Malaria is a global public health problem with many cases each year in the world (241 million cases with 247,000 deaths (67% were under five children) in 2020. Most malaria cases occur in Sub-Saharan African countries (93%).
The objective of our study was to observe how is implemented ITN policies against malaria with a view on socio-economic factors, in Senegal, which is country close to malaria elimination.
Data used for analysis is from Demographics and Health Surveys 2019 for Senegal. Linear regression models were performed with an estimation of the mean number of persons using ITNs among groups (urban or rural areas, wealth level, highest education level in the household and age of household head) in each country. We evaluated the importance of co-factors in the relationship between the number of ITNs (insecticide-treated nets) in a household and the number of household members by calculating the R-squared.
Senegal has 58.7%) of households in which all children under 5 sleep under ITNs. We found R-squared (R2 = 0.36) for the relationship between the number of ITNs in a household and household size. When wealth level, age of head of household, area of residence (rural or urban), education level in the household and number of bedrooms in the household were controlled for, we found R2 = 0.38.
We found that Senegal's national malaria program is decentralized with entomological monitoring in all districts, which is normal considering the intervention stage in the fight against malaria.
Our study present ITN health policies (possession and use) according some socio-economic factors in Senegal, which has succeeded in maintaining low malaria prevalence (in Senegal). Being close to elimination, Senegal required more active malaria surveillance than passive surveillance. These results merit a review in the context of each African country.
Malaria, National malaria programs, Health policies, Linear regression
GDPs: Gross Domestic Products; ITNs: Insecticide-Treated Net
Malaria is a global public health problem with many cases each year in the world (241 million cases with 247,000 deaths (67% were under five children) in 2020. Most malaria cases occur in Sub-Saharan African countries (93%). The prevalence of malaria in some Sub-Saharan African countries is very high. While almost all African countries have set up a national program to fight malaria with grants from international organizations, local governments, and private funds, they have not made the same progress or used the same methods in the elimination of malaria, producing tailored intervention by countries [1,2].
Senegal is a West African country, which has gross domestic products (GDP) of around 20 billion United States Dollars. Yearly minimum and maximum temperature in Senegal are (24.5 ℃ and 32.3 ℃). Yearly minimum and maximum rainfall in millimeter are (0.18 mm and 261.36 mm). Senegal is close to malaria elimination while Burkina Faso is not. The national malaria program of Senegal has been very successful. Senegal has maintained low malaria prevalence for several years [3,4].
Several studies have found that the risk of malaria infection is influenced by climate (such as quantity of rainfall or air temperature) and by socio-economic factors (such as the economic status or education level of a family) which can influence some behaviors such as the use of nets [5-7].
According to operational requirements for malaria elimination outlined by the World Health Organization, countries that are close to malaria elimination, strengthening of health systems with early detection and early treatment of malaria cases is critical in achieving malaria elimination [8].
Malaria is one of the major public health problems in Africa, with most cases and mortalities occurring among African children. Health policies in the fight against malaria have been implemented in Senegal, with good results. Studies have shown the importance of considering parameters such as funding, malaria case management, health information systems, collection of routine data for surveillance and other specific health policies in the assessment of malaria programs [9-11]. The aim of our study was to present ITN policies (by considering socio-economic factors) applied in the fight against malaria in an African country (Senegal) which is close to malaria elimination.
Using malaria diagnostic test results obtained from Demographics and Health Surveys (DHS) which are nationally representative surveys, we estimated malaria prevalence in each concerned country.
DHS data, used for quantitative analysis of ITN use, is from DHS 2019 for Senegal. We used DHS data from 2010 to 2018toestimate longitudinal progress concerning malaria prevalence in Senegal. There was no data of malaria test available on DHS web site for survey of 2019 in Senegal.
Senegal (16 million inhabitants) is a west African country with a warm and tropical climate. The northern part of Senegal is very hot (dry Sahelian plain). Incidence of malaria in Senegal is 400 per 1,000 population at risk, in 2019 (World Banque. Country Report) [3]. DHS surveys are a cross-sectional, nationally representative survey carried out in developing countries. Firstly, each country was divided into small geographic areas (clusters) and in each cluster, three strata were created: Towns, cities and rural or urban areas. In the second degree, households were selected (a two-stage sampling procedure) [2].
DHS surveys also collect socio-economic data, which we used in this study: urban or rural residence, economic level of the household, possession and use of an ITN (insecticide-treated net), education level in the household, age of head of household, number of rooms in the house and number of household members.
During DHS surveys, a person infected with malaria was determined by several methods such as microscopy or RDT (rapid diagnostic test). For microscopy, blood smears were dried, fixed with methanol and packed. For RDT, immediate diagnostic results were determined during the survey and positive cases received drugs considered to be first-line treatment in the country. Results from microscopy testing were used for the present study [12].
Statistical analyses were performed using IBM SPSS version 20.0 and SAS studio. We performed a linear regression to investigate the relationship between number of ITNs and number of persons in a household, adjusted for age of household head, economic level of household, the highest education level in the household and the area of residence (rural or urban). Normality and homoscedasticity of regression models were verified by observing the shape of points, curves in plots and scatter plots of residuals. Figures representing R-squared in each model were shown with their confidence intervals at 95%.
We estimated the mean number of persons using ITNs among groups (urban or rural areas, wealth level, highest education level in the household and age of household head) and in each country using analysis of variance [13].
We evaluated the importance of socio-economic factors in our linear regression model for the relationship between the number of ITNs in a household and the number of household members by computing the R-squared of each model. We must note that this evaluation was performed considering only areas of intermediate malaria endemicity (prevalence 5-40%) and high endemicity (prevalence > 40%). Areas of low malaria endemicity (malaria prevalence < 5) were not considered in this estimation.
Semi-partial correlation (correlated to R-squared) provides a solid estimate of the relative importance of each predictor in a multiple regression model. Studies have demonstrated the unique contribution of each independent variable in a multiple regression model. The square of semi-correlation represents how much the R-squared value decreases in a model when a predictor is removed. We used the decrease in the R2 value when a co-variable is dropped from the model to assess the importance of a factor in the model for each country (Senegal or Burkina Faso) [14].
Data from DHS surveys used is described in Table 1. We used a sample size of 4538 households.
Table 1: Descriptive of data. View Table 1
We can observe that the proportion of the poorest households is 30.6% and the proportion of urban household sis 29.1%. Since 2010, malaria prevalence was close to 1% in Senegal.
Figure 1 shows the longitudinal trend for malaria prevalence in Senegal, which remains very low.
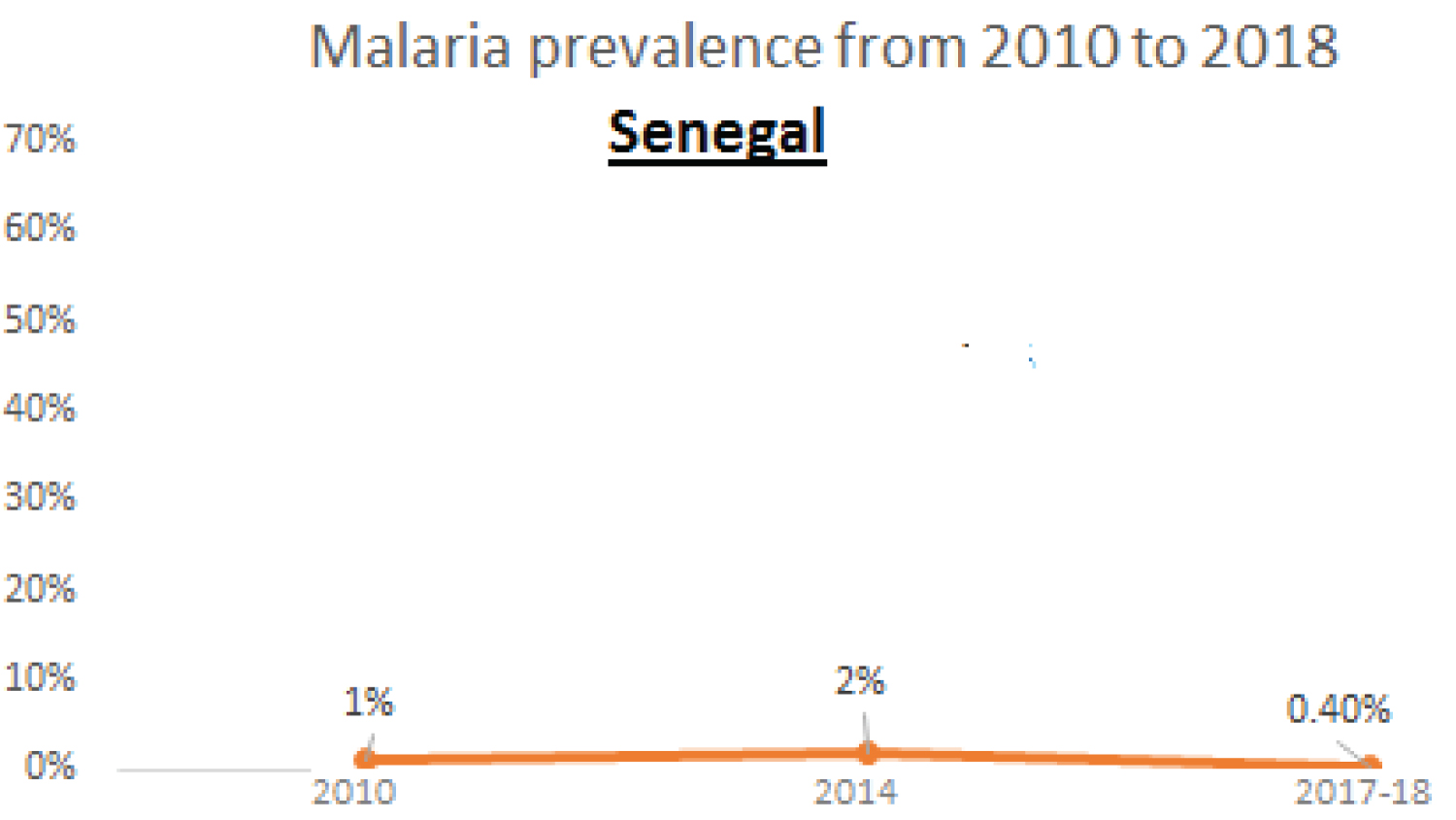 Figure 1: Progress for malaria prevalence in Senegal 2010 to 2018 (DHS surveys) [2].
View Figure 1
Figure 1: Progress for malaria prevalence in Senegal 2010 to 2018 (DHS surveys) [2].
View Figure 1
As the use of ITNs is an important element in the fight against malaria [5], we compared the mean number of ITNs used in sub-groups according socio-economic factors. We found that there is significant difference in the number of ITNs used only considering age of head of households (< 0.0001) (Table 2). Wealth level is an important factor in ITN use [5]. Poor households used not significantly more ITNs than the richest households in Senegal, which is an effective policy. Studies have demonstrated that the poorest houses are at increased malaria risk due to the absence of windows with insect filters [17].
Table 2: Comparison of ITN number used by household in Senegal. View Table 2
We found a positive linear relation between the number of ITNs per household and the number of members per household in Senegal. In Senegal, the number of ITNs per household increases with the household size (Figure 2A). We observe a negative linear relation between the ratio of ITNs number and household size with the number of members per household in Senegal (Figure 2B). In Senegal, the number of ITNs per household increases with the household size. When we controlled the relationship between the number of ITNs and the number of household members with age of household head, economic level of household, place of residence (urban/rural), highest education level in the household and number of sleeping rooms in the household, we found (R2 = 0.3878) (Table 3).
 Figure 2: (A) Evolution of ITN number according to number of household members in Senegal; (B) Evolution of ratio of ITN number with household size and household size in Senegal.
View Figure 2
Figure 2: (A) Evolution of ITN number according to number of household members in Senegal; (B) Evolution of ratio of ITN number with household size and household size in Senegal.
View Figure 2
Table 3: Importance of co-factors in the relationship between the number of ITNs in a household and the number of households members. View Table 3
This result indicates that in Senegal, the number of ITNs in a household increases with the size of the household. Senegal is close to malaria elimination; they need to do more than apply the universal distribution of ITNs. If a resurgence of the disease is to be avoided, Senegal must also organize free distribution in targeted areas and to targeted sub-groups according to surveillance data.
Socio-economic factors such as wealth level must be overcome by policies implemented against malaria. Several studies have noted that poor households have a greater need for the use of ITNs than the richest households [18]. It is very important to reach all categories of households for the distribution of ITNs, particularly household sin targeted areas.
The objective of our study was to provide a view of ITN policies (use and possession) implemented against malaria by considering some socio-economic factors (with best results) in Senegal, which is close to malaria elimination during several years. These could serve as example to others African countries. To achieve our purpose, we used DHS survey data.
Proportion of the poorest households in Senegal (30.6%) this is particularly important for household ownership of bed nets and use. It must be noted also that wealthy people may have access to good housing, good sanitation and environmental management, aid conditioner etc. all factors are determinants to be considered when providing interpretation.ITN data used in this paper is about possession of ITN and use of ITN. Senegal has88.6% of households in which all children under 5 sleep under an ITN. In general, wealth level of households have a positive relation with ITN possession but a negative relation with ITN use. This must be considered in management of the fight against malaria. As mentioned before, although studies have demonstrated that the poorest houses are potentially at higher malaria risk than the richest houses have, this should be relatively discussed with the fact that wealthy people have more access to clean environment, access to other means of protection from malaria and may not need necessary bed nets compared to poorest household [19-21]. In Senegal there is no significant difference between the mean number of ITNs used in households in rural and urban areas. A study by Thwing had found a significant difference between number of possession of ITN between rural and urban households in Senegal in 2010. This study explained that the difference between ITN numbers in urban and rural households in Senegal was due to the fact that Senegal also applied free ITN distribution to children under five. As rural households had more children under five than urban households, it was logical that there were more ITNs in rural areas than in urban areas in Senegal. We found a different result for Senegal 2019 which can be due to policies implemented against malaria in Senegal currently considering more local context [22]. Several studies have demonstrated that the use of ITNs can greatly reduce malaria risk by reducing the rate of mosquito bites and density of mosquitoes [15]. Wealth level is an important factor in ITN possession in African countries [23]. We found that poorest households had the highest mean number of ITN use in Senegal. Studies have demonstrated that the poorest houses are potentially at higher malaria risk than the richest houses [24].
The possession of ITNs (88%) does not necessarily equate to the use of ITNs (58%). The use of ITNs in a population is strongly associated with the education of the population on the prevention of malaria. Senegal must implement communication policies appropriate for the local context and level of education and also age of individuals. We found that, there is no significant difference in the use of ITNs in relation to the highest education level in the household. Number of sleeping room in the households is the most important factor influencing ITN possession according DHS survey 2019 in Senegal. This element must be considered and included in policies implemented against malaria in Senegal [24].
Due to the unavailability of data on malaria test results, analyses were also carried out for clusters where the prevalence of malaria was very low. We must note that Senegal is close to elimination.
We presented ITN policies implemented in the national malaria programs of Senegal according some socio-economic factors.
Being close to malaria elimination and having neighboring countries with high malaria transmission areas, it is a challenge for Senegal to maintain a stable low transmission level, particularly as the immunity of its population against malaria is decreasing. So Senegal implement a lot of active monitoring and surveillance is necessary, such as entomological monitoring in each district or an indoor residual spraying policy, in order to rapidly and locally decrease mosquito vector capacity [25-32].
Our study provided a view of ITN policies applied in an African country, which has strongly succeeded in maintaining low malaria prevalence during several years. These results merit a review in the context of each African country by including a view on others policies against malaria as entomological monitoring, the use of insecticides, management of malaria cases, health system organization, communication and surveillance.
Not applicable.
Not applicable.
DHS data are available on DHS Web site
https://dhsprogram.com/data/available-datasets.cfm
The authors declare that they have no competing interests.
Not applicable.
YC and EM conceived. YC designed the study. EM made statistical analysis. All authors critically reviewed literature synthesis, statistical analysis and interpretation of results.
Many thanks to all co-authors who contributed greatly.