The origin of COVID-19 originally named Novel coronavirus was Wuhan in China in December 2019. Renamed COVID-19 by the World Health Organization on February 11th 2020 [1] the virus is severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (WHO. Novel Coronavirus-China, 2020). Investigations linked the virus to a local Huanan South China Seafood Market in Wuhan, Hubei Province, China in December 2019 [2].
Coronavirus is a major pathogen belonging to a family of viruses that target the human respiratory system and may cause various symptoms such as pneumonia, fever, difficulty in breathing as well as lung infections [3]. SARS-CoV-2 is the seventh coronavirus known to infect humans, and the third zoonotic virus after SARS-CoV and MERS-CoV [4]. These viruses include the severe acute respiratory syndrome (SARS)-CoV and the Middle East Respiratory Syndrome (MER)-CoV all characterized as of public health threat [1]. As much as there are similarities in the symptoms between COVID-19 and earlier viruses such as fever, dry cough and dysnea, COVID-19 was found to show some unique clinical features that include the targeting of lower airway by upper tract symptoms like rhinorrhea, sneezing and sore throat with less gastrointestinal symptoms unlike SARs and MARs [3]. The clinical characteristics of patients hospitalized with COVID-19-related pneumonia at the height of the pandemic in Wuhan, China indicated that 26% were transferred to the ICU because of complications such as Acute Respiratory Distress Syndrome (ARDS) and shock [5]. Given the spread of the new coronavirus and its impacts on human health, the research community has responded rapidly to the new virus and many preliminary research articles have already been published about this epidemic [2].
On 31st December 2019, the WHO China Country Office was informed of cases of pneumonia unknown etiology (unknown cause) detected in Wuhan City, Hubei Province of China. From 31st December 2019 through 3rd January 2020, a total of 44 case-patients with pneumonia of unknown etiology were reported to WHO by the national authorities in China. During this reported period, the causal agent was not identified. The Emergency Committee on the novel coronavirus (2019-nCoV) under the International Health Regulations (IHR 2005) was reconvened on 30th January 2020. WHO declared the outbreak to be a public health emergency of international concern [6].
The official name of the 2019 novel coronavirus was announced by WHO as the coronavirus disease (COVID-19). The current reference name for the virus is severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). It was reported that a cluster of patients with pneumonia of unknown cause was linked to a local Huanan South China Seafood Market in Wuhan, Hubei Province, China in December 2019 [7].
The 2019-20 coronavirus pandemic was confirmed to have spread to Africa on 14th February 2020. The first confirmed case was in Egypt and the first confirmed case in sub-Saharan Africa was in Nigeria. Most of the identified imported cases have arrived from Europe and the United States rather than from China.
COVID-19 caused by SARS-CoV, has been associated with consumption of wild animals specifically linked to bats as the ecological reservoirs with suspicion that the intermediate animal host could be a domestic food animal, a wild animal, or a domesticated wild animal [6]; still under investigation to identify the intermediate animal as a recommendation made during the WHO Zoom meeting held on Friday 31st January 2020 pm, (Paris time). Bats have been identified as the source for a wide range of zoonoses. Bats are regarded as either delicacies or of medicinal value in a number of countries, particularly in East and Southeast Asia, the Pacific Islands and Sub-Saharan Africa including Madagascar. In Ghana, straw-coloured fruit bats (Eidolon helvum) are hunted in large numbers (over 128,000 annually in the south of the country alone) despite being potential hosts for a number of pathogens including the Ebola virus [8].
Our generation has witnessed key changes in the health needs of the world's populations. In Africa, we have witnessed the double burden of infectious and chronic diseases making up major causes of morbidity and mortality. There has been a rise in infectious diseases, which includes the Severe Acute Respiratory Syndrome Virus (SARS), the H1N1 pandemic influenza, the Ebolavirus and the Covid-19 virus. These diseases have rapidly spread across the world and created unprecedented connectivity that defines modern civilization. Though countries the world over have made significant progress towards improving global surveillance for Emerging Infectious Diseases (EIDs), the vast majority of Low-and Middle-income Countries (LMICs) have fragile health systems and various challenges which make them vulnerable to outbreaks and hence bring about dramatic social and economic consequences when they are reported [9].
Throughout the world, despite major advances in epidemic preparedness, Africa remains uniquely susceptible to a myriad of infectious diseases, especially the novel coronavirus disease 2019 (COVID-19). Twenty two of the twenty-five countries most susceptible to an infectious disease outbreak are in Africa, according to the Infectious Disease Vulnerability Index. The high prevalence of HIV, tuberculosis, and other pathogens might potentiate the severity of COVID-19 and contribute to diagnostic ambiguity. Health-care systems especially in Sub-saharan Africa are inadequate and human resources wanting. Although Africa is endowed with a youthful generation, with more than half the population aged below 20 years, which may be viewed as protective against Covid-19, it is of no comfort, since it also means that Africa may have much to lose in terms of disability adjusted life years [10].
Traditionally, the various cuisines of Africa use a combination of locally available foods such as, cereal grains and vegetables, as well as milk and meat products, and do not usually have food imported but also take cognizant that a number of Africa communities consume wild animal.
For over 5 decades now on the African continent the repeatedly reemerging infectious viruses have been, ebola viruses and related filoviruses. This has been across the equatorial belt of the African continent and they have been known to cause epidemics of highly fatal hemorrhagic fever. To virologists and epidemiologists, the most plausible answer to the emergence of this disease was from two different reservoirs (mammals) which eventually spilled over into humans. This indicated that viral reservoir hosts are species to which a virus becomes adapted over long periods of time, causing minimal or no disease in that host and being maintained via silent circulation within the host species either by host-to-host transmission or via intermediate hosts or vectors [11].
What the African communities eat can be viewed in the context of the diverse socio-cultural and economic environments. The food consumed is not the same throughout, although there are some striking similarities. Generally, Africans eat more grain foods, but most of them consume less than one serving of fruits per day. Locally available staples generally form the basis of a meal, but the meal becomes nutritionally adequate and tasty if a relish or soup (consisting of beans or groundnuts, vegetables, fats or oils, condiments and spices) and fruits are eaten with the staple. In most African communities, people rely on one or two staple crops. Most common are maize, teff, cassava, yam, sweet potato, plantain and enset. These crops provide the bulk of energy intake of household members. To balance their diet, consumers complement staple foods with legumes or foods from animal sources that are rich in proteins and fats/oil [12].
Commonly eaten fruits and vegetables in Africa include avocado, baobab fruit, citrus fruits, guava, mango, papaya, passion fruit, banana and jackfruit. Eggplant, gourd, green pepper, okra, squash, pumpkin, tomato, chilli, amaranth, spinach, leaves from baobab, cassava leaves, cowpea leaves, sweet potato and pumpkin leaves are among the vegetables commonly eaten [13].
Fruits are important in a diet as they are a good source of vitamins, minerals fiber and phytochemical substances. Vitamin C is important because of its role in healing wounds, fractures, bruises, and preventing bleeding gums. Potassium for keeping the body parts running smoothly and is involved in maintaining water and electrolyte balance and regulating nerve and muscle functions. Fruits are generally, good sources of potassium, Vitamin A, a fat-soluble vitamin plays an important role in vision, growth, bone development and normal reproduction. Folate is important for DNA metabolism. Vegetables are important in the diet because they provide vitamins, including vitamins A, C and folate and minerals including, iron and magnesium; proteins and phytochemicals [12].
Patients infected with COVID-19 showed higher leukocyte numbers, abnormal respiratory findings, and increased levels of plasma pro-inflammatory cytokines [3].
As much as key molecular mechanisms of the SARS-CoV-2 pathogenesis are still unknown the pathophysiology involves viral entry in respiratory droplets into the lungs via the airways. Due to the two cytokines IL6 and TNF-alpha which interact with the brains hypothalamus resulting in inflammation that causes increased body temperature and fever, whereas the response results in vasodilation and increased vascular permeability, increasing fluid accumulation, causing increased breathing capabilities and consequently difficulties in breathing [14].
The possibility of persistent and recurring infections, especially in immune compromised patients, is unknown; we still have very limited data on the importance of pre-existing morbidities [4]. Respiratory viruses flourish in bodies where the immune system is either still developing or has started to wear out. Reviews comparing the pathophysiology of coronaviruses seems seem to indicate that COVID-19 has the same pathogenic effect as SARS 2003. However, it tends to infect lower parts of the respiratory system, namely bronchioles and alveoli, leading to 15-20% of cases, to have severe pneumonia. It further infects cells by attaching to receptors of Angiotensin converting enzyme–II. The reason COVID-19 is more dangerous has been identified as the lack of memory cells in the immune system to generate adequate and timely immune response to tackle the infection early [15]. It has been suggested that during the response to SARS-CoV-2, the immune dysregulation and the high level of pro-inflammatory cytokines could be the main cause of tissue injury [16].
The person-to-person transmission of COVID-19 infection led to the isolation of patients that were administered a variety of treatments. At present, there are no specific antiviral drugs however, a number of vaccines against COVID-19 infection for potential therapy of humans. The only option available is using broad-spectrum antiviral drugs like Nucleoside analogues and also HIV-protease inhibitors that could attenuate virus infection until the specific antiviral becomes available. The treatments that have so far been attempted showed that 75 patients were administrated existing antiviral drugs [3]. There are no proven or registered therapeutics for COVID-19 infection at this time. Treatment is largely supportive [6].
Currently scientists are testing different treatment regimens to identify the best working medicines in the treatment of COVID-19. Some of the drugs under review include antiviral compounds such as broad spectrum antiviral Remdesivir and Chloroquine as well as broad spectrum antivirals that provide drug treatment options for COVID-19 infection include Lopinavir/Ritonavir, Neuraminidase inhibitors, peptide (EK1), RNA synthesis inhibitors. Despite these, there is need for increased research to identify chemotherapeutic drugs for COVID-19.
Micronutrients have key roles at every stage of the immune response. The schematic in Figure 1 below summarizes important components and processes that are involved in different aspects of the innate and adaptive immune responses. The significant overlap between micronutrients and processes indicates the importance of multiple micronutrients in supporting proper function of the immune system [17]. Marginal deficiencies of micronutrients have been shown to either impair or collectively boost the immune system [17]. Based on various systemic reviews and clinical data, vitamins A, B, C, D, E, Folate, Zinc, Iron, Copper and selenium are important in supporting optimum immune system. Vitamin A is also referred to as anti-inflammatory vitamin and plays a vital role in regulatory of cellular immune processes and humoral immune processes [18]. Vitamin A is important for epithelial cell integrity and immune function of the mucosa. In the presence of controversial ideas between immune system and COVID-19, some scientist and reports suggested that Vitamin C and D, and zinc are some supplements to trigger the immune system and improve the function of white blood cells that fights infection [19].
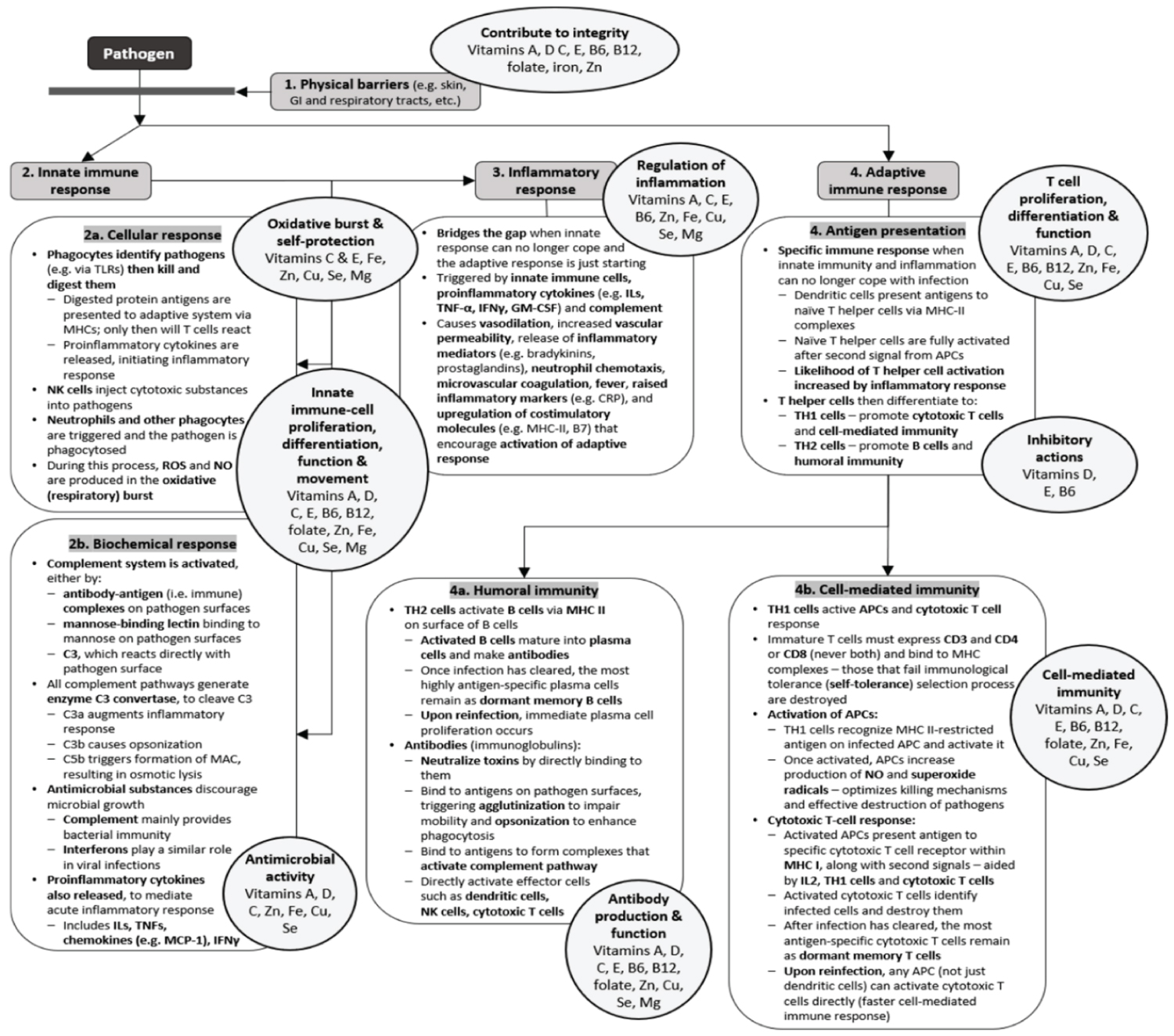 Figure 1: The circles highlight those micronutrients that are known to affect immune responses.
Abbreviations: APCs: Antigen-presenting cells; C3: Complement component 3; CRP: C-reactive protein; Cu: Copper; Fe: Iron; IFNs: Interferons; Igs: Immunoglobulins; ILs: Interleukins; GI: Gastrointestinal; GM-CSF: Granulocyte-macrophage colony stimulating factor; MAC: Membrane attack complex; MCP-1: Monocyte chemoattractant protein-1; Mg: Magnesium; MHCs: Major histocompatibility complexes; NK: Natural killer; NO: Nitric oxide; ROS: Reactive oxygen species; Se: Selenium; TLRs: Toll-like receptors; TNF: Tumor-necrosis factors; Zn: Zinc [17].
View Figure 1
Figure 1: The circles highlight those micronutrients that are known to affect immune responses.
Abbreviations: APCs: Antigen-presenting cells; C3: Complement component 3; CRP: C-reactive protein; Cu: Copper; Fe: Iron; IFNs: Interferons; Igs: Immunoglobulins; ILs: Interleukins; GI: Gastrointestinal; GM-CSF: Granulocyte-macrophage colony stimulating factor; MAC: Membrane attack complex; MCP-1: Monocyte chemoattractant protein-1; Mg: Magnesium; MHCs: Major histocompatibility complexes; NK: Natural killer; NO: Nitric oxide; ROS: Reactive oxygen species; Se: Selenium; TLRs: Toll-like receptors; TNF: Tumor-necrosis factors; Zn: Zinc [17].
View Figure 1
Vitamin C, is an important water-soluble vitamin which acts as a co-factor for several enzymes and an antioxidant which directly scavenges Reactive Oxygen Species (ROS), responsible for most disease conditions. It supports the immune functions and protects against infection caused by a Coronavirus [20]. During the SARS outbreak where no specific treatment had been identified, Vitamin C was suggested as a micronutrient that could have shown non-specific effects on severe viral respiratory tract infections including transformation of lymphocytes and production of interferons [22]. For many years it's been documented that vitamin C has positive impacts on the duration and severity of common cold, attenuating the role of vitamin C in respiratory infections [21]. Three controlled trials with human subjects reported a significantly lower incidence of pneumonia in vitamin C-supplemented groups, suggesting that vitamin C may affect susceptibility to lower respiratory tract infections under certain conditions [21]. COVID-19 had been reported to infect the lower respiratory tract, and vitamin C could be one of the effective alternatives to treat COVID-19 [20,22].
The combined use of vitamin C, hydrocortisone, and thiamine has been found to improve the chest radiologic findings and reduce the mortality of patients with severe pneumonia [23]. During infection, an individual's requirement for vitamin C increases with the severity of the infection. Severe cases of infection may require intravenous administration to compensate for the enhanced turnover of the vitamin [24]. A Randomized Controlled Trial (RCT) carried out in the United States of America involving 167 patients with sepsis-related Acute Respiratory Distress Syndrome (ARDS) indicated that administration of approximately 15 g/day of IV vitamin C for 4 days decreased mortality [25].
So far, there is no known or approved effective pharmaceutical agent against the SARS-CoV-2 virus. Some studies have highlighted the possibility of treating patients infected with the novel SARS-CoV-2 virus with chloroquine and hydroxychloroquine, of which mechanism of action is not completely understood. There is suggestion of reducing the effects of the virus on the affected patients and improving clinical trials outcome through the synergistic action of zinc and chloroquine in patients suffering from the coronavirus disease [26].
Fat soluble Vitamin D is different from others because its synthesized [20] in our bodies with the help UV light from the sunlight for induced conversion of its precursor under the skin [1,6]. Vitamin D is unique because it is also a hormone [20]. Due to its immune modulation role, enhancing innate immunity by upregulating the expression and secretion of antimicrobial peptides therefore its deficiency is likely to affect the immune system and the effect would be reduced mucosal defenses. Low levels of serum vitamin D have been associated with increased risk and severity of viral respiratory infections including community acquired pneumonia and reduced risk with vitamin D supplementation [27].
Furthermore, recent meta-analyses have reported a protective effect of vitamin D supplementation on respiratory tract infections [6] and also lower the immunological sequelae responsible for its fulminant respiratory effects [27]. Populations with limited exposure, e.g. during winter, housebound or institutionalized with limited or no exposure to sunlight are likely to register low levels of vitamin D [28,29]. Vitamin D has been found to have protective effects which may reduce the risk of Covid-19 infection, and also lower the immunological sequelae responsible for its fulminant respiratory effects [27].
In its action vitamin D enhances cellular innate immunity partly through the induction of antimicrobial peptides, and defensins. Vitamin D also enhances cellular immunity, in part by reducing the cytokine storm induced by the innate immune system [30].
It has been proposed that seasonal influenza results from vitamin D deficiency due to lack of exposure to solar radiation, which impairs the innate immune system and triggers viral replication [31]. The innate immune system generates both pro-inflammatory and anti-inflammatory cytokines in response to viral and bacterial infections, as observed in COVID-19 patients [1]. Therefore, vitamin D could work as another therapeutic option for the treatment of this novel virus [20]. Vitamin D has many mechanisms by which reduce the risk of microbial infection and death [1].
There is existing guidance that older adults should supplemented with vitamin D, and there now exists a wealth of evidence which demonstrates the safety of vitamin D3 supplementation at doses of 20-50 micrograms per day. In the face of the Covid-19 pandemic, any effective anti-viral drug therapy to treat those infected, these findings support supplementation of all individuals susceptible to Covid-19 infection, with vitamin D at a minimum daily dose of 20 micrograms per day [32].
Practices like handwashing, vaccinations, social distancing, frequently disinfecting of items and surfaces and isolating help reduce the spread and impact of infectious respiratory diseases. However, additional measures may be necessary. Acute respiratory tract infections were responsible for approximately 2.38 million deaths worldwide in 2016. The current situation with SARS-CoV-2 infection and severe outcomes of COVID-19 and the morbidity and mortality figures make it clear that more strategies need to be taken. New strains of influenza are continuously emerging and can be enormously difficult to contain. As such, additional safe and cost-effective strategies especially among poor populations, are needed to support the immune system, and further protect individuals and populations from harm. Such strategies include provision of sufficient nutritional support for the immune system. The role of nutrition in supporting the immune system has been well-established. Vitamins, for example A, B6, B12, C, D, E, and folate; trace elements like zinc, iron, selenium, magnesium, and copper; and the omega-3 fatty acids eicosapentaenoic acid and docosahexaenoic acid have been found to play important and complementary roles in supporting the immune system [18,33,34].
Not applicable.
Not applicable.
The authors declare that they have no competing interests.
Not applicable.
All authors contributed equally to conduct this review, read, and approved the final manuscript.
Not applicable.