Bartonellosis or Cat Scratch Disease (CSD) is defined as an infectious, benign illness that in most cases results from the scratching, licking or biting of animals carrying the bacterium Bartonella henselae. This study aims at describing the epidemiological profile of serologically reactive samples between the years 2011 and December 2017 in Brazil. Official data from the requests for diagnostic tests registered in GAL (Gerenciador de Ambiente Laboratorial/Laboratory Environment Manager) in the Ministry of Health of Brazil were analyzed. The reactive samples were selected by their place of occurrence, date and demographic profile. The results showed that the Brazilian states with the highest incidence of reactive samples were respectively Rio de Janeiro 31.04% (149/480) and Minas Gerais 29.37% (141/480). The year with the highest number of reactive samples was 2017, with 47.29%, (227/480). Regarding the demographic indicators, the urban environment outstand itself with the highest number of incidents, 33.33% (160/480). It's noticed a balanced incidence among males 52.91%, (254/480) and females 47.08% (226/480). About race/color, most were white 18.54%, (89/480). The most incident age group was 0 to 10 years 40.00% (192/480). We point out in this study that although bartonellosis is a well-known disease, there is still a shortage of papers describing the distribution of the disease in Brazil, so it is necessary to carry out more investigative studies, in order to better clarify the epidemiological profile of the cases and thus to assist health services in the early diagnosis, treatment and decision-making.
Bartonellosis, Cat scratch disease, Epidemiological profile
The disease popularly known as "Cat Scratch Disease" (CSD) or Bartonellosis, is defined as an infectious and benign illness that in most cases results from the scratching, licking or biting of animals carrying the bacterium Bartonella henselae [1]. The etiological agent of the disease is a bacterium belonging to the bartonellaceae family, of which, almost 50 species have been identified, and 15 of them are pathogenic to humans [2].
Bartonellosis may present in its clinical picture; fever, headache, weakness and inappetence [3]. The disease rarely progress to visceral, ocular and neurological impairment [4]. It is estimated that the incidence is approximately ten cases per 100,000 inhabitants per year in the United States, but in Brazil, there is little available data on the occurrence of cases at the population level [5].
The diagnosis of Bartonellosis can be obtained through serological methods (immunofluorescence and enzyme immunoassay), molecular and isolation [6]. Antibodies directed against B. henselae are detected in serum by plasma or cerebrospinal fluid from infected patients. For this, indirect immunofluorescence (IFI) or immunoenzymatic assays are used, using specific antigens [7].
In Brazil few cases of the disease have been described and their magnitude is underestimated [8-15]. Based on the above, this study aims to delineate the epidemiological aspects of the reactive samples for bartonellosis in the Brazilian states, regarding place of occurrence, date and demographic profile.
This study quantitatively analyzes the distribution of bartonellosis reactive samples in humans by place of occurrence, date and demographic profile between January 2011 and December 2017 in Brazil. For its accomplishment, official data of the biological materials registered in the Laboratory Environment Manager System-GAL of the Ministry of Health, were used. GAL is the information system used by the Brazilian Ministry of Health for the laboratory routines.
The analysis considered data on serology requests made through Indirect Immunofluorescence Reaction. This assay is intended for qualitative or semi-quantitative determination of human IgG class antibodies against Bartonella henselae. The detection of anti-Bartonella immunoglobulin G (IgG) antibodies was performed by a test produced by the manufacturer Scimedx/Medivax®, with titration cut-off values greater than 1/64.
This study considered the following variables: Place of occurrence (State and municipality of residence). Date of occurrence (date of request). Demographic data (Sex, Age, Race/Color and Occurrence Zone).
A distribution map made with the Tabwin 32 program, tables and graphs generated in Microsoft Excel 2007 software were made from the results. The results were presented by descriptive statistics and shown by means of absolute and relative frequency.
It should be noted that we used secondary data, presented in a database that did not contain nominal information or that could identify individuals. Thus, the appreciation of this study to the ethics committee was dispensable.
A total of 1265 samples were analyzed in the period, of which 61.42% (777/1265) were non-reactive, 37.94% (480/1265) were reactive for anti-Bartonella henselae antibodies, 0.55% (7/1265) presented inconclusive results and 0.07% (1/1265) was not tested. The annual distribution of reactive samples can be seen in Figure 1A. Regarding the monthly average frequency, it was observed that there was an equilibrium in the distribution of reactive samples with a slight increase in the months of September and October (Figure 1B).
 Figure 1: Seasonality of reactive samples for bartonellosis from the biological materials registered in the Laboratory Environment Manager System - GAL of the Ministry of Health of Brazil. A) Number of reactive samples for bartonellosis according to the year of collection of the biological material. Brazil, January 2011 to December 2017; B) Monthly distribution of reactive samples for bartonellosis in Brazil, 2011 to 2017. View Figure 1
Figure 1: Seasonality of reactive samples for bartonellosis from the biological materials registered in the Laboratory Environment Manager System - GAL of the Ministry of Health of Brazil. A) Number of reactive samples for bartonellosis according to the year of collection of the biological material. Brazil, January 2011 to December 2017; B) Monthly distribution of reactive samples for bartonellosis in Brazil, 2011 to 2017. View Figure 1
In relation to the states, or Federated Units (FU) and the region of the occurrence of the reactive samples, it is observed that the Southeast region 85.42% (410/480) and the FUs, Rio de Janeiro 31.04% (149/480) and Minas Gerais 29.38% (141/480) presented the highest prevalences. Absolute and relative frequencies according to the Brazilian regions and the FU are presented in Table 1. The distribution of the reactive samples according to the patients' municipality of residence is shown in Figure 2.
Table 1: Distribution of reactive samples for bartonellosis, according to Federated Units and regions of Brazil. View Table 1
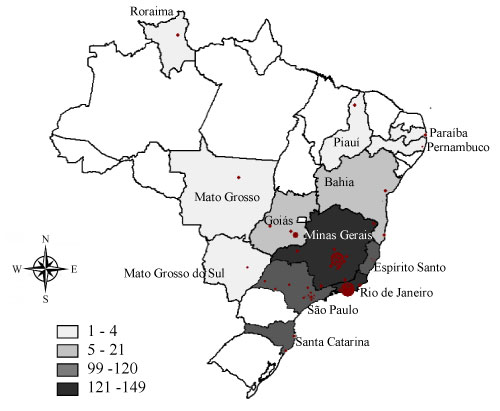 Figure 2: Spatial distribution of reactive samples for bartonellosis, according to the Federated Units and the municipalities of residence in Brazil, 2011 to 2017. View Figure 2
Figure 2: Spatial distribution of reactive samples for bartonellosis, according to the Federated Units and the municipalities of residence in Brazil, 2011 to 2017. View Figure 2
Regarding the demographic profile of the reactive individuals, more specifically in relation to color/race, gender, age group and zone of residence, it is possible to observe the absolute and relative frequencies of the reactive samples in Table 2.
Table 2: Demographic profile of reactive samples for bartonellosis in Brazil from 2011 to 2017. View Table 2
It is possible to observe an increase of reactive samples for bartonellosis in Brazil during the historic serie evaluated. The seasonality of the reactive samples was more frequent in the months of September and October. During the same period, cases of spotted fever occur in Brazil and many bartonellosis tests are requested as a differential diagnosis of spotted fever [16]. Animal contact and the presence of a febrile clinical picture motivate the investigation of both diseases.
The Southeastern region of Brazil was highlighted with the states (Or FU) of Rio de Janeiro and Minas Gerais, with a higher frequency of reactive samples. About the municipalities, it is noticed that the highest frequency occurred in the capitals of these states, which is a justifiable fact, given the greater population density in these municipalities and because they host the reference laboratories for the Brazilian Ministry of Health [17]. Molecular diagnosis is also available in the network of public health laboratories in Brazil. However, as its use is recent in the country, this information will be discussed at another time.
Regarding the zone of residence, we verified a higher frequency of individuals living in urban areas. However, this information should be better evaluated, since the requests for laboratory diagnoses do not have information on the probable site of infection, only if the individual is a resident of an urban or rural area.
In Brazil, bartonellosis is not a notifiable disease for health services, so many cases are not investigated by epidemiological surveillance services and the site of infection is not identified [18].
Regarding the other demographic aspects, the highest frequency of positive samples among children from 0 to 10-years-old, is highlighted. A justification for this information would be that children in this age group are more exposed to the reservoir animals and as the age advances, a lower frequency of reactive samples is noticed [6,19]. Men and women present similar proportions of reactive samples and the white race was also the most prevalent. Our results are in line with other studies conducted in Brazil [8,12,13,15].
Lamas, et al. [8] verified prevalences varying from 12 to 41% with an epidemiological profile like the one presented here. Pitassi, et al. [13] evaluated the prevalence among blood donors in 500 blood donors from Campinas, Brazil. Antibodies against B. henselae were found in 16% of blood donors. These same authors verified that Bartonella DNA was present in the bloodstream of approximately one out of thirty donors from a major blood bank in South America. The bloodstream infection with B. henselae or B. clarridgeiae was associated with cat contact or history of tick bite. These risk factors should be considered during donor screening, as bacteremia by these Bartonella species may not be detected by traditional laboratory screening methods, and it may be transmitted by blood transfusion [15].
It should be noted that there are currently no official protocols within the scope of the Brazilian Ministry of Health, with information on the conduct of epidemiological surveillance, diagnosis and treatment of cases of bartonellosis. For this reason, it is likely that the data presented here are underestimated. In addition, the number of unavailable information (not informed) in the forms of request for laboratory diagnosis makes our analysis partially impaired. Our results are limited by the lack of information on the demographic profile of the individuals.
Even with the restrictions from the bartonellosis laboratory diagnosis requests, it was possible to delineate the epidemiological aspects related for Bartonella henselae in Brazil, based on the locality, date and demographic profile of the reactive samples.
It is hoped that the information presented in this study can contribute to the current knowledge on the distribution of bartonellosis infections and that it stimulates and directs more investigative research in order to assist the health services in the early diagnosis, treatment and decision making.
The author declares that there is no conflict of interest regarding the publication of this article.