Background: Coronavirus disease (COVID-19) is an infectious disease caused by the SARS-CoV-2 virus, a novel strain of corona virus was first detected in December 2019 in Wuhan, a city of Chinas Hubei province with population of 11 million, after an outbreak of pneumonia without an obvious cause. The virus has now spread to over 200 countries and territories across the globe and was characterized as a pandemic by the world health organization march 2020.
Objective:- To determine the incidence rate of COVID-19 in pediatric and health workers
- To identify the demography of participant’s and epidemiological characteristics of a positive case.
Material and method: Across sectional study in the tertiary hospital in Baghdad city. It was conducted for about two years 2020-2021.The study sample constitutes laboratory- confirmed COVID-19 by testing PCR (polymerase chain reaction) to children attends to the hospital and laboratory-confirmed COVID-19 of health workers in the center, data collected was taken from health workers by face to face interview, about children information which is taken from child’s family.
Data included demographic information like age, gender, job specifications, pre- existing condition (i.e. diabetes, malignancy and so on), mode of presentation asymptomatic or has symptoms like (fever, respiratory symptom, headache, loss of taste, insomnia and so on) , congenital abnormality for children if present , fallow the positive case covid-19 for a consequence of disease may be need admission, not need or admitted to respiratory care unit in severe cases with final result (dead, alive well or alive with complication).
Data were analyzed by using SPSS (statistical software version 20) chi-square test found a significant difference in several characteristics, p-value of 0.05 was considered significant.
Result: The total number of testing PCR (polymerase chain reaction) for children in the year of 2020 was 975 and positive cases was 199 so the incidence rate 20.4%, In 2021 1847 PCR test was done, positive cases 383 so the incidence rate of children equal to 20.7%.
The total number of testing PCR was done to heath workers in the year of 2020 was 3290 and positive cases was 281 so the percentage 8.5%, In 2021 2055 PCR test, positive cases 236 so percentage rate of health workers equal to 11.4%.
The number of children with positive PCR more in spring of year 2020 but in the year 2021 more positive cases in spring and summer, there’s a significant seasonal variation (The p-value was 0.000577. The result was significant at p < 0.05 Positive cases of children more occur in the age group 1-5 years (34%), male more than female in percentage 56.9%, about chronic disease children has cancer & hematological abnormality susceptible to infected than others chronic diseases. symptom present in the children 159 (27.3%) complaining from fever only, 152 (26.1%) complaining from fever with respiratory symptom like cough, shortness of breath, (25.3%) children complaining from respiratory symptom only, gastro intestinal symptom only 2.2%, others (headache, tiredness, myalgia) 1%, no symptoms 101 (17.4%).
During fallow up the final condition of children small percentage complained from complication mostly has chronic disease or congenital anomalies, dead (1.2%) has congenital anomalies or chronic disease.
Health care workers have continued to provide care of patient in spite risk of COVID-19infection, seasonal variation highest percentage of positive cases in summer and autumn2020, in2021 more in the spring. (The p-value is 0.000577. The result is significant at p < 0.05).
From 517 positive case health care workers189 (36,6%) between 30-40years age group. Female more than male, 398 (77%) female infected.
Occupation of health workers, doctors infected 15.3%, nursing staff 8.75, other includes servant, cleaning workers, office clerks, engineers 50%, symptom of health workers 25.7% has only fever, loss of olfactory and tasting 9.9%and 25.1% no symptom, low percentage complaining from complication
Conclusion:COVID-19 positive cases infected with the virus mild to moderate respiratory illness and recover without requiring special treatment. However, some will become seriously ill and require medical attention.
Majority male effected of children, 1-5 years’ group major effected Majority female of the health workers, group of 30-40 years major effected Fever most common symptom in both children and health workers, in children 17.4% asymptomatic, 25% asymptomatic of health workers.
Epidemiological study, Single center, COVID 19, Baghdad city-Iraq
COVID-19: Corona virus disease 2019; WHO: World Health Organization; SARS-CoV-2: SARS Coronavirus 2
Coronavirus disease (COVID-19) is an infectious disease caused by the SARS-CoV-2 virus [1]. SARS-CoV-2 is a new type of coronavirus that has not been found in humans before. SARS-CoV-2 is characterized by its rapid spread, high contagiousness, and the high susceptibility of the population [2].
Most people infected with the virus will experience mild to moderate respiratory illness and recover without requiring special treatment. However, some will become seriously ill and require medical attention [1]. The current COVID-19 pandemic is caused by a coronavirus named SARS-CoV-2. Coronaviruses are a large family of viruses, several of which cause respiratory diseases in humans, from the common cold to rare and serious diseases such as the Severe Acute Respiratory Syndrome (SARS) and the Middle East respiratory syndrome (MERS), both of which have high mortality rates and were detected for the first time in 2003 and 2012, respectively. Coronaviruses are divided into four genera: alpha-, beta-, gamma- and delta SARS-CoV-2. All SARS-CoV-2 Coronaviruses currently known to cause disease in humans belong to the alpha- or the beta-CoV. Many of these CoVs can infect several animal species as well. CoVs infected civet cats and infected humans in 2002 and MERS-CoV is found in dromedary camels and infected humans in 2012. A virus that is regularly transmitted from an animal to a human is called a zoonotic virus [3].
The coronavirus disease caused by SARS-CoV-2, were first reported from Wuhan City, China, in December 2019. All SARS-CoV-2 isolated from humans to date are closely related genetically to coronaviruses isolated from bat populations, specifically, bats from the genus Rhinolophus. CoV, the cause of the SARS outbreak in 2003, is also closely related to coronaviruses isolated from bats [3]. The virus that causes COVID-19 is constantly changing, and new variants of the virus are expected to occur. Sometimes new variants emerge and disappear.
Other times, new variants persist. Numerous variants of the virus that causes COVID-19 are being tracked in the United States and globally during this pandemic [4].
The principal mode by which people are infected with SARS-CoV-2 is through exposure to respiratory fluids carrying infectious virus. Exposure occurs in three principal ways: 1- inhalation of very fine respiratory droplets and aerosol particles, 2- deposition of respiratory droplets and particles on exposed mucous membranes in the mouth, nose, or eye by direct splashes and sprays, and 3- touching mucous membranes with hands that have been soiled either directly by virus-containing respiratory fluids or indirectly by touching surfaces with virus on them [5].
People release respiratory fluids during exhalation (e.g. quiet breathing, speaking, singing, exercise, coughing, sneezing) in the form of droplets across a spectrum of sizes These droplets carry virus and transmit infection. The largest droplets settle out of the air rapidly, within seconds to minutes. The smallest very fine droplets, and aerosol particles formed when these fine droplets rapidly dry, are small enough that they can remain suspended in the air for minutes to hours, factors that increase the risk of SARS-CoV-2 infection under these circumstances include enclosed spaces with inadequate ventilation or air handling within which the concentration of exhaled respiratory fluids, especially very fine droplets and aerosol particles [5]. Younger people also become infected, although they have milder clinical manifestations than adults and the elderly [6].
There are different types of disease presentation based on the age of the person who is infected by this virus. Luckily, children and adolescents tend to have more mild disease compared to adults. Most people who are infected with the SARS- CoV-2 virus have respiratory symptoms. They start to feel a little bit unwell, they will have a fever, they may have a cough or a sore throat or sneeze. In some individuals, they may have gastrointestinal symptoms. Others may lose the sense of smell or the sense of taste. Especially in the youngest children, they tend to be more mild, which means they don't have as many symptoms as adults do. Some children may have gastrointestinal symptoms like diarrhea or vomiting, but they tend to be more mild. And even most children tend to have asymptomatic infection, which means they don't have any symptoms at all [7]. Every age may be affected but childhood seems to be safeguarded by severe COVID-19, due to comorbidities associated with lethal COVID-19 infection (obesity, diabetes and chronic heart disease) [8].
The total number of testing PCR (polymerase chain reaction) for children in the year of 2020 was 975 and positive cases was 199 so the incidence 20.4%. In 2021 1847 PCR test was done, positive cases 383 so incidence rate of children equal to 20.7%.
The total number of testing PCR was done to heath workers in the year of 2020 was 3290 and positive cases was 281 so the incidence 8.5%. In 2021 2055 PCR test, positive cases 236 so incidence rate of health workers equal to11.4%.
Number of children with positive PCR more in spring of year 2020 but in the year 2021 more positive cases in spring and summer, there’s a significant seasonal variation (The p-value is 0.000577. The result is significant at p < 0.05). Seasonal variation of children seen in the Figure 1, Figure 2 and Table 1.
 Figure 1: Seasonal variation of positive cases child in the year 2020.
View Figure 1
Figure 1: Seasonal variation of positive cases child in the year 2020.
View Figure 1
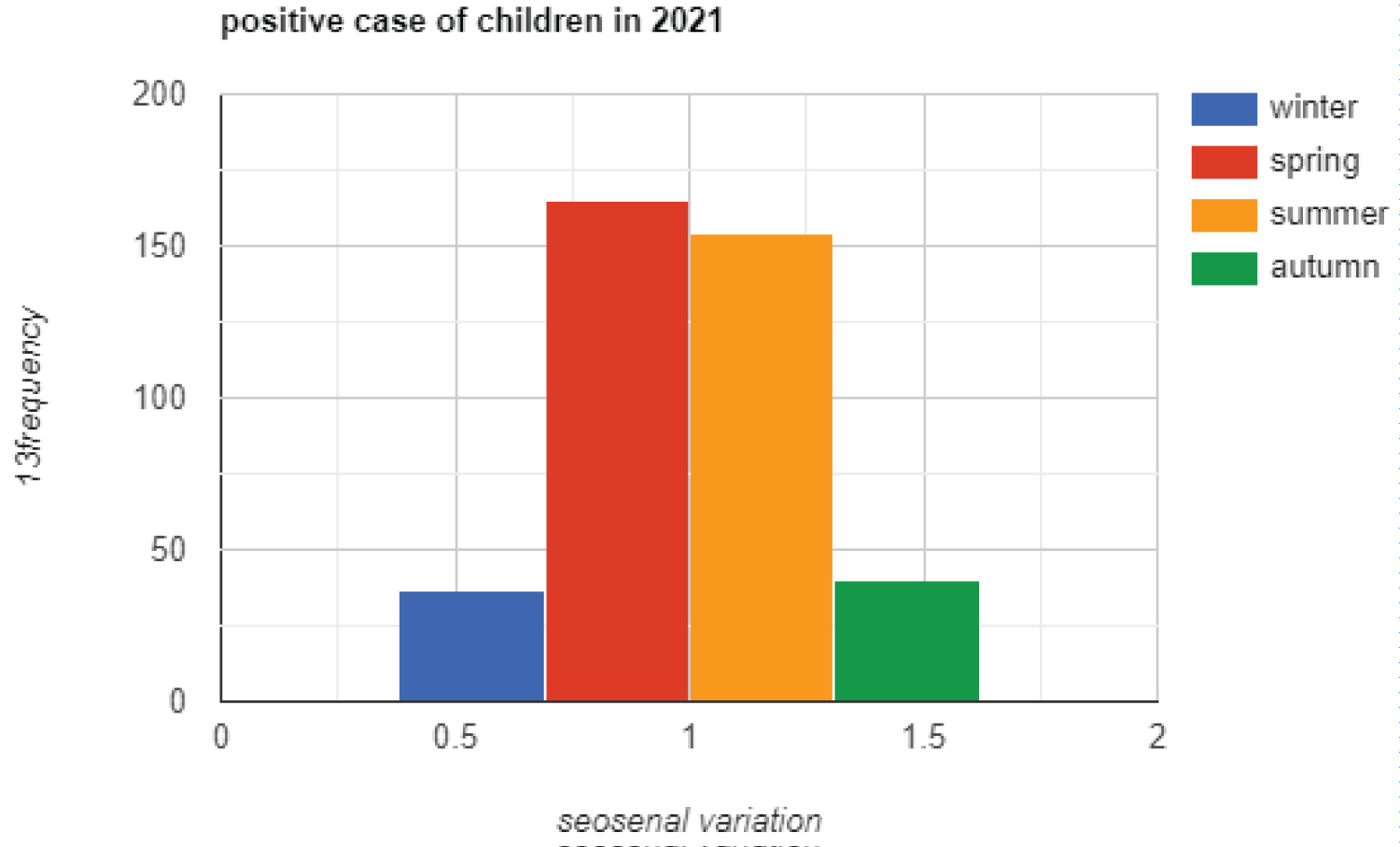 Figure 2: Seasonal variation of positive cases child in the year 2021.
View Figure 2
Figure 2: Seasonal variation of positive cases child in the year 2021.
View Figure 2
Table 1: Crosstab between children positive cases and seasonal variation. View Table 1
Positive cases of children more occur in the age group 1-5 years (34%), male more than female in percent 56.9%, about chronic disease children has cancer & hematological abnormality susceptible to infected than others chronic diseases present in the Table 2 and Table 3.
Table 2: Frequency with percentage of the age and gender of children. View Table 2
Table 3: Frequency with percentage of chronic diseases - congenital abnormality of children. View Table 3
Symptom present in the children, 159 (27.3%) has only fever, 152 (26.1%) complaining from fever with respiratory symptom like cough, shortness of breath. respiratory symptom without fever 147 (25.3%), gastro intestinal symptom 2.2%, others (headache, tiredness, myalgia) 1%, no symptoms 101 (17.4%).
PCR done to all children attending to the hospital complaining or for checkup before any intervention like surgery, dialysis and so on. During fallow up the final condition of children small percentage complained from complication mostly has chronic disease or congenital anomalies, dead 9 (1.2%) already has congenital anomalies or chronic disease.
Symptoms of the disease with final state of children participants present in the Table 4.
Table 4: Symptom - final result of children. View Table 4
Health care workers have continued to provide care of patient in spite the risk of infection, seasonal variation highest percentage of positive cases in summer and autumn 2020, in 2021 more in the spring, there is significant about seasonal variation The p-value is 0.000577. The result is significant at p < 0.05 present in Figure 3, Figure 4 and Table 5.
 Figure 3: Seasonal variation of positive cases of health workers in the year 2020.
View Figure 3
Figure 3: Seasonal variation of positive cases of health workers in the year 2020.
View Figure 3
 Figure 4: Seasonal variation of positive cases of health workers in the year 2021.
Figure 4: Seasonal variation of positive cases of health workers in the year 2021.
Note: Please change the seosenal spelling to Seasonal in all the four figures.
View Figure 4
Table 5: Seasonal variation crosstab 2020, 2021. View Table 5
From 517 positive case health care workers 189 (36.6%) in 30-40years age group. Female more than male, 398 (77%) female infected. About occupation, doctors infected 15.3%, pharmacist 8.7% nursing staff 8.75, lab technician 15.1% other includes servant, cleaning workers, office clerks, engineers 50.3%, present in the Table 6.
Table 6: Age-gender & occupation. View Table 6
About symptom of health workers 25.7% has only fever, loss of olfactory and tasting 9.9% and 25.1% no symptom, low percentage complaining from complication.
Symptoms, chronic disease and final condition of health workers present in the Table 7.
Table 7: Symptom-chronic disease-final result. View Table 7
The total number of testing PCR (polymerase chain reaction) for children in the year of 2020 was 975 and positive cases was 199 so the percentage rate 20.4%. In 2021 1847 PCR test was done, positive cases 381 so percentage rate of children equal to 20.7%.
The total number of testing PCR was done to heath workers in the year 0f 2020 was 3290and positive cases was 281 so the percent 8.5%. In 2021 2055 PCR test, positive cases 236 so percent of health workers equal to 11.4%.
The number of children with positive PCR more in spring of year 2020 but in the year 2021 more positive cases in spring and summer, there’s a significant seasonal variation (The p-value is 0.000577). The result is significant at p < 0.05.
Positive cases of children more occur in the age group 1-5 years (34%), male more than female in percent 56.9%, About symptom present in the children 159 (27.3%) has fever only, 152 (26.1%) complaining from fever with respiratory symptom like cough, shortness of breath, children complaining from respiratory symptom without fever 147 (25.3%), gastro intestinal symptom only 2.2%, others (headache, tiredness, myalgia) 1%, no symptoms 101 (17.4).
During fallow up the final condition of children small percentage complained from complication mostly has chronic disease or congenital anomalies, dead 9 (1.2%) already has congenital anomalies or chronic disease.
Health care workers have continued to provide care of patient in spite risk of infection, seasonal variation highest percentage of positive cases in summer and autumn 2020, in 2021 more in the spring.
From 517 positive case health care workers 189 (36.6%) in 30-40years age group. Female more than male, 398 (77%) female infected.
About occupation, doctors infected 15.3%, pharmacist 8.7%, lab technician 15.1% nursing staff 8.75%, health workers complaining from fever 25.7%, loss of olfactory and tasting 9.9% and 25.1% no symptom, low percentage complaining from complication.
Study in china, more women than men were diagnosed with COVID-19 in Gansu Province Thirty-six (53.7%) of the patients were women and thirty-one (46.3%) men. And the median ages were 40 (IQR 31-53) years [2].
French study, they were predominantly female (63%) and their median age was 44 years [9].
Study from North-East Nigeria Majority of children were asymptomatic (60.4%), while 32.1% and 7.5% had mild and moderate diseases respectively. The most common symptoms were cough (20.8%), fever (17%), and sneezing (15.1%). Five children (9.4%) complained of loss of taste while anosmia was documented in one child (1.9%) [10]. Screening clinic of a tertiary care hospital in Peshawar, Pakistan found infections were more frequent among male gender accounting for 85 (70.25%) patients.
Common symptoms included fever (88 patients, 72 %), cough (72 patients, 59.5%) and shortness of breath [11]. Care workers in three hospitals in the south of the Netherlands, Health-care workers are at increased risk of being exposed to viruses within hospitals but can also be a source of transmission by introducing a virus into their hospital. SARS- CoV-2 infections in health-care workers can have a substantial effect, because pathogens are introduced into settings with high numbers of individuals with comorbidities [12]. Study of Saudi Arabia more than half (74.1%) of COVID-19 patients were female; most of them were employed 85 (48.9%). About 163 (93.7%) cases were asymptomatic [13].
The estimated nationwide community-based prevalence of COVID19 was 6.4% in Bangladesh between April and October 2020. The prevalence of COVID-19 was almost the same in urban (5%) and rural (7%) areas. Asymptomatic COVID-19 cases were estimated to be high (87%) among the positive cases of COVID-19, in the study population nationwide. The highest peak of COVID-19 cases were in June 2020, which was immediately after the end of the first nationwide restricted movement in Bangladesh [14]. In a tertiary care center in Bangkok, Thailand.
The spectrum of disease included 82 (20%) asymptomatic, 232 (56%) mild and 102 (24%) with pneumonia. Abnormal chest x-ray findings included ground-glass opacities (46%), focal infiltrations (27%), perihilar opacities (19%), reticular infiltrations (15%) and other non-specific findings (4%). Only 12 children (3%) required oxygen support. Favipiravir was prescribed to 129 children (31%); 102 patients with pneumonia and 27 patients at risk for disease progression.
Pneumonia was more common in all age [15]. Study in the United State and 6 in Canada, 25 (52%) were male, and the median (range) age was 13 (4.2-16.6) years Forty patients (83%) had significant preexisting comorbidities, 35 (73%) presented with respiratory symptoms [16].
In a population-based study in Iceland, children under 10 years of age and females had a lower incidence of SARS-CoV-2 infection than adolescents or adults and males [17].
Controlling the infection by wearing mask. Masks are a key measure to reduce transmission and save lives. maintaining physical distancing, avoiding crowded, closed and close-contact settings, ensuring good ventilation of indoor spaces, cleaning hands regularly, and covering sneezes and coughs with a tissue of bent elbow. Depending on the type, masks can be used for either protection of healthy persons or to prevent onward transmission, or both [18]. Corona vaccines are very important part for prevention from corona disease Vaccinating not only protects yourself, but also protects those in the community who are unable to be vaccinated [19].
The authors would like to thank participants.
No funding was received for this study.
The authors declare that they have no competing interests.