The emergence of the novel Corona virus disease (COVID-19) in Wuhan city, China, in December, 2019 ushered in changes in the state of events globally. The pandemic has shaken the global health system and economy to their bases. The epidemic of Covid-19 is still ongoing and showing no signs of decreasing trend. An intriguing fact is that in every decade of the 21st century, there is a new major corona virus epidemic; severe acute respiratory syndrome (SARS) IN 2002, Middle East respiratory syndrome (MERS) IN 2012 and now Covid-19. The World Health Organization (WHO) categorised Nigeria as one of the thirteen (13) African Countries vulnerable and at high risk of the disease as a result of the poor state of her health infrastructure. Covid-19 Vaccine may be the most practical and feasible solution to curb the menace of the disease. Aside the technological and medical hurdles involved in vaccine production, one of the major challenges is the apathy and hesitancy of the masses to the vaccine. Several covid-19 vaccines have been produced and rolled out to different Countries including Nigeria. To prevent hesitancy and apathy towards the use of the vaccines; y = the public must be targeted with multifaceted interventions aimed at raising awareness and emphasizing the safety and efficacy of the vaccine.
The corona virus disease (COVID-19) is a highly transmittable and pathogenic viral infection caused by severe acute respiratory syndrome corona virus 2 (SARS-CoV-2), which caused a global pandemic that led to a dramatic loss of human lives worldwide.
Corona virus is one of the major pathogens that primarily target the human respiratory system. Previous outbreaks of corona viruses (CoVs) include the severe acute respiratory syndrome (SARS)-CoV and the Middle East respiratory syndrome (MERS)-CoV which have been previously characterized as agents that are a great public health threat [1]. Corona viruses belong to the Coronaviridae family in the Nidovirales order. Corona represents crown-like spikes on the outer surface of the virus; thus, it was named a corona virus. Corona viruses are minute in size (65-125 nm in diameter) and contain a single-stranded RNA as a nucleic material, size ranging from 26 to 32 kbs in length. The subgroups of the corona viruses family are alpha (α), beta (β), gamma (γ), and delta (δ) corona virus [2]. Corona viruses infect mammals and birds in rare cases but animal corona viruses may evolve and infect humans and then spread from person to person [3]. According to the World Health Organization, the 2003 SARS outbreak originated with civet cats and the 2012 MERS outbreak with dromedary camels.
Corona viruses were thought to infect only animals until the world witnessed a severe acute respiratory syndrome (SARS) outbreak caused by SARS-CoV, 2002 in Guangdong, China [4]. Only a decade later, another pathogenic corona virus, known as Middle East respiratory syndrome corona virus (MERS-CoV) caused an endemic in Middle Eastern countries [5]. Recently at the end of 2019, Wuhan an emerging business hub of China experienced an outbreak of a novel corona virus that killed more than Eighteen hundred and infected over Seventy thousand individuals within the first fifty days of the epidemic [1]. This virus was reported to be a member of the β group of corona viruses. The novel virus was named as 2019-nCov by the Chinese researchers. The International Committee on Taxonomy of Viruses (ICTV) named the virus SARS-CoV-2 and the disease COVID-19 [6].
The genetic sequence of the COVID-19 showed more than 80% identity to SARS-CoV and 50% to the MERS-CoV and both SARS-CoV and MERS-CoV originate in bats [6]. Thus, the evidence from the phylogenetic analysis indicates that the COVID-19 belongs to the genus betacorona virus, which includes SARS-CoV that infects humans, bats, and wild animals. COVID-19 represents the seventh member of the corona virus family that infects humans and has been classified under the Orthocoronavirinae subfamily. The COVID-19 forms a clade within the subgenus sarbeco virus. Based on the genetic sequence identity and the phylogenetic reports, COVID-19 is sufficiently different from SARS-CoV and it can thus be considered as a new Beta corona virus that infects humans. COVID-19 most likely developed from bat-origin corona viruses. Another piece of evidence that supports that COVID-19 is of bat origin is the existence of a high degree of homology of the ACE2 receptor from a diversity of animal species, thus implicating these animal species as possible intermediate hosts or animal models for COVID-19 infections [7]. Moreover, these viruses have a single intact open reading frame on gene 8, which is a further indicator of bat-origin CoVs. However, the amino acid sequence of the tentative receptor-binding domain resembles that of SARS-CoV, indicating that these viruses might use the same receptor [8].
The "2019 Novel Coronavirus" was first identified in January 2020. Early cases were associated with a seafood and live animal market in Wuhan City, China [7]. The first cases were reported in December 2019 [9]. From December 18, 2019, through December 29, 2019, five patients were hospitalized with acute respiratory distress syndrome and one of these patients died [10]. By January 2, 2020, 41 admitted hospital patients had been identified as having laboratory-confirmed COVID-19 infection, less than half of these patients had underlying diseases, including diabetes, hypertension, and cardiovascular disease. These patients were presumed to be infected in that hospital, likely due to nosocomial infection. It was concluded that the COVID-19 is not a super-hot spreading virus (spread by one patient to many others), but rather likely spread due to many patients getting infected at various locations throughout the hospital through unknown mechanisms. In addition, only patients that got clinically sick were tested, thus there were likely many more patients that were presumably infected [11].
The disease has spread to more than 200 countries with over 200 million cases, approximately 4.1 million deaths, and 180 million recoveries worldwide according to the World Health Organization as of August 2021 [1]. The US has the highest number of reported infections and deaths in the world. India while Brazil, Russia, and France have the highest number of infections after the US. Brazil, India, Mexico, and Peru have the highest number of deaths after the US. In Nigeria, 180,661 cases have been confirmed, 165,122 cases have been discharged and 2163 deaths have been recorded in 36 states and the Federal Capital Territory as of 8th August 2021 [12].
At their core, corona viruses contain a genetic blueprint called RNA similar to DNA. The single-stranded RNA acts as a molecular message that enables production of proteins needed for other elements of the virus. Bound to this string of RNA are nucleoproteins- (dark blue discs)-proteins that help give the virus its structure and enable it to replicate. Encapsulating the RNA genome is the viral envelope (teal), which protects the virus when it is outside of a host cell. This outer envelope is made from a layer of lipids, a waxy barrier containing fat molecules. As well as protecting the precious genetic cargo, this layer anchors the different structural proteins needed by the virus to infect cells. Envelope proteins (dark blue dots) embedded in this layer aid the assembly of new virus particles once it has infected a cell. The bulbous projections seen on the outside of the corona virus are spike proteins (red-orange). This fringe of proteins gives the virus its crown-like appearance under the microscope, from which the Latin name corona is derived. The spike proteins act as grappling hooks that allow the virus to latch onto host cells and crack them open for infection. Like all viruses, corona viruses are unable to thrive and reproduce outside of a living host [13] (Figure 1).
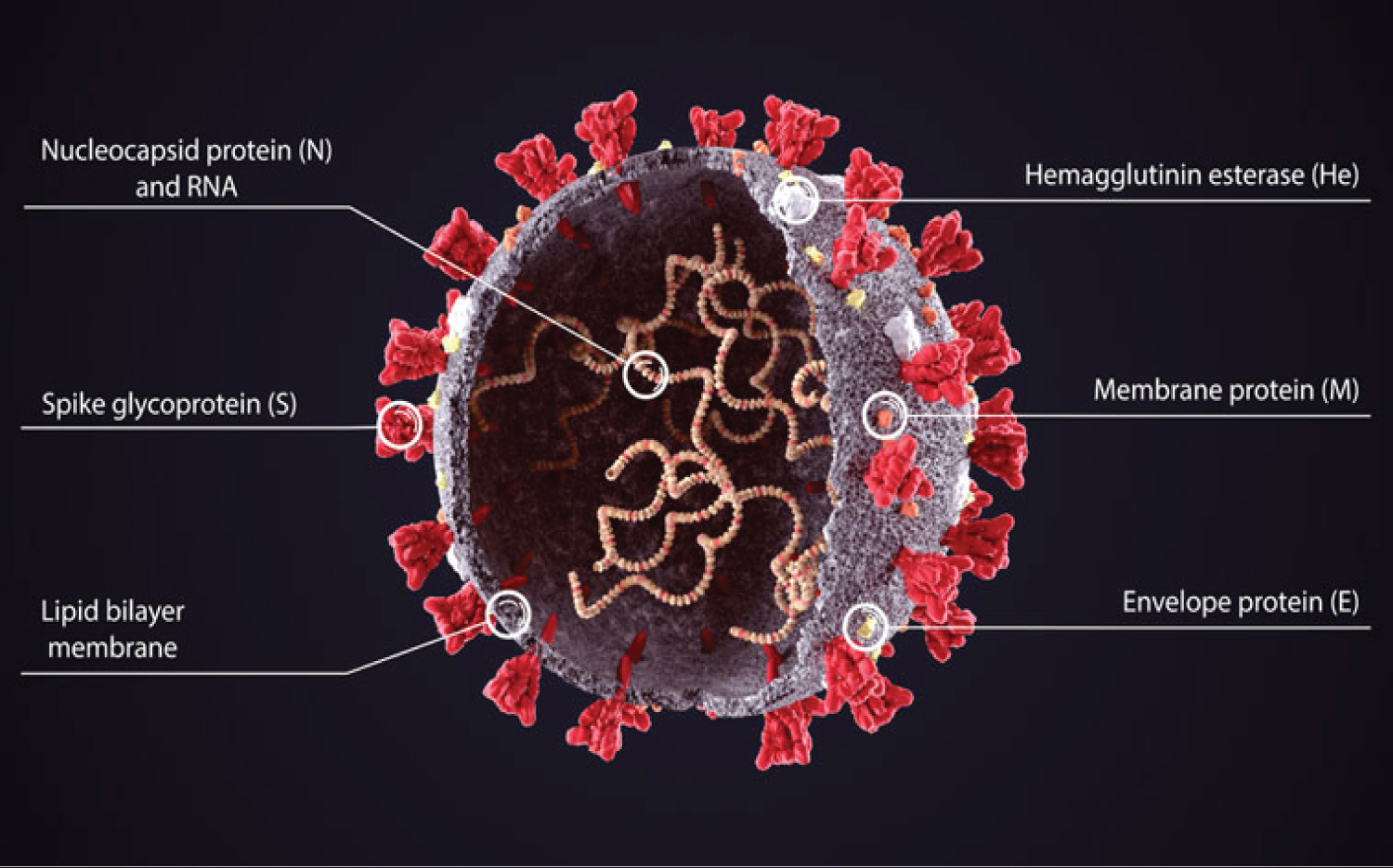 Figure 1: Structure of SARS-CoV-2 [1].
View Figure 1
Figure 1: Structure of SARS-CoV-2 [1].
View Figure 1
Based on the large number of infected people that were exposed to the wet animal market in Wuhan City where live animals are routinely sold, it is suggested that this is the likely zoonotic origin of the COVID-19. Efforts have been made to search for a reservoir host or intermediate carriers from which the infection may have spread to humans. Initial reports identified two species of snakes that could be a possible reservoir of the COVID-19. However, to date, there has been no consistent evidence of corona virus reservoirs other than mammals and birds [14]. Genomic sequence analysis of COVID-19 showed 88% identity with two bat-derived severe acute respiratory syndromes (SARS)-like corona viruses indicating that mammals are the most likely link between COVID-19 and humans. Several reports have suggested that person-to-person transmission is a likely route for spreading COVID-19 infection [15].
COVID-19 is primarily transmitted from person to person through respiratory droplets. These droplets are released when someone with COVID-19 sneezes, coughs or talks. Infectious droplets can land in the mouths or noses of people who are nearby or possibly be inhaled into the lungs. Respiratory droplets can land on hands, objects or surfaces around the person when they cough or talk, and people can then become infected with COVID-19 from touching hands, objects or surfaces with droplets and then touching their eyes, nose, or mouth [16].
Recent data suggest that there can be a transmission of COVID-19 through droplets of those with mild symptoms or those who do not feel ill. Current data do not support the long-range aerosol transmission of SARS-CoV-2, such as those seen with measles or tuberculosis. Short-range inhalation of aerosols is a possibility for COVID-19, as with many respiratory pathogens. However, this cannot easily be distinguished from "droplet" transmission based on epidemiologic patterns. Short-range transmission is a possibility particularly in crowded medical wards and inadequately ventilated spaces. Certain procedures in health facilities can generate fine aerosols and should be avoided whenever possible [17].
The development of a new COVID-19 strains or variants is not unique, it occurs in all viruses. The scientists studying the disease and developing COVID vaccines have always anticipated that new strains would evolve. Viruses mutate when they replicate and create a slightly different version of the virus. Many variants of COVID-19 have been discovered. Variants that appear to meet one or more of these criteria may be labelled "variants under investigation" or "variants of interest" [1]. The primary characteristic of a variant of interest is that it shows evidence that demonstrates it is the cause of an increased proportion of cases or unique outbreak clusters; however, it must also have limited prevalence or expansion at national levels, or the classification would be elevated to a "variant of concern" If there is clear evidence that the effectiveness of prevention or intervention measures for a particular variant is substantially reduced, that variant is termed a "variant of high consequence" [8].
In late 2020, experts noted gene mutations in COVID-19 cases seen in people of southeastern England. This variant has since been reported in other countries, including the U.S. Scientists estimated that these mutations could make the virus up to 70% more transmissible, meaning it could spread more easily. Some research has linked this variant to a higher risk of death, but the evidence is not strong [18]. The mutation on the alpha variant is on the spike protein, which helps the virus infect its host and this is what COVID-19 vaccines target. These vaccines make antibodies against many parts of the spike protein, so it is unlikely that a single new mutation in the alpha variant will make the vaccine less effective.
This variant of the virus have been found in other countries, including South Africa and Nigeria. The beta variant appears to spread more easily than the original virus but does not seem to cause worse illness [19].
In January 2021, experts spotted this COVID-19 variant in people from Brazil who had traveled to Japan. By the end of that month, it was showing up in the U.S. The gamma variant appears to be more contagious than earlier strains of the virus and it may be able to infect people who have already had COVID-19. A report from Brazil confirms that a 29-year-old woman came down with this variant after an earlier corona virus infection a few months before [20].
This variant was spotted in India in October 2020. It caused a huge surge in cases beginning in Mid-April 2021. The highly contagious variant is now found in more than 130 countries including the U.S. The delta variant has now become a dominant strain in the U.S due to community spread. This variant was observed to cause more cases of COVID-19 in young people [21].
The symptoms of COVID-19 infection appear after an incubation period of approximately 5 days. The period from the onset of COVID-19 symptoms to death ranged from 6 to 41 days with a median of 14 days. This period is dependent on the age of the patient and the status of the patient's immune system. It was shorter among patients > 70-years old compared with those under the age of 70 [9]. A wide range of symptoms for COVID-19 has been reported by the World Health Organization these which include: Fever or chills, Cough, Shortness of breath or difficulty breathing, Fatigue, Headache, Nasal congestion or runny nose, Muscle or body aches, sore throat, new loss of smell or taste, Nausea or vomiting, headache, haemoptysis, dyspnoea, lymphopenia and Diarrhoea. It is important to note that some people become infected and do not develop any symptoms or feel unwell. Patients infected with COVID-19 showed higher leukocyte numbers, abnormal respiratory findings and increased levels of plasma pro-inflammatory cytokines [1].
It is important to note that COVID-19 is a new disease, therefore there is limited information regarding risk factors for severe disease. The risk of severe disease increases steadily as people age. Additionally, those of all ages with underlying medical conditions (including but not limited to heart disease, diabetes, or lung disease) appear to be at higher risk of developing severe COVID-19 compared to those without these conditions. As more data become available, additional risk factors for severe COVID-19 may be identified [19].
Vaccines are biologics that provide active adaptive immunity against specific diseases [2]. Vaccine development involves utilizing the microorganisms responsible for the disease either in the killed or attenuated form or it involves the use of micro-organisms toxins or surface proteins. The vaccines are introduced in the body via the mouth, injection or by nasal route to incite the immune system against foreign bodies. In the process of immunity development, the body produces antibodies against specific microorganisms, which generates the defense mechanism. When a person encounters the same microorganisms later, the antibodies produced by the body in response to the microorganisms' antigens either prevents the person from the disease induced by the microorganism or lessens the severity of the disease. Vaccines in general are considered the most economical healthcare interventions and it is said that "A dollar spent on a childhood vaccination not only helps save a life but greatly reduce spending on future healthcare" [22].
Years of research enable a COVID-19 vaccine to be developed in record time. There are many different corona viruses. SARS-CoV-2, the virus that causes COVID-19, is just one; others can cause illnesses like the common cold [23]. Before the COVID-19 pandemic began, experts at the NIH Vaccine Research Centre (VRC) were studying corona viruses to find out how to protect against them. The scientists chose to focus on one "prototype" corona virus and create a vaccine for it. That vaccine could then be customized to fight different corona viruses. This vaccine needed to be three things: Fast, Reliable and Universal [1].
As of August 19, 2021, over 200 million confirmed cases of COVID -19 infection and over 4 million deaths due to COVID-19 globally had been reported to the World Health Organization. Nigeria, like a lot of African countries, seems to have been spared the worst of the pandemic. To date, the Nigerian Center for Disease Control (NCDC) has recorded about 165,000 confirmed cases of COVID -19 infections [12]. According to the Nigerian Primary Health Care Development Agency [24], the agency in charge of the vaccine roll-out, the country received 3.92 million out of the expected 14 million doses of Oxford/AstraZeneca vaccine through COVAX on March 2nd, 2021 and also took delivery of 177,600 doses of Johnson & Johnson vaccines, being part of the 29,850,000 doses that the Federal Government of Nigeria procured through the AVAT of the AU Commission, using the facility provided by African Export-Import Bank (Afreximbank). This batch of J&J vaccines will be focused on those who are in the hard-to-reach areas, riverine areas, desert areas, and security-compromised areas, the elderly and frail individuals, across the country. This is because the J&J vaccine is administered as a single dose vaccine, unlike the AstraZeneca and Moderna that require two doses for complete vaccination. The J&J vaccine have been listed for emergency use by WHO on March 12, 2021. The vaccine has been authorized for use in Europe, the United States, and other countries [25].
As of April 28, 2021, about doses of the Oxford AstraZeneca vaccines had been administered. Nigeria has reported a little over 1 million vaccinations. Most of these have been given to health workers, older people, and people with medical co -morbidities. There were rare but serious events of interest that occurred in the trials and post-trial period. These include reports of rare but serious cases of blood clots with low platelets likely associated with both the AstraZeneca and Johnson & Johnson vaccines according to the European Medical Agency (EMA) and the US centre for disease control (CDC) respectively. These rare types of blood clots mostly occurred in women less than 60-years-old. A few of these events resulted in death [12].
Both CDC and EMA continue to advise that the benefit of vaccination outweighs the risk for a vast majority of people. Israel and US military members also recently reported rare cases of myocarditis inflammation of heart muscles in young men less than 30-years-old after the Pfizer and Moderna vaccines. It will not be unusual to hear more reports of seemingly bad events happening after the vaccines are administered. This does not always mean that those events were caused by the vaccine [1]. Traditional vaccine development has been a complex and time-consuming process that typically takes around 10-15 years. Vaccines typically require several years of research and development, three phases of trials with human participants, and final approval by the CDC and FDA [9]. Some other Covid-19 vaccines approved through emergency use are; BNT162 vaccine by Pfizer and BioNTech, mRNA-1273 vaccine by Moderna, CoronaVac by Sinovac and COVID-19 vaccine by Sinopharm and the Wuhan Institute of Virology, China [1,26].
Figure 2 and Figure 3.
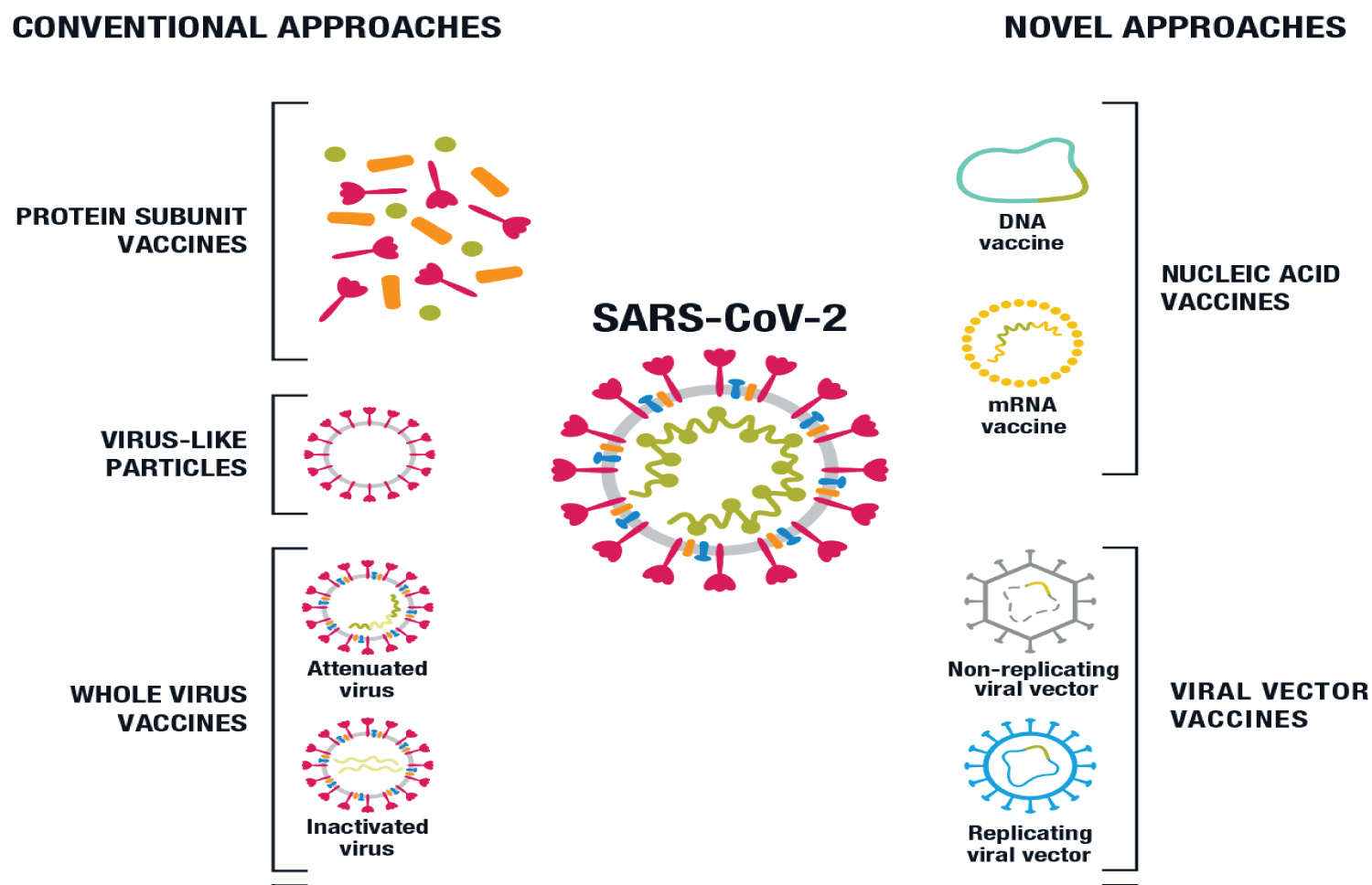 Figure 2: COVID- 19 learning network.org
Figure 2: COVID- 19 learning network.org
Approaches in Production of vaccine against SARS-CoV-2 [1].
View Figure 2
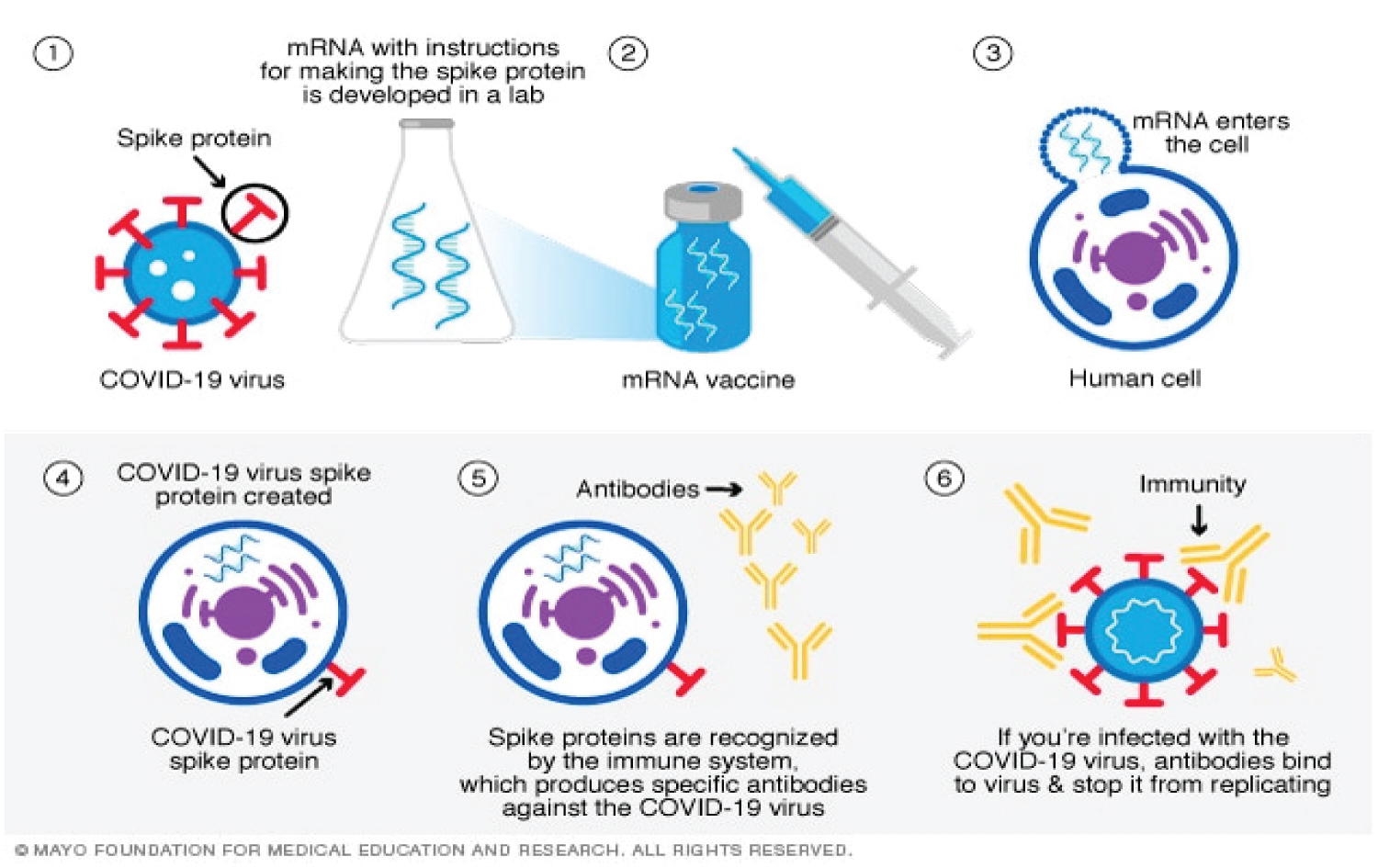 Figure 3: Mechanism of Action of COVID-19 Using Mrna Vaccine [27].
View Figure 3
Figure 3: Mechanism of Action of COVID-19 Using Mrna Vaccine [27].
View Figure 3
Nigeria is a multi-ethnic, multi-cultural and multi-religious country. Experiences with the GAVI-supported routine immunization program show vaccination coverage rates differ across the country with higher coverage rates in the southern states compared to the north, and within states, higher coverage rates in urban compared to rural areas. Disparities in rates are also observed when a comparison is made across caretaker literacy levels, family wealth index, and caretaker age [21]. The polio vaccination refusal saga in 3 states in northern Nigeria between 2003 and 2004 is a grim reminder of how public mistrust of government intentions and the international community, political and religious discordances and poor community engagement can disrupt a vaccination program intended for the good of the people with grave consequences. It stresses the need for a clear understanding of the context-specific factors that may influence a COVID-19 vaccination program in Nigeria and the timely implementation of strategies to achieve high coverage rates when a vaccine eventually becomes available in the country.
Nigeria is the most populated country in Africa and has a convoluted history of vaccine hesitancy. Vaccination coverage in Nigeria has continuously dropped since its peak of 81.5% in the 1990s, and by 2013, only 25% of children under the age of 2 were fully vaccinated. The 2003/2004 polio vaccine refusal in Nigeria had a far-reaching effect. It increased the incidence of polio by many folds in Nigeria and contributed to outbreaks of polio across three other continents [28].
Over the last two decades, worldwide, vaccination programs for polio, whooping cough, diphtheria, and measles have significantly reduced the prevalence of these diseases. Despite the benefits vaccination reap for public health, this fundamental effort for disease control still faces major obstacles globally and Nigeria is not an exception. It has been noted that one of the major obstacles to vaccine acceptance is the public perception of the relative risks and benefits of vaccination. Summarized into the acronym VAMRIS V = Vaccine hesitancy; A = Attitude and uptake by health care workers; M = Misinformation; R = Religion; I = Immunization rollout plans; S = Social influences and enabling environment [29].
Vaccine hesitancy is defined as a delay in acceptance or denial of vaccination regardless of the accessibility of vaccination services [2]. Vaccine hesitancy is complicated and context-specific, differing across time, place and vaccine to vaccine. It is affected by factors such as complacency, convenience and confidence. If there is greater hesitancy, it can lead to reduced vaccine demand. However, low levels of hesitancy do not certainly mean a higher vaccine demand. The vaccine hesitancy determinants matrix illustrates the factors affecting the behavioural decision to accept, delay or reject some or all vaccines, beneath three categories namely contextual, individual and group, and vaccine/vaccination-specific influence [30].
Vaccine hesitancy could have a direct and wide-reaching effect on the acceptance of COVID-19 vaccine(s) by individuals in the community as it confers threat not only on the hesitant individual but on the community as a whole, as delays and refusals would make it impossible for communities to reach the threshold of vaccine uptake necessary for the conferment of herd immunity. Vaccine hesitancy, also known as anti-vax/anti-vaccination, which has been identified by the World Health Organization (WHO) as one of the top 10 global health threats is a reluctance or refusal to be vaccinated or to have one's children vaccinated against contagious diseases like COVID-19 [2]. Vaccine hesitancy stems from multiple key factors including, complacency, lack of confidence in the vaccine and convenience. In Africa, vaccine hesitancy is a complex public health issue. In the past years, there have been a series of reports on vaccine scandals including reports on critical side-effects of vaccination leading to increased vaccination hesitancy. Vaccine hesitancy leads to refusals, delays, and contributes to disease outbreaks and spread [29].
Attitude and uptake of vaccination by healthcare workers (HCW) is a significant determinant that is consistently associated with patient adherence and acceptance to vaccination and its schedules, which thus reduces vaccine aversion [2]. Vaccinated HCWs have been shown to have a noticeable effect on patients' decisions to take a vaccine. This will not be different in the case of the COVID-19 vaccine. Evidences showing that HCWs are being vaccinated can lead to greater acceptance and uptake by the general population [29].
In many African countries, COVID-19 vaccine misinformation spreading through multiple channels may present substantial obstacles to achieving coverage and herd immunity [21]. Anti-vaccination activists are already campaigning in multiple African countries against the need for a COVID-19 vaccine, with some denying the existence of the corona virus. People are inevitably exposed to misinformation, rumours and false conspiracy theories, which may erode their confidence in vaccination. In this era of 'Infodemics', developing trusted sources, fact-checking, and responding to misinformation by using trusted messengers outlets to help navigate the COVID-19 vaccine information landscape is crucial to prevent communities from forming negative opinions against them [1].
Religious fanaticism (related to one's own or one's groups' devotion to religion is an important factor in determining the likelihood of COVID-19 acceptability in African nations. Over the years, African communities have developed strong religious values that can be deemed to escalate into the concept of religious fanaticism. While major faith institutions typically endorse the principles around the public health goals of vaccination, hesitancy has been documented at an individual clergy level, and concerns have been raised across some religious organizations [31]. Over the past years, religious leaders have had enormous influence over their followers when it comes to attitudes towards public health interventions. Often, they have helped guide their followers in their health-seeking behaviours. Consequently, their pronouncements can significantly reduce or enhance the likelihood of vaccine acceptability and uptake. Nevertheless, some religious leaders have expressed concerns that followers may face an "ethical dilemma" over Africa's COVID-19 vaccination plan. To achieve an effective public health prevention response like COVID-19 vaccination, it is critical that religion and science flow in tandem, given that the role of religious leaders cannot be over-emphasized.
COVID-19 Immunization rollout plans for Nigeria need to consider factors such as the convenience of location and time, associated costs, as well as logistics associated with getting vaccinated. One key consideration that can enhance acceptability is ensuring that the vaccines "go to" the target populations and are readily accessible. Another challenge is the fact that roll-out plans will have to adopt strategies to target adults since typically, so far in the Nigeria context, vaccination campaigns have targeted children. Therefore, context-specific COVID-19 vaccination roll-out plans that are also convenient for the local populations will be very important for COVID-19 vaccination to be successful [12].
There is a need to harness social influencers, including trusted community figures like top performing artists, politicians, top sports individuals, top health officials, Presidents, Ministers and Nigerian celebrities [16]. It is important to establish a checklist of context-specific enabling environments for COVID-19 vaccination to be successful. This will equally involve making vaccine uptake "visible" to others, through health facilities in prominent public places, or by enabling ways for people to showcase that they have received the vaccine - on social media, in news media, or in person, and amplifying endorsements from trusted community members will increase gains in vaccine acceptability [29].
The landscape of COVID-19 infection, treatment and prevention are constantly changing. Many lessons have been learned but there is still a lot of information that is not unknown. How long immunity from natural infection and vaccination last, whether vaccines fully prevent the spread of infection, how well vaccines protect people with weak immune systems, long term effects of the vaccine, how the vaccines will fare long term in the face of a mutating virus are among questions that have not been fully resolved [32]. The devastation that COVID-19 has wrecked in our world so far is devastating, and until everyone is safe and protected, no one is safe. Many clinical experts were very pleasantly surprised by how well the vaccines work to prevent people from getting critically sick and/or dying from COVID. Real-world studies have continued to suggest that the vaccines are highly effective and so far, most of the side effects have been tolerable and short-lived [33].
There are numerous unanswered questions associated with SARS-CoV-2 immunity, specifically protective immunity. There is a necessity for different types of vaccines for differing populations such as infants and children, pregnant women, immune compromised individuals, as a majority of the vaccines under development are targeting the healthy population (18-55 years-old adults). A safe regulatory pathway must also be delineated for use of these vaccines in children, pregnant women, and immune compromised individuals. Recent outbreaks of pertussis and measles in countries where these diseases were formerly controlled demonstrated that the success of immunization programs cannot be taken for granted. Changes that occur over decades, such as lessened compliance with immunization or modifying the epidemiology of disease can overturn original assumptions about the impact of the vaccine. Post-marketing surveillance should also be continued to record adverse events [8].
To develop a safe and effective vaccine, pre-clinical trials must be done with caution to avoid severe adverse events. Moreover, cooperation between international organizations such as the WHO, CEPI, GAVI, and Bill and Melinda Gates Foundation is needed to ensure ample funding for vaccines. However, the efficacy of approved vaccines on the new mutant strains found in the United Kingdom and South Africa, are yet to be studied. The implementation of the first-generation vaccines could be achieved by pushing the nucleic acid-based priming vaccines followed by a booster dose of protein-based vaccines to rein in the mortality among high-risk communities. In parallel, more potent and efficient second-generation vaccines can be developed and manufactured to combat mutations in the virus [32].
A physical distance of at least 1 meter (3 ft) between persons is recommended by the World Health Organization (WHO) to avoid infection and CDC recommends maintaining a physical distance of at least 1.8 meters (6 ft) between persons. Public trust is important in promoting public health and plays an essential role in the public's compliance with vaccination programs and other health interventions. However, if the public trust is eroded, false information can spread, leading to the rejection of health interventions with a major threat to public health. It is also important that the Nigerian government should heighten its investment in effective and clear vaccine communication and community engagement. Also, national health authorities, stakeholders, and policymakers in Nigeria need to ensure that access to the COVID-19 vaccine is equitable as it becomes available. There is a need for health authorities in African nations to fully assess their health systems and the current levels of willingness to receive a potentially safe and effective COVID-19 vaccine. Public health officials and advocacy groups should focus on building vaccine literacy among the population and target groups to enhance its acceptability.