Background: Solid organ transplant (SOT) recipients are more susceptible to infections, particularly Nocardia infections (NI). Our study examines the outcomes associated with NI in SOT recipients.
Methods: Our study used National Inpatient Sample data (2015-Q4 to 2018) and ICD-10 codes to identify patients with NI and SOT. Pearson chi-square test was used to evaluate categorical and continuous variables. Multivariate regression analysis was used to evaluate outcomes using STATA.
Results: Among 621,925 SOT hospitalizations, 734 (0.12%) had NI. Patients with NI were typically older and mostly of white race, with the Southern U.S. having the highest incidence of NI (38.8%). NI increased hospital length of stay (LOS) and costs, and was most prevalent in renal transplant recipients, followed by heart, lung, liver, and pancreas. SOT patients were at a significantly higher risk of developing NI, and co-infection with cytomegalovirus was associated with NI in SOT recipients.
Conclusion: Nocardia is a pathogen known to primarily affect immunocompromised patients. Our study indicates that patients with SOT have a higher odd of developing NI, which translates into longer LOS and higher hospital charges in such patients. Prompt identification with appropriate treatment can help lessen the burden frequently faced by SOT recipients.
Nocardia, Solid organ transplant, Opportunistic infections, Immunosuppression, Clinical outcomes
CCI: Charlson Comorbidity Index; CMV: Cytomegalovirus; ICD-10: International Classification of Diseases, 10th Edition; LOS: Length of Stay; NIS: National Inpatient Sample; NI: Nocardia Infection; SOT: Solid Organ Transplant
Solid organ transplant (SOT) recipients are at an increased risk of a wide range of infections, including nosocomial, opportunistic, and community-acquired [1]. A notable late-stage pathogen is Nocardia, which is rare but life-threatening [1,2]. Nocardia infection (NI) incidence in SOT patients ranges from 0.4-2.65% [3]. While Minero, et al. [4] note that SOT accounts for 25% of NI, there is associated topographical variability. This variability is due to Nocardia’s geographic dependence, as it is predominantly found in dry, arid climates, which aids with aerosolizing spores [5].
The rate of NI also depends on the type of transplanted organ. Several studies have attempted to describe a range of NI in SOT patients. The majority of studies show that lung transplant recipients have the highest incidence of NI [6]. Peleg, et al. [7] noted the frequency of infection with NI to be 3.5%, 2.5%, 1.3%, 0.2%, and 0.1% for transplant recipients of lung, heart, intestine, kidney, and liver, respectively [8].
Current literature identifies various risk factors that increase the prevalence of NI in SOT patients. While immunosuppression reduces the risk of rejection, it makes the recipients more susceptible to NI [9]. Calcineurin inhibitors and prolonged use of steroids are known independent risk factors for NI in SOT patients [7] as Calcineurin-inhibitors suppress T-cell-mediated immunity, which leaves the patient defenseless against NI [10]. CMV infection in the preceding six months also predisposes SOT patients to opportunistic infections such as Nocardia [6].
The data regarding SOT recipients and NI is limited to case studies or studies with decreased statistical power given small sample size, and most of the studies are based on single center experiences. In this study using the data from the National Inpatient Sample (NIS), we sought to better understand the relationship between SOT and NI. With a very large sample size, we explored the recent trends of NI in SOT recipients. In addition, we examined the disease prevalence, effect on length of stay (LOS) in hospital, and risk factors involved in pathogenesis of the disease.
This research adheres to the ethical guidelines of the Declaration of Helsinki. As the study exclusively involved the analysis of de-identified patient data from the National Inpatient Sample (NIS), a publicly accessible database, it did not require review board approval or individual patient consent. The authors confirm their commitment to ethical research conduct, ensuring patient privacy and confidentiality while contributing valuable insights to enhance patient care for solid organ transplant recipients.
The NIS is the largest inpatient discharge database in the US, providing information such as length of stay, severity, procedures, admission and discharge status, without including any patient identifiers. This, in addition to the sheer size of the database (data from over 1000 US hospitals with over 8 million hospital stays per year), makes it ideal to study outcomes [11]. Our study sample was obtained from the NIS 2015 quarter 4 through 2018. We used ICD-10 codes to identify and extract patients who underwent SOT procedures, such as heart, lung, kidney, liver, pancreas, and intestine. We further isolated patients from these subgroups diagnosed with a NI and compared them to those who did not have NI infections.
We utilized Pearson chi-square test for evaluating categorical and continuous variables. In addition, we applied multivariate regression analysis to compare groups of interest and further controlled for all variables such as age, gender, race, Charlson Comorbidity Index (CCI), median income based on zip code, type of insurance, and CMV co-infection. All samples represented in this study were weighted using an algorithm provided by the NIS, allowing for an accurate national estimate of cases of interest. All extractions and statistical analysis were conducted utilizing Stata version 17.0 (StataCorp).
We identified 621,925 SOT hospitalizations, among which 734 (0.12%) had NI. Patients with SOT and NI were older compared to the non-NI cohort (mean age 61.3 +/- 10.9 vs. 56.1 +/- 17.2; p < 0.001); however, both SOT with and without NI were majority white (Table 1). The highest incidence of NI in SOT patients in the US occurred in the South (38.8%), followed by the West (26.5%), Midwest (17.7 %), and Northeast (17.0%) (Table 1). There were no significant differences in baseline CCI between the two cohorts (3.62 vs. 3.73; p = 0.40) (Table 1). Hospitalizations with SOT and NI had longer LOS [adjusted mean difference (aMD) 5.7 days] and higher hospital charges adjusted for inflation over time (aMD $66,348); all p < 0.01.
Table 1: Baseline characteristics of solid organ transplant hospitalizations in the national inpatient sample (2015 Q4-2018) stratified by Nocardia Infection. View Table 1
Moreover, hospitalizations with SOT had higher odds of developing NI compared to those without SOT [adjusted odds ratio (aOR) 13.1; 95% CI 10.0-17.1; p < 0.001]. NI was most prevalent in renal transplant (53.1%), followed by heart transplant (23.8%), lung transplant (12.9%), liver transplant (8.2%), and pancreas transplant (2%) recipients (p < 0.001) (Figure 1).
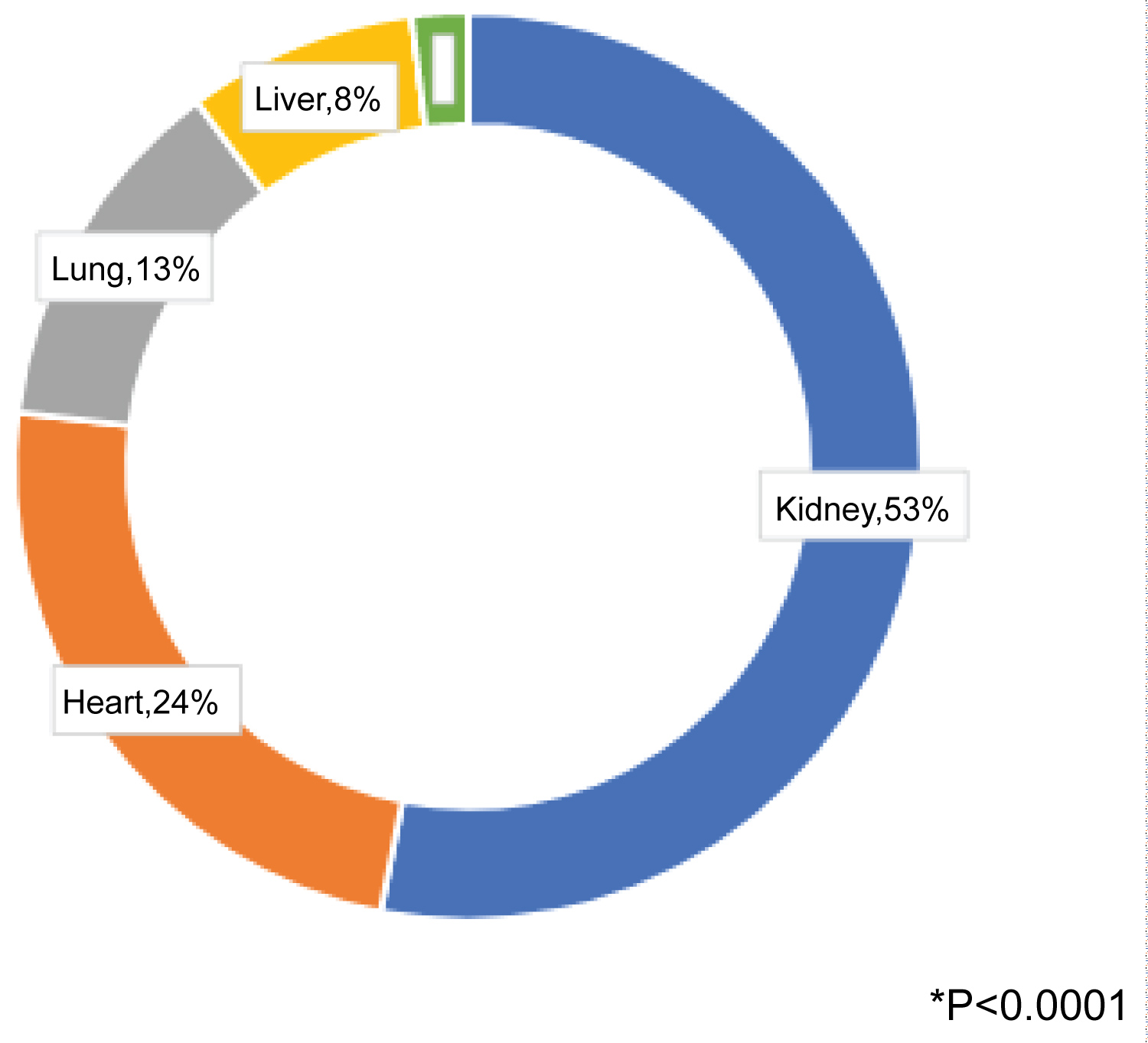 Figure 1: Proportion of Nocardia in solid organ transplant recipients* .
View Figure 1
Figure 1: Proportion of Nocardia in solid organ transplant recipients* .
View Figure 1
Our findings show that compared to SOT hospitalizations without NI, SOT hospitalizations with NI were in older patients, had longer LOS, and had higher hospital charges. In addition, Nocardia was most prevalent in renal transplants, followed by heart, lung, liver, and pancreas. We also found that hospitalizations with SOT had higher odds of developing Nocardia than hospitalizations without SOT. Regionally, the highest incidence of NI occurred in the South, followed by the West, Midwest, and Northeast. We also found a correlation between CMV co-infection and NI in SOT.
Our study demonstrates that the hospitalizations with SOT and NI were older (specifically > 60 years) than the non-NI cohort. Also, hospitalizations with NI and SOT had longer LOS and higher hospital charges. Previous studies have identified old age as a potential risk factor for Nocardia infection in SOT recipients [3]. Our study, in line with the literature, finds that the older population is more susceptible to developing Nocardia infections. Risk factors predisposing NI among SOT recipients include diabetes, high-dose steroids, obstructive pulmonary disease, and alcoholism [12,13]. The older population has increased comorbidities such as diabetes and pulmonary disease [14], which increases the risk for NI. Coussement, et al. [2] found that Nocardia developed in SOT patients with longer LOS (> 8 days) in the ICU compared to patients with shorter LOS (< 8 days) alluding to the opportunistic nature of Nocardia. Due to variations in the post-operative course of SOT patients and increased immunosuppression, NI prolongs a patient’s LOS and explains higher medical charges.
Contrary to pre-existing literature, our study finds that NI is most prevalent in renal transplant patients. Previous data have shown lung transplants to have the highest incidence of NI, followed by heart, with the kidney having a much lower prevalence [15]. The difference could be due to several reasons. First, there have been no updated multicenter analyses regarding the prevalence of Nocardia [3] since 2013. Most of the other data was derived from single organ transplant centers, some from multi-organ centers, and even fewer looking at the nationwide data. Second, kidneys have been the most prevalent organ transplant in the US for the past two decades. In 2018, kidneys accounted for the majority of all organ transplants in the US, with a total of over 20,000 total transplants [16,17]. Therefore, our results from the NIS could skew toward kidneys simply due to the increased number of kidney transplants that have occurred in the recent years.
Our study also revealed that hospitalizations with SOT were associated with higher odds of developing NI than those without SOT. These results align with the current literature, which suggests that NI is primarily observed in immunocompromised patients who lack cell-mediated immunity [18]. The higher odds of NI in SOT patients can be attributed to using tacrolimus, a commonly used immunosuppressant known to increase the risk of NI by suppressing T cell mediated immunity [18,19]. Furthermore, NI transplants are increasingly prevalent in the last two decades, possibly due to the development of improved detection methods and the growing number of transplant patients [16,20]. Thus, this trend may further explain the increased odds of NI observed in SOT patients.
In our study, we found that the highest incidence of NI is in the Southern US, followed by the West, Midwest, and finally, the Northeast. Literature supports these findings, showing the highest prevalence of NI in the Southwest region [3]. This geographic preference is due to the dry, windy climate supporting the aerosolization of the bacteria. The challenge with identifying the prevalence of Nocardia in different geographic regions is the use of multi-variant tools for the diagnosis of the pathogen. Older studies looked at biochemical tests to identify NI, whereas newer studies rely on molecular tests [21]. Our study looks at a specific time frame throughout the nation and hence sheds more reliability in identifying prevalence patterns within the country.
Our study identifies a high incidence of CMV co-infection with NI in SOT hospitalizations, which is consistent with previous case studies that have associated CMV and Nocardia co-infection in renal transplant patients [18,22]. The literature on the relationship between CMV and Nocardia in SOT patients is inconsistent. While some studies suggest that CMV infection before transplantation increases the risk of Nocardia infection [7], others indicate no correlation between CMV serostatus, illness, or disease and Nocardia [2]. The reasons for this inconsistency are likely multifactorial. Firstly, immunosuppression in transplant patients, including using medications such as tacrolimus, can suppress T cell mediated immunity and increase susceptibility to both CMV and Nocardia infections [23]. Secondly, transplant-related procedures or donor-derived infections can also increase the likelihood of both CMV and Nocardia infections in transplant patients [23,24]. Thirdly, bone marrow suppression with leukopenia and acute kidney injury can occur during the post-transplant course, making it difficult to use prophylactic antibiotics, such as sulfa-trimethoprim and valganciclovir, leading to increased opportunistic infections [23]. Finally, the symptoms of CMV and Nocardia infections can overlap [8] or be masked in an array of noninfectious fever etiologies, making it difficult to distinguish and identify between the two infections. This can lead to delayed diagnosis and treatment, increasing co-infection risk and potentially more severe outcomes.
A notable strength of this paper is that this is the only study looking at a national database for associations of NI with SOT and various risk factors. However, the study is not without its limitations. The NIS is an administrative dataset prone to coding errors and over calculation of encounters due to possible multiple admissions of the same patient. Due to the nature of the dataset, it is also difficult to track patient encounters longitudinally. Furthermore, certain information such as lab values and specific medication regimens being administered to the patient population are not included. To mitigate these limiting factors, it would be advantageous to conduct further studies and stratify the data, including variables that are not present in the NIS. Still, the NIS is one of the largest publicly available databases in the US and can be useful in the study of rare diseases such as NI in SOT.
In conclusion, we found the highest prevalence of NI in renal transplant patients, with increased odds of NI, LOS, and hospital charges. With rising SOT cases and even higher susceptibility to life-threatening Nocardiosis in SOT patients, closer monitoring is important in this population for early recognition and intervention to avoid major complications from NI. Further studies using large-scale data are also warranted to provide more reliable information about the epidemiology of NI and management strategies to prevent and treat NI.
The authors of this research paper, Rezwan Munshi, Narois Nehru, Madison Lannom, James R. Pellegrini Jr, Ngoc-Van Tran, and Fatima Anjum, declare that they have no conflicts of interest to disclose. This research was conducted in an unbiased manner, and the authors did not receive any financial or non-financial support that could potentially influence the results or interpretation of the findings presented in this paper.
This research received no specific grant from any funding agency, commercial entity, or governmental organization. The authors conducted this study independently without external financial support.
The authors, Rezwan Munshi, Narois Nehru, Madison Lannom, James R. Pellegrini Jr, Ngoc-Van Tran, and Fatima Anjum, declare that they have no financial interests or relationships with any commercial entities that could be construed as a potential source of bias or conflict of interest regarding this research. All authors have contributed to this research without any external financial incentives or competing financial interests.
Rezwan Munshi, MD: Conceptualization, Methodology, Data Analysis, Writing- Original Draft Preparation, Supervision, Project Administration; Narois Nehru, MD: Writing- Review & Editing; Madison Lannom, MD: Writing- Review & Editing; James R. Pellegrini Jr, MD: Data Analysis, Writing- Review & Editing; Ngoc-Van Tran, MD: Writing- Review & Editing; Fatima Anjum, MD: Writing- Review & Editing, Supervision.