To reduce coronary artery bypass graft (CABG) deep incisional and organ/space surgical site infection (SSI) incidences we established consistent use of SSI prevention bundle elements, education, and audits. These practices have helped us reduce and maintain zero CABG SSI incidences from October 2016-July 2021 at our hospital.
Surgical site infections (SSI) are a substantial cause of morbidity, prolonged hospitalization, re-admissions, and even death [1]. In 2017, it was approximated that 160,000 to 300,000 SSI incidences occurred in the United States; half of which the Centers for Disease Control and Prevention (CDC) deemed preventable using evidence-based strategies [2,3].
Coronary artery bypass graft (CABG) procedures are one example of an operation susceptible to SSI incidences. CABG surgeries are conducted to improve poor blood flow to the heart by taking a healthy blood vessel from the leg, arm, or chest and connecting it below or above the blocked arteries in the heart [4]. There are two types of CABG procedures, those with both chest and donor site incisions (CBGB) and those with only a chest incision (CBGC).The purpose of this quality improvement project is to describe our experience achieving zero CBGB and CBGC deep incisional and organ/space SSI incidences from October 2016-July 2021.
To prevent CABG deep incisional and organ/space SSI incidences our Infection Prevention and Epidemiology Department along with the Cardiothoracic and Vascular Surgery Department established SSI prevention bundle elements, continuous education, and monthly audits.
SSI prevention bundle elements are pre-operative, peri-operative, and post-operative steps that are required to achieve best results. We follow the CDC's SSI prevention bundle checklist recommendations. Pre-operative bundle elements include Methicillin-resistant Staphylococcus aureus (MRSA) screening and nasal decolonization. Antiseptic prophylaxis via CHG soap or wipes are used for bathing the night before or morning of the procedure, antimicrobial prophylaxis is administered one to two hours before surgery, the patient's hair is removed using clippers, and skin is further prepped with a CHG scrub. Glycaemic, normothermia, and oxygenation levels are monitored peri-operatively and post-operatively. Wound care with dressing changes at least every 24 hours is conducted, and antibiotics are typically administered for up to 24 hours after surgery.
Computer-based education on SSI prevention is completed upon hire for new employees then annually. There is also a Nurse Educator that reminds employees of infection prevention importance and procedures; scrubbing instead of painting CHG on a patient is especially focused on.
Additionally, monthly multidisciplinary workgroup meetings are conducted that consist of an Infection Preventionist, Surgeon Champion, Peri-op Manager, Certified Nurse Specialist, Nurse Educator, Performance Improvement Specialists, and Information Technology Specialist. Together we assess which SSI prevention elements are in place and determine which bundle elements are in alignment with evidence-based national guidelines. These meetings reinforce the importance of infection prevention in surgical procedures and give team members the opportunity to discuss any concerns while also learning from each other as everyone brings different expertise to the group.
Our infection prevention team conducts monthly audits on each CABG SSI prevention bundle element through electronic medical record reviews, direct observation, and interviewing caregivers. The operating rooms where CABG procedures take place are routinely rounded on in depth as part of the environment of care annual audits. During that investigation, the Joint Commission guidelines on factors such as environmental management and disinfection, sharps safety, hand hygiene, instrument inspection, personal protective equipment, positive air pressure, and limited room traffic are all evaluated for compliance. Each infection prevention item is marked as either compliant or non-compliant and total led at the end to determine a facilities compliance score. The completed checklist with comments on findings and recommendations is sent to the manager of the department and a follow up evaluation is scheduled to determine progress.
From quarter one of 2015 through quarter three of 2016 there were 317 CABG procedures, three of which developed into deep incisional or organ/space SSI cases. From quarter four of 2016 through quarter two of 2021 there have been 625 procedures, zero of which developed into CABG deep incisional or organ/space SSI incidences. See Figure 1 for the corresponding CABG SSI standardized infection ratio (SIR) by quarter.
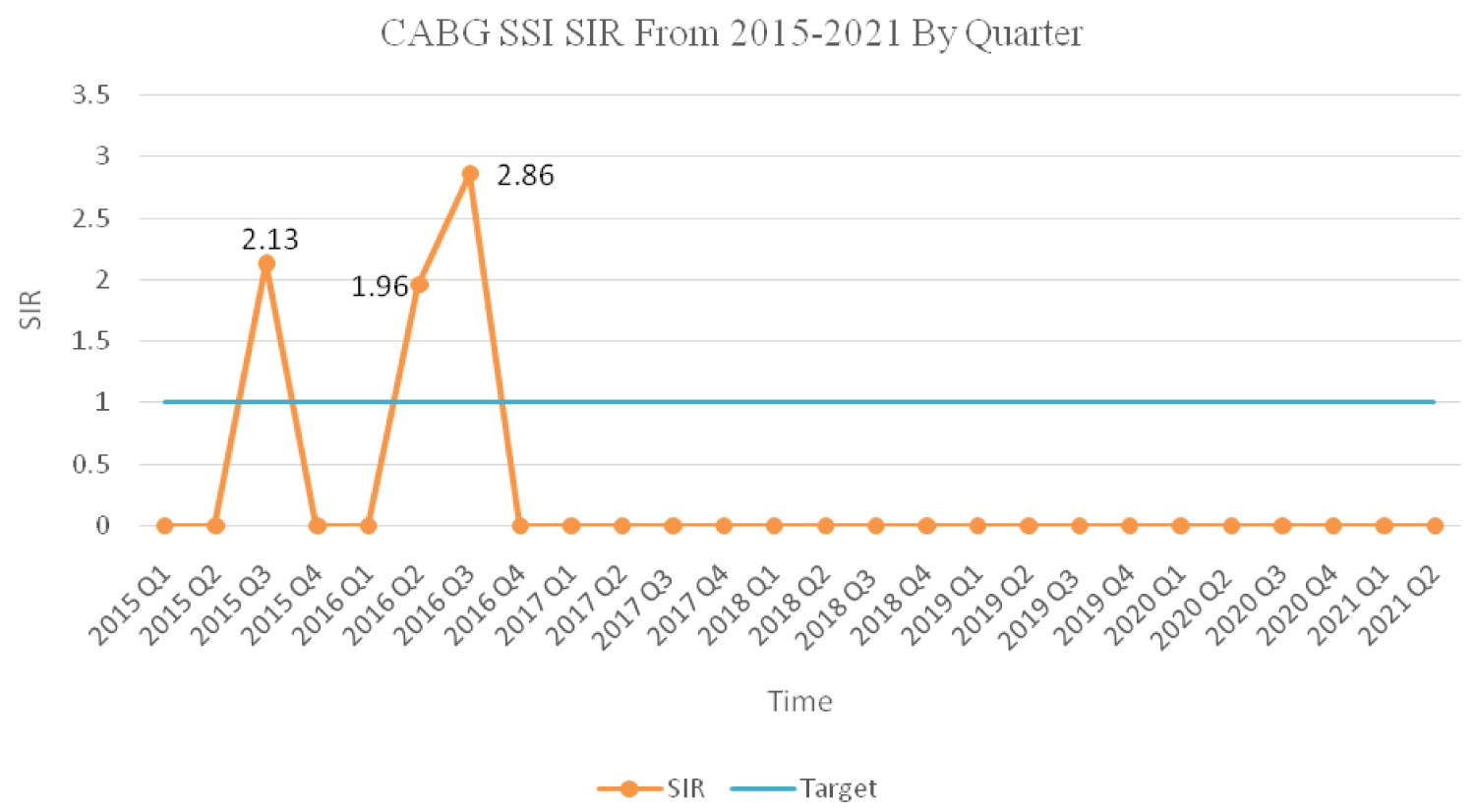 Figure 1: Coronary Artery Bypass Graft Surgical Site Infections by Quarter from 2015 to 2021.
Figure 1: Coronary Artery Bypass Graft Surgical Site Infections by Quarter from 2015 to 2021.
In mid-2015 through the end of 2016 our hospital had higher than predicted CABG SSI incidences. Upon implementing CABG SSI prevention bundle elements, education, and audits our infections dropped and sustained at zero.
View Figure 1
CABG SSI prevention bundle element compliance on 275 procedures from December 2018-July 2021 were audited. Pre-operatively, CHG scrubbing was 98.4% compliant, CHG bathing was 88.2%, antibiotics were 93.5%, and hair removal was 99.6% compliant. MRSA screening was 97.2% compliant and post-operative normothermia was 96.3% compliant. In 2020, audits from the operating rooms discovered 65 out of 69 (94%) environment of care checklist items to be compliant.
Our results show overall improvements in our quarterly CABG SSI SIR from quarter one of 2015 to quarter two of 2021. Initially two small spikes in CABG SSI incidences occurred however by quarter four of 2016 the CABG SIR decreased to zero. This period of no CABG SSI incidences has been maintained for the following 57 months.
From the most recent audits on our SSI bundle compliance and operating room we have concluded that infection prevention measures are being met for CABG procedures. Overall SSI bundle element compliance is relatively high with an average of 83% from December 2018-July 2021. Bundle element compliance was not recorded from March-May 2020 due to limited CABG procedures as a result of the COVID-19 pandemic. Operating rooms were found to be highly compliant. There was some dust and tape residue, but this was quickly resolved upon receiving feedback. All other checklist items for compliance were met.
This experience demonstrates the importance of complying to SSI prevention bundle elements, education, and auditing in reducing and maintaining zero CABG deep incisional and organ/space incidences for over four years. Additional research is needed to determine the effectiveness of each individual bundle element in CABG SSI prevention.