In 2018, the American Academy of Family Physicians (AAFP) published an abridged summary of the 2016 U.S. Preventive Services Task Force (USPSTF) recommendations on Skin Cancer Prevention: Behavioral Counseling. We believe that a contemporary review paper that helps to expand on those recommendations and explain nuanced options for patients and providers is timely and will prove valuable. With the proliferation of skin protection products, scientific studies, and both expert and non-expert advice on social media, our review aims to give a balance of evidence-based recommendations as well as clinical acumen from a team headed by an academic dermatologist with more than 20 years of experience in both the clinical and research settings. This paper aims to serve as a comprehensive and practical guide to sun protection, physical and chemical sunscreens, UV detection stickers, UV-protective clothing, and systemic supplements. We aim to gear it towards the general medical community (as well as to the non-medical layman) without the burden of excessive technicalities.
Skin cancer is the most common malignancy in the U.S.; one in five Americans are predicted to develop skin cancer during their lifetime [1]. Nonmelanoma skin cancers (basal and squamous cell carcinomas) affect more than 3 million Americans a year. Melanoma is predicted to be the fifth most commonly diagnosed cancer in 2022, with almost 200,000 new cases [1]. Contributing factors to skin cancer include excessive sun exposure, use of tanning beds, childhood sunburns, skin that burns easily, red or blonde hair, excessive or atypical moles, and family history [2].
To ensure early skin cancer detection, the American Academy of Dermatology (AAD) recommends monthly self-exams looking for any moles or sores that are significantly growing, changing color or shape, tender, non-healing, or bleeding (Figure 1). Annual visits to a dermatologist for skin checks are recommended, particularly in high-risk populations (history of skin cancer, immunosuppressed, fair skin types, history of childhood sunburns). When detected early, the 5-year survival rate for melanoma is 99 percent [3].
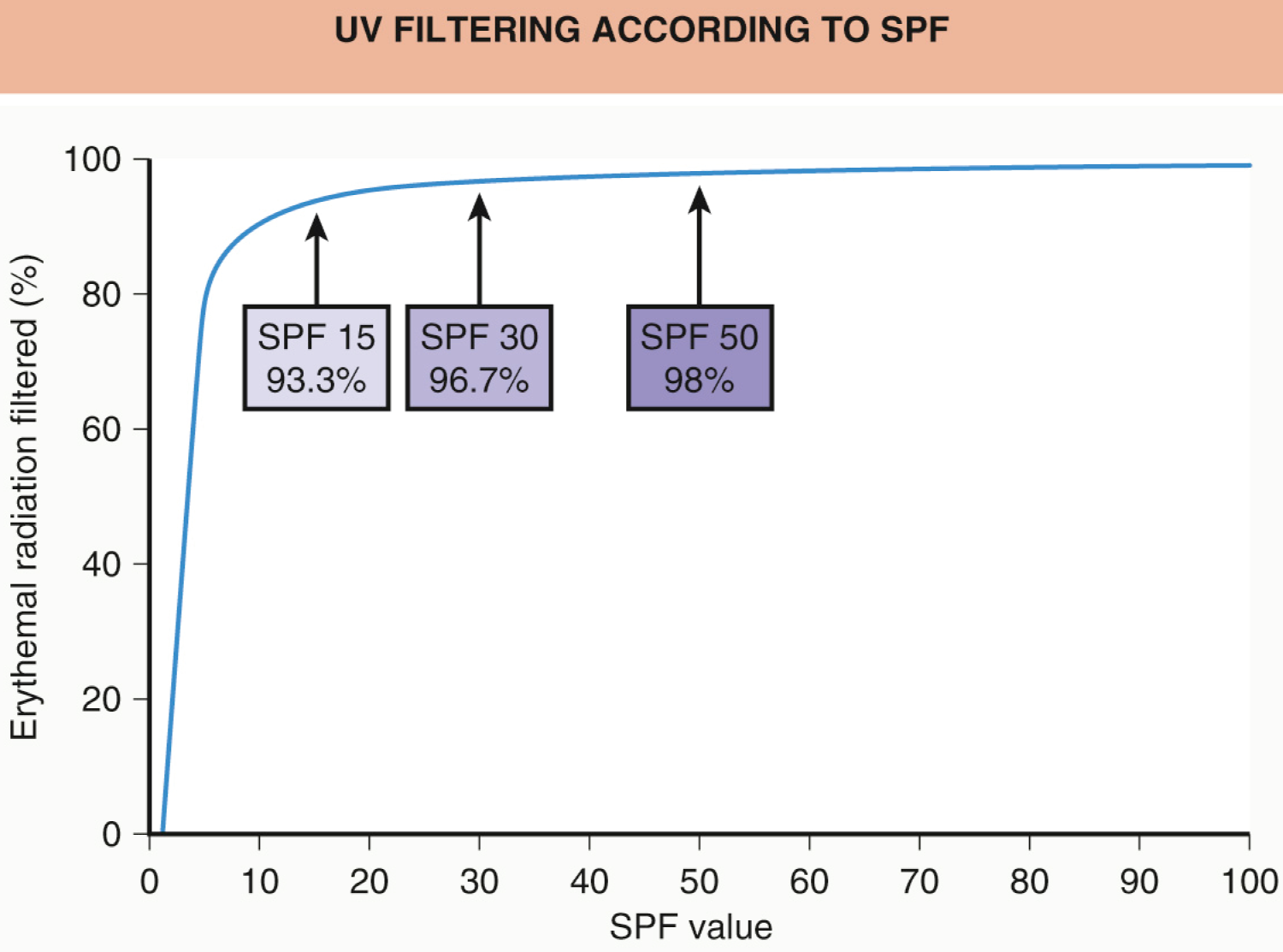 Figure 1: Instructions for monthly skin self-exams, as recommended by the Skin Cancer Foundation.
View Figure 1
Figure 1: Instructions for monthly skin self-exams, as recommended by the Skin Cancer Foundation.
View Figure 1
Sun protection has been emphasized since ancient times. It is well known that excessive sun exposure leads to sunburns, skin cancers, skin damage, and early aging. Despite increased awareness over the past few decades of the damaging effects of sun exposure, there has been little change in positive behavior, with continued sunburns (particularly adolescents), tanning (over 20 million Americans going to tanning salons each year), and even a decline in sunscreen use in some studies [4].
Sunscreens have been proven to decrease rates of skin cancer and photodamage. The efficacy of sunscreen is determined by its sun protective factor (SPF), which is based on the minimal erythema dose (MED), defined as the smallest amount of UV radiation that leads to minimal redness of the skin [3]. Simply put, a sunscreen with an SPF of 15 will allow for an individual to be in the sun 15 times longer before any redness occurs than without any sunscreen at all. The AAD recommends sunscreens with [5]:
1. SPF of at least 30, which blocks 97% of UV rays.
2. "Broad-spectrum" coverage, which protects against both UVA and UVB rays. UVA contributes to early aging and skin damage; UVB is responsible for sunburn. Both cause skin cancers.
3. "Water-resistant" on the label, which allows for maintenance of SPF after 40 to 80 minutes in water.
Sunscreen should be re-applied every two hours. This is particularly important when around sand, snow, and water, as these surfaces reflect UV rays. Even on cloudy days, up to 80% of the sun's rays can penetrate through. Reapplication of sunscreen every two hours, and after swimming or sweating, is recommended [3].
It is important to note that most people only apply 20-50% of the amount of sunscreen needed to achieve the proper amount of SPF on the label [6]. Therefore, liberal application of sunscreen is recommended - when in doubt, use more! One ounce (equivalent to a shot glass) of sunscreen is considered necessary to cover an adult body. Application of two layers or using a sunscreen with double the recommended SPF can help overcome these hurdles.
Sunscreens are categorized into physical and chemical blockers. Physical blockers, containing zinc oxide or titanium dioxide, aim to scatter or reflect UV rays off the skin; they are generally more photoprotective than chemical sunscreens and are better for sensitive skin [7]. Chemical sunscreens absorb UV rays and convert them into harmless, lower-energy wavelengths. They contain more ingredients (oxybenzone, avobenzone, octocrylene, PABA) and have the potential to cause irritation or contact dermatitis but tend to be more cosmetically appealing [8].
Concerns have been raised in recent years about the safety of some ingredients in chemical sunscreens. In 2019, the FDA published a report revealing that four ingredients (oxybenzone, avobenzone, octocrylene, ecamsule) can be absorbed systemically [9]. In 2021, benzene (linked to lymphomas) was found to exist in some aerosolized sunscreen brands, causing them to be recalled [9]. However, a 2020 study in the Journal of the American Medical Association tested six ingredients found in chemical sunscreens and found that while these ingredients were minimally absorbed into the bloodstream, more research was needed to determine if that had any health implications [10]. Simply because an ingredient is absorbed systemically does not automatically render it unsafe. Further studies looking at oxybenzone and octinoxate have not shown any adverse effects of these absorbed compounds on hormone levels, fertility, or development [11].
Studies that suggested a possible link between benzophenone and male infertility as well as oxybenzone in pregnancy being linked to decreased gestational age/low birth weight were limited by confounding factors and high heterogeneity [11,12]. The bottom line is that: 1) Further studies are needed to elucidate any definitive conclusions regarding adverse health effects and 2) The benefits of wearing sunscreen, as proven by studies and clinical trials, far outweigh any theoretical risks. If concerned, patients should talk to their dermatologist to tailor a specific sunscreen for them.
Notably, physical sunscreens pose no such issues of systemic absorption. They have been FDA-labeled as "generally recognized as safe and effective" (GRASE). However, they can leave a chalky white or gray residue on the skin, especially in skin color. Darker-skinned individuals should aim to use micronized sunscreen formulations for a more even spread [13]. They can also benefit from tinted sunscreens, which match skin tone more evenly and provide protection against visible light in addition to UV light. This can prevent solar hyperpigmentation, which affects skin of color disproportionately.
The Fitzpatrick scale describes the ability of an individual to get burnt or tanned after UV radiation exposure (Figure 2). Individuals with Fitzpatrick types I-III (as well as with red or blonde hair) are more likely to burn [3]. Sunburns during childhood and adolescence increase the risk of melanoma [3]. Interestingly, darker-skinned individuals (Fitzpatrick types IV-VI) have a "natural built-in" average SPF of 13.4 due to their increased melanin serving as a UV filter [3]. However, this does not mean they can forego sun protection, as skin cancer can affect any skin color. In fact, certain subtypes of melanomas are more prevalent in darker-skinned individuals and tend to be diagnosed at later, more severe stages.
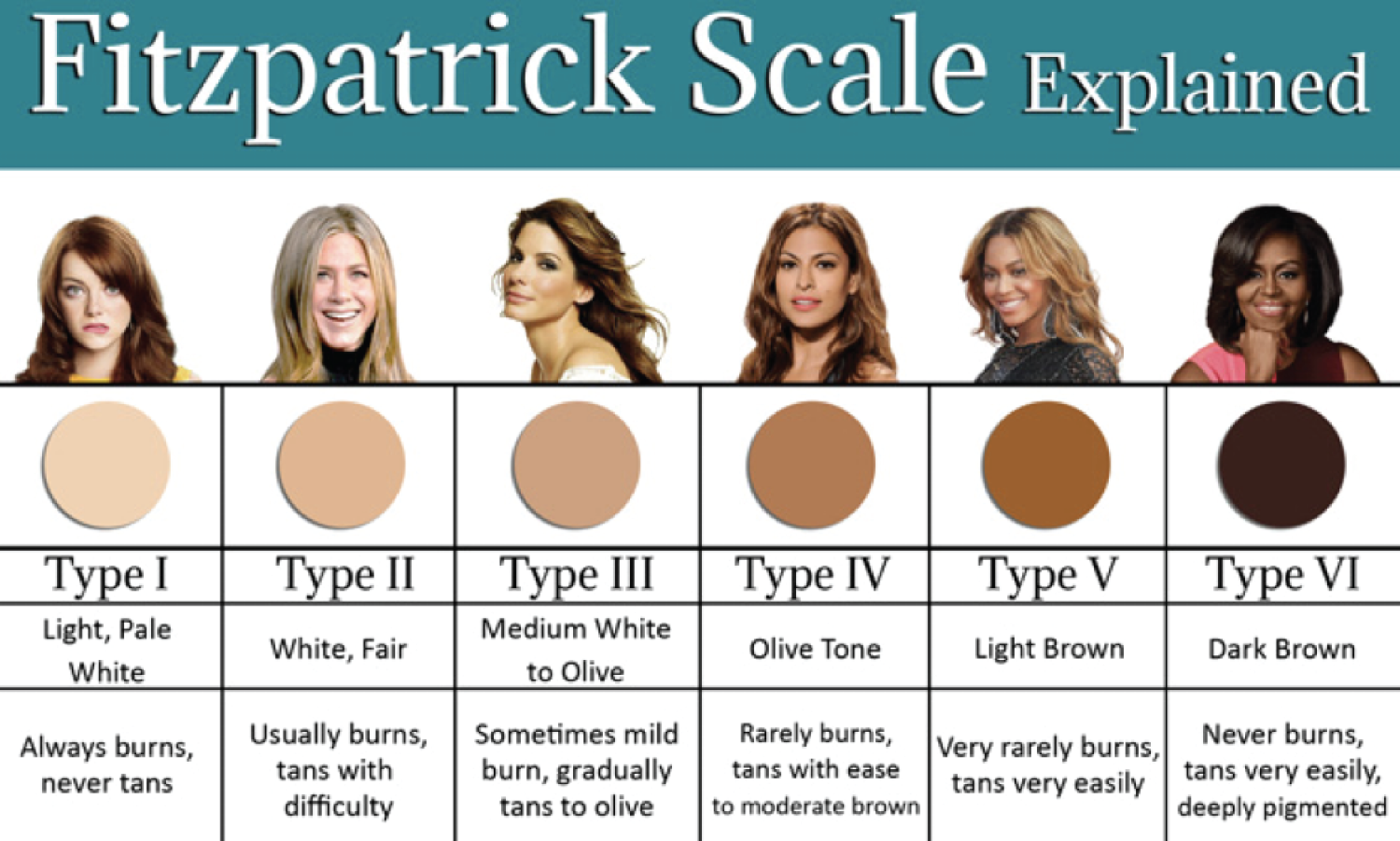 Figure 2: The Fitzpatrick scale, which categorizes individuals on the basis of how easily they tan or burn.
View Figure 2
Figure 2: The Fitzpatrick scale, which categorizes individuals on the basis of how easily they tan or burn.
View Figure 2
Sunscreens come in many different formulations tailored to preference. Creams are preferred for dry skin and the face. Gels are good for hairy areas such as the male chest or scalp. Sticks are useful for around the eyes and lips. Sprays can be convenient for parents to apply onto children, though it can be more difficult to get adequate coverage. It is encouraged to spray until the skin glistens and then rub into the skin evenly. Many moisturizers, foundations, and lip balms contain SPF, adding to convenience. The mantra of the senior author of this paper is that "the best sunscreen is the one that the patient will actually wear."
The AAD recommends minimizing sunscreen use in children under 6 months of age, preferring staying in the shade and covering up (long sleeves, wide-brimmed hat, sunglasses) [5]. However, if the above measures are unavailable, broad-spectrum, water-resistant sunscreen with an SPF of at least 30 can be applied every two hours, as in adults [5]. Physical sunscreens are preferred in order to avoid systemic absorption and irritation to their sensitive, thin skin.
UV detection stickers are adhesives which contain UV-sensitive dyes and photochromic molecules indicating sunscreen efficiency and reapplication time. Examples include Sundicators (Treadley Pty Ltd., Australia), the My UV patch (La Roche-Posay, France), and the SPOTMYUV sticker (Suncayr LTD, Australia). It is recommended to apply the sticker to a sun-exposed area, apply sunscreen over it, then reapply sunscreen to the body when indicated by the sticker changing color (clear to purple with the SPOTMYUV, for example; illustrated in Figure 3) [14]. The color change and toy-like nature may be especially appealing to children. The stickers are reasonably priced, some at less than $1 per sticker. Downsides include lack of adhesiveness to the skin after sweating or if wet.
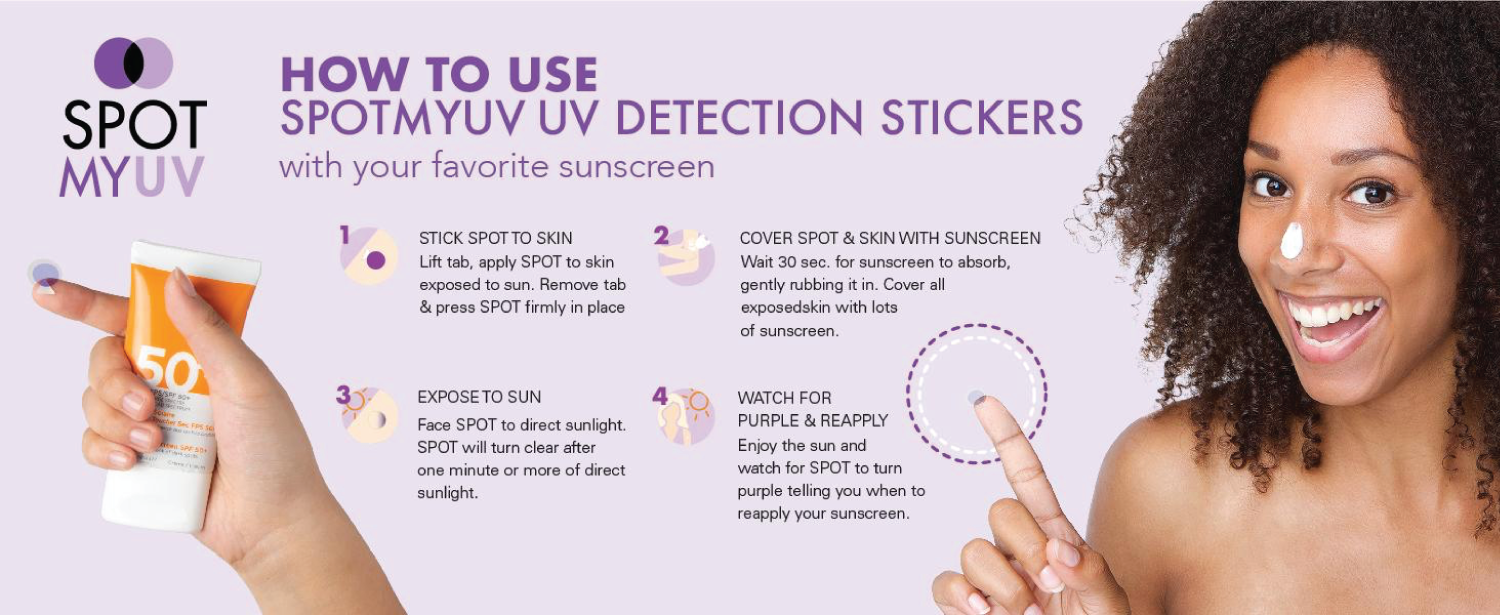 Figure 3: Example and image of a UV-detection sticker.
View Figure 3
Figure 3: Example and image of a UV-detection sticker.
View Figure 3
In a 2019 field study by Hacker, et al. individuals who were given UV detection stickers reapplied sunscreen twice as frequently [15]. Seventy-five percent of participants found the stickers to be helpful, useful, and educational; adherence rates were high (95%).
Wide-brimmed hats (3-inch brim recommended), long sleeves, and UV-protective sunglasses are recommended, especially between the hours of 10 AM to 4 PM (Figure 4) [3]. Thicker clothing with tighter weave fabrics such as denim, canvas, wool, synthetic fibers (Spandex), polyester/cotton, and nylon/elastane, offer greater protection [16,17]. Darker colors and loose fits are more protective. All clothing becomes less photoprotective if wet or stretched. Sun gloves (up to the wrists or forearms) can be useful for UV protection while driving. SunGuard is a laundry aid that adds UPF 30 to clothes for 20 washes.
 Figure 4: AAD recommendations for protective clothing.
View Figure 4
Figure 4: AAD recommendations for protective clothing.
View Figure 4
Clothing has been designed with an ultraviolet protective factor (UPF) up to 50, indicating what fraction of the sun's UV rays (1/50) can penetrate the fabric [16,17]. In contrast, a standard white cotton T-shirt has a UPF of 5. The Skin Cancer Foundation recommends clothing with at least UPF 30 [5]. Brands that specialize in UV-protective clothing as of 2022 include Coolibar, Solbari, Mott50, Lilly Pulitzer, Cabana Life, and Baleaf (Figure 5).
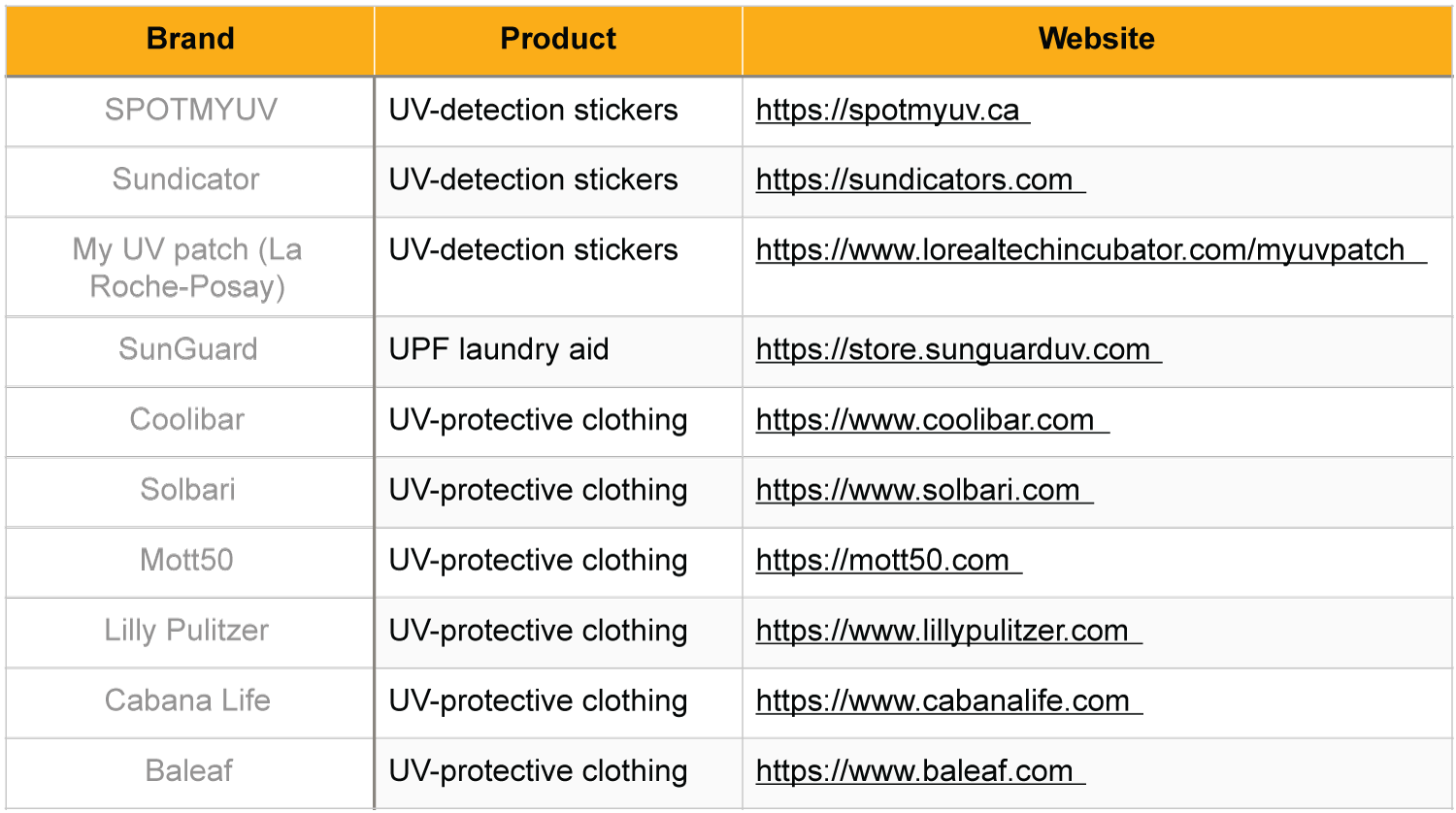 Figure 5: Websites and images for UV-protective clothing brands and UV-detection stickers.
View Figure 5
Figure 5: Websites and images for UV-protective clothing brands and UV-detection stickers.
View Figure 5
Antioxidants (Vitamin C, Vitamin E, selenium, polyphenols) are found in several foods, notably green tea, and have been shown to have photoprotective effects. In a 2021 meta-analysis, Kapoor, et al. found that regular intake of green tea catechins increased minimal erythema dose, preventing redness/sunburns through suppression of reactive oxygen species formation [18]. These compounds also had anti-carcinogenic properties through inhibition of metalloproteinases and leucocyte elastase. Resveratrol, an antioxidant found in grape skin and red wine, has been linked to anti-carcinogenic effects mostly through anti-UVB protection [19]. Niacinamide (or nicotinamide) is the active form of niacin; it has been shown to enhance DNA repair and decrease the formation of cyclobutene pyrimidine dimers in keratinocytes [20]. In one Phase III RCT, niacinamide 500 mg twice daily was associated with a decreased rate of development of actinic keratoses and nonmelanoma skin cancers [20]. However, it has not been shown to increase minimal erythema dose (no redness/sunburn protection). Polypodium leucotomos extract (HelioCare) is derived from a fern native to Central and South America and has been shown to protect against sunburns [20-23]. Many dermatologists recommend these capsules before and during vacations where significant sun exposure will be had.
Other dietary compounds linked to photoprotective effects include flavonoids, carotenoids (carrots, tomatoes), turmeric, pomegranate juice, astaxanthin, Coenzyme Q10 (oily fish, organ meats), and essential Omega-3 fatty acids (fish, flaxseed, chia seeds) [24].
The AAD and Skin Cancer Foundation websites and social media accounts are great resources for further information on sun protection, providing a variety of family-friendly handouts, images, and events.
None.
The authors have no conflict of interest.
The authors declare no funding.