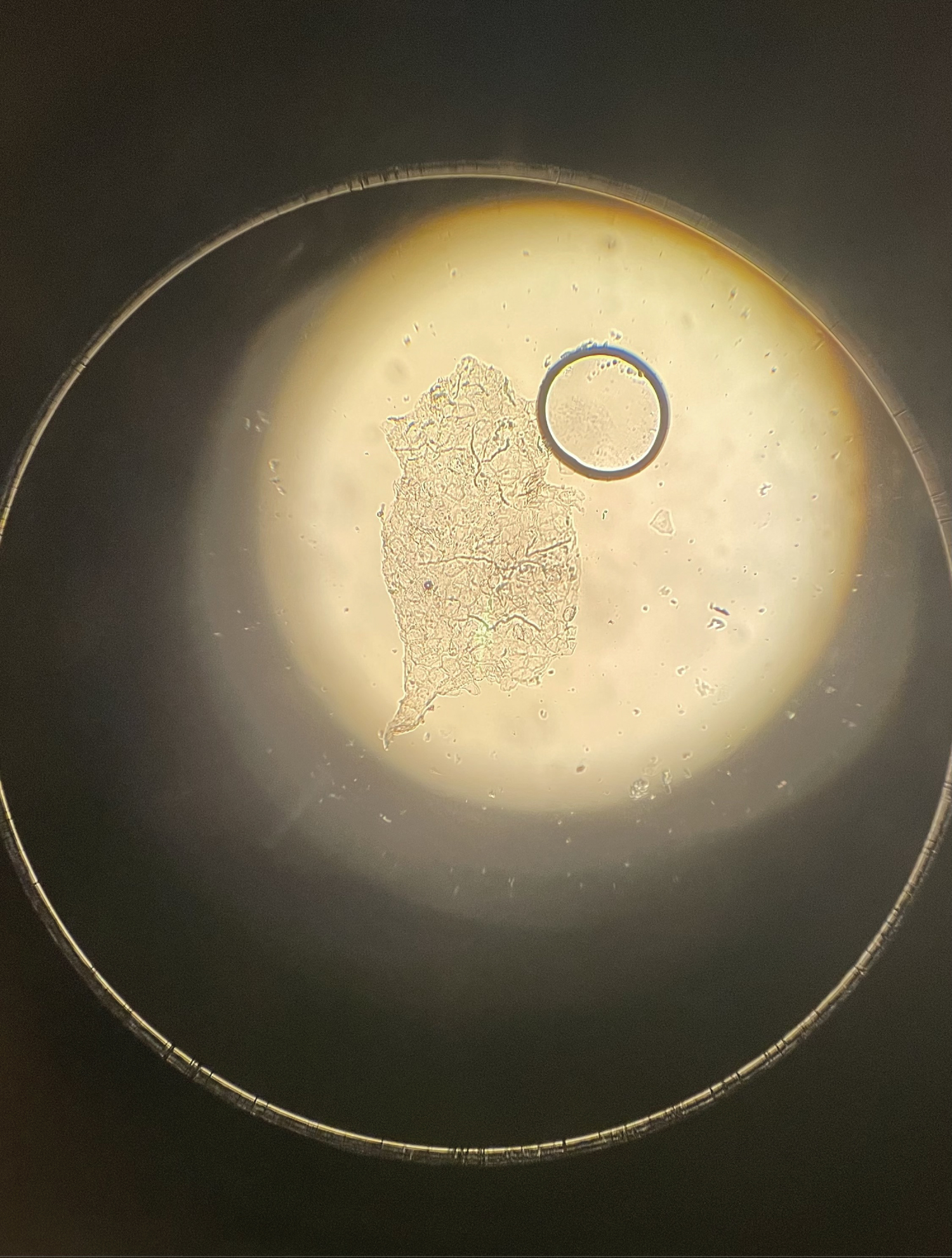 Figure 2: Light microscopy of potassium hydroxide preparation of peripheral skin scaling showing dermatophyte hyphae.
View Figure 2
Figure 2: Light microscopy of potassium hydroxide preparation of peripheral skin scaling showing dermatophyte hyphae.
View Figure 2
Tinea incognito was first described in 1968 as an infection in which dermatophytes are able to proliferate freely [2]. This is due to the blunted cutaneous immune response that occurs after application of topical corticosteroids, which have an anti-inflammatory and anti-mitotic mechanism [3]. Although topical steroids are the most common cause of tinea incognito, literature has also described topical calcineurin inhibitors such as tacrolimus as exacerbating agents, as well as mixed drug combination creams that contain a steroid, an antifungal, and an antibacterial agent [4].
Classic tinea infections present as well-demarcated, itchy, annular plaques with raised scaly borders and central clearing. Lesions generally range in size from 1-centimeter to 5-centimeters, may be single or multiple, and commonly occur on the trunk, limbs, face, and scalp. As infections progress to tinea incognito, cutaneous findings become atypical, as lesions are often less scaly, have a flatter margin, and may be more pustular and pruritic. Concurrent tinea pedis or onychomycosis often occurs simultaneously with tinea incognito, as seen in this case [4]. Predisposing factors for dermatophyte infection include underlying diseases such as lymphoma, diabetes mellitus, or immunocompromised status, as well as excessive sweating and old age.
The gold standard for diagnosis of tinea corporis is microscopic examination of potassium hydroxide preparation of skin scrapings showing fungal hyphae [3], although most family medicine practices do not have adequate access to resources for microscopic diagnosis. To alleviate unnecessary referrals to dermatology due to limited microscope access, family clinicians can send a scraping of the suspected fungal infection to the laboratory for microscopic examination or fungal culture. The scraping should be collected with a scalpel from the leading edge of the rash into a sterile urine cup. If laboratory findings are inconclusive or if the rash fails to improve with antifungals, patients should then be referred to dermatology for examination.
If tinea incognito is suspected, family clinicians may opt to treat patients with topical antifungals either alone or combined with systemic antifungals. Topical steroids for symptomatic relief should be avoided to prevent worsening of the fungal infection as topical steroids can allow tinea to travel deeper into the hair follicles, known as Majocchi’s granuloma. The standard treatment of Majocchi’s granuloma is oral antifungals, as topical antifungals do not penetrate deeply enough to eradicate the infection [5]. Oral terbinafine or itraconazole are preferred for systemic therapy, but it is recommended to measure serum transaminases before initiating treatment with terbinafine due to its hepatotoxic effects [6]. For localized cases of tinea incognito, topical antifungals should be prescribed for four weeks, or up to eight weeks in extensive infections [7]. Topical allylamines (e.g. terbinafine) and imidazoles (e.g. clotrimazole) are the mainstays of therapy for localized disease without concurrent onychomycosis.
We present a case of tinea incognito exacerbated by prescription of topical corticosteroids for pruritis. Inadequate access to light microscopes for examination of skin scrapings may lead to misdiagnosis or delayed diagnosis of tinea infections, with topical corticosteroids prescribed to control pruritis. Tinea incognito may have a misleading clinical picture, but if suspected, family physicians should consider collecting a scraping of the affected skin for outside laboratory review, as well as treatment with topical antifungals for four to eight weeks. If systemic antifungals are indicated, serum transaminases should be measured before initiation of treatment.
The authors report no conflicting or competing interests.
The authors did not receive funding for this manuscript.
There are no acknowledgments. All authors contributed equally.