Introduction: Nearly 4 million cases of cholera are reported each year worldwide, including 189,000 (5 to 14%) in the Democratic Republic of Congo (DRC). The eastern provinces, known as "hot spots", report more than half of these cases.
Objective: Describe the epidemiological and diagnostic aspects of cholera in eastern DRC.
Methods: This is a cross-sectional, retro-prospective descriptive and analytical study of Vibrio cholerae (Vc) O1 isolates collected at the North Kivu provincial public health laboratory (AMI LABO) from January 1, 2011 to June 30, 2022.
Results: A total of 4,709 out of 17,443 suspected cholera cases have been confirmed, representing a prevalence of 26.99%. Only 4382 isolates fulfilled the inclusion criteria. The majority of samples (72.46%, n = 3175) came from the province of North Kivu. Half of the patients (51.5%, n = 2258) were male with a median age of 11 years [IQR: 4-25]. Children under 14 accounted for 57.8% of cases (2535/4382). Of the 3 serotypes isolated, the serovar Inaba was the majority (57.6%, n = 2522). Over 90% of 83 Vc Hikojima strains and 98.9% of 1777 Vc Ogawa strains were isolated between 2019 and 2022, making them emerging strains in the region. Very high levels of resistance were found to ampicillin (74.7%), nalidixic acid (83.8%), erythromycin (73.6%), chloramphenicol (68.8%) and Sulfamethoxazole/Trimethoprim (82%). On the other hand, quinolones (except nalidixic acid), macrolides (except erythromycin) and cyclins remained relatively sensitive.
Conclusion: Cholera remains a real public health problem in eastern DRC. Hence the importance of strengthening epidemiological surveillance, improving hygiene conditions and access to drinking water.
Epidemic, Cholera, Vibrio cholerae O1, Eastern Democratic Republic of Congo
Cholera is an acute, highly contagious, epidemic intestinal poisoning caused by a gram-negative bacterium called Vibrio cholerae [1]. Two main serogroups (O1 and O139) are currently responsible for the main cholera epidemics and pandemics in the world [2,3]. It is a faecal peril disease very often associated with natural disasters, wars and massive population displacements against a background of low socio-economic status [1,4]. It is a real public health emergency. According to the World Health Organization (WHO), approximately 1.4 to 4 million cases and 21,000 to 143,000 deaths are due to cholera [5]. Nearly 98% of these cases are concentrated in Africa, South Asia and Haiti [5-7]. Half of the cases and deaths occur in children under 5 years of age [5,8]. Although it is a notifiable disease, the WHO estimates that the number of officially reported cholera cases is only 5-10% of the actual number of cases worldwide. In 2020, the cholera pandemic coincided with the start of the COVID-19 pandemic (due to the SARS-CoV-2 virus). The extent of the impact of COVID-19 on the transmission, surveillance and reporting of cholera cases globally is not yet fully documented [5,9,10]. In the Democratic Republic of Congo (DRC), after several epidemics in the 1970s, cholera has become endemic in its eastern part since 1978 [11,12]. About 5 to 14% (189,000) of global cholera cases are reported in the DRC, more than half of them in the eastern provinces known as "hot spots". The DRC is therefore in the world's top five countries reporting more cases of cholera each year [9,13,14]. It is in this context that our study takes place, the main objective of which was to describe the epidemiological and diagnostic aspects of cholera in eastern DRCongo.
This is a cross-sectional, retro-prospective, descriptive and analytical study of Vibrio cholerae O1 isolates collected at the North Kivu provincial public health laboratory (AMI LABO) from January 1, 2011 to June 30, 2022. Were included in this study, all isolates positive for Vibrio cholerae O1 from the eastern provinces of the DRC. Samples with missing data were excluded.
Sampling being exhaustive. We therefore collected all the positive samples recorded in the laboratory during our study period. The data was collected from the "cholera" registers of the bacteriology department of the AMI LABO laboratory using a standard collection sheet including socio-demographic characteristics (age, sex, geographical origin, period) and biological (type sampling, culture, serogrouping, serotyping, biotyping).
Culture and identification of strains of Vibrio cholerae O1 were made from freshly passed stool samples. These were made in sterile, leak-proof, well-labeled vials and transported to the laboratory in Cary-Blair transport medium. The strains of Vibrio cholerae were cultured on TCBS nutrient agar, enriched in a liquid medium with alkaline peptone water and incubated at 37 °C for 18 to 24 hours. Morphological, biochemical and serogroup characterizations were then performed according to conventional bacteriological techniques and standard protocols [15-17]. Antibiograms were performed on isolates using the Kirby-Bauer disk diffusion method with Mueller Hinton agar.
Data were entered into Microsoft Excel software and analyzed using R version 4.0.3 software. Categorical variables were described as relative and absolute frequencies. As for the quantitative variables, they were presented in the form of mean ± standard deviation or median depending on the type of distribution. A bivariate analysis was determined using Fisher- Freeman-Halton's exact test and Pearson's chi-square. Values of p < 0.05 were considered statistically significant.
This study obtained the authorization of the steering committee in charge of training and research within the provincial public health laboratory of North Kivu AMI LABO where the study was carried out.
Over a period of 11 years and 6 months, from January 1, 2011 to June 30, 2022, we collected 4709 isolates of Vibrio cholerae O1 out of a total of 17443 stool samples from suspected cholera subjects from six provinces located in the Eastern DRC: North Kivu, South Kivu, Maniema, Tanganyika, Lomami and Kasaï Oriental, then analyzed at the AMI LABO laboratory, i.e. a prevalence of 26.99%. Only 4382 isolates were retained for this study. The flow diagram illustrates the selection process according to the inclusion and non-inclusion criteria previously defined (Figure 1).
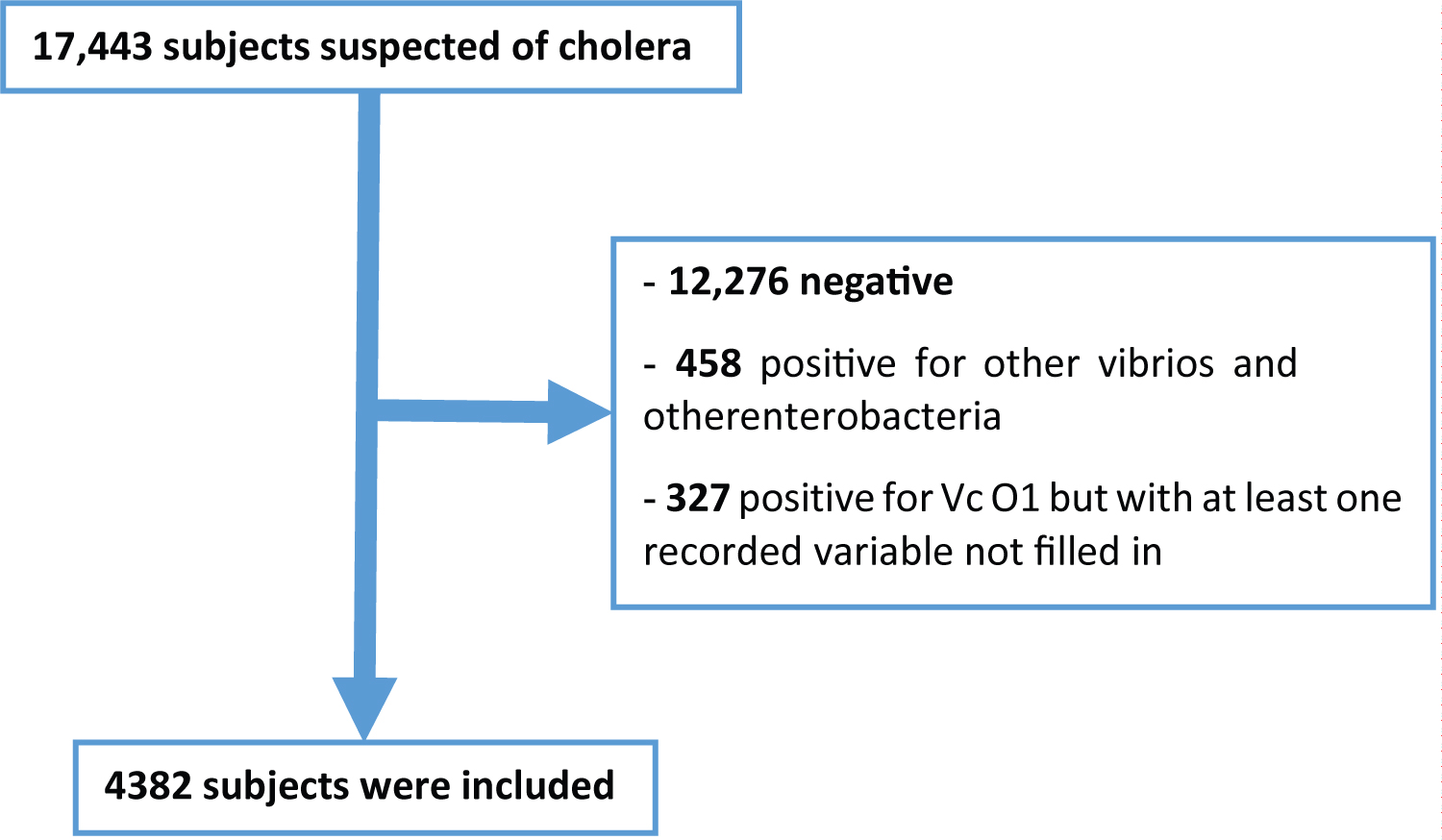 Figure 1: Recruitment flow diagram of Vibrio cholerae O1 isolates at the North Kivu provincial public health laboratory AMI LABO during cholera epidemics in eastern DRC from January 1, 2011 to June 30 2022.
View Figure 1
Figure 1: Recruitment flow diagram of Vibrio cholerae O1 isolates at the North Kivu provincial public health laboratory AMI LABO during cholera epidemics in eastern DRC from January 1, 2011 to June 30 2022.
View Figure 1
Slightly more than half (51.5%, 2258/4382) of the patients were male (sex ratio M/F = 1.06). The median age was 11 years [IQR: 4-25]. The age group from 5 to 14 years was the most affected (30.7%, 1347/4382) followed by that from 0 to 4 years (27.1%, 1188/4382). Children aged 0 to 14 alone accounted for more than half of the cases with a total of 57.8% (n = 2535). More than half (72.46%, 3175/4382) of the patients came from the province of North Kivu. Table 1 summarizes this distribution.
Table 1: Sociodemographic characteristics of patients with cholera confirmed at the North Kivu provincial public health laboratory AMI LABO, collected in eastern DRC from January 1, 2011 to June 30, 2022 (n = 4382). View Table 1
Compared to the study period, half of the 4,382 cases (51%) were identified in 2011, with a transient drop to 17% in 2020 and 16% in 2021, then a rise to 26% in the first half alone. of the year 2022 (Figure 2).
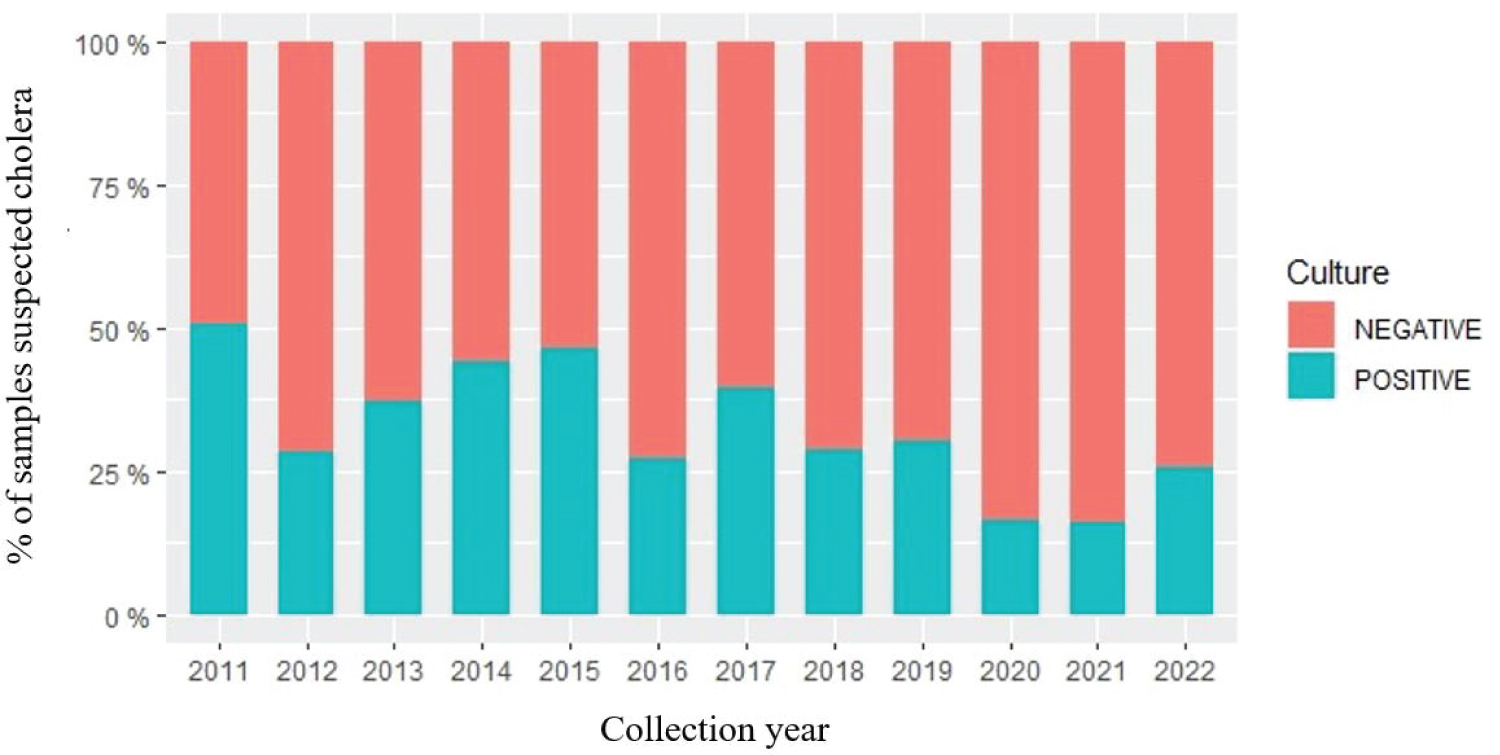 Figure 2: Distribution by year of cholera cases collected in eastern DRC and recorded at the North Kivu provincial public health laboratory AMI LABO from January 1, 2011 to June 30, 2022 (n = 4382).
View Figure 2
Figure 2: Distribution by year of cholera cases collected in eastern DRC and recorded at the North Kivu provincial public health laboratory AMI LABO from January 1, 2011 to June 30, 2022 (n = 4382).
View Figure 2
Among the 4382 strains of Vibrio cholerae O1 isolated, all (100%) were the El Tor biotype and all 3 serotypes were found, the majority of which was serovar Inaba (57.6%) (Figure 3).
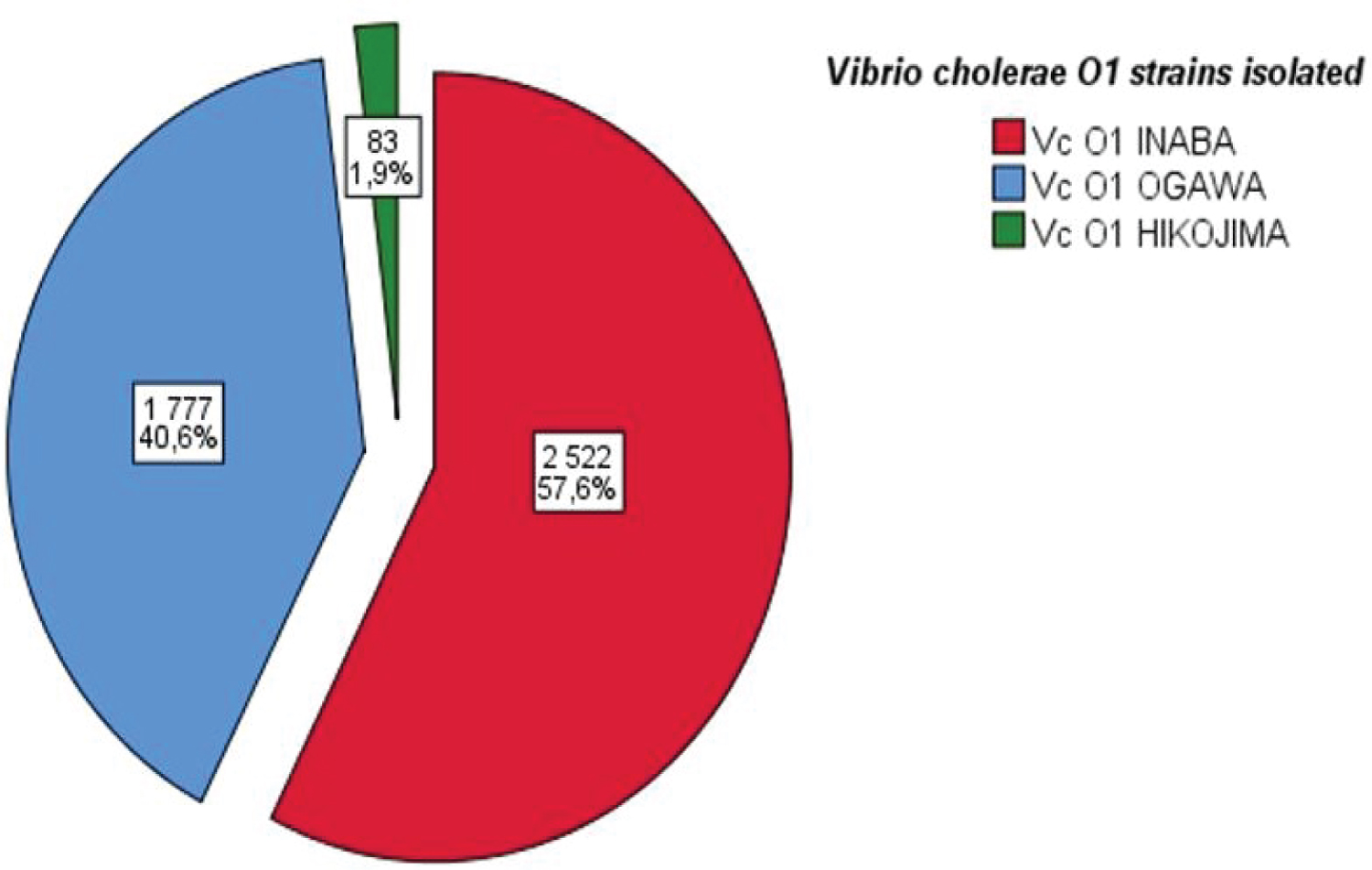 Figure 3: Distribution according to identification by strain (serotype), of isolates of Vibrio cholerae O1 collected in eastern DRC and recorded at the provincial public health laboratory of North Kivu AMI LABO from January 1, 2011 to June 30, 2022 (n = 4382).
View Figure 3
Figure 3: Distribution according to identification by strain (serotype), of isolates of Vibrio cholerae O1 collected in eastern DRC and recorded at the provincial public health laboratory of North Kivu AMI LABO from January 1, 2011 to June 30, 2022 (n = 4382).
View Figure 3
As shown in Table 2 and Figure 4, the distribution of the different strains of Vibrio cholerae O1 isolated (serotypes) during this study was statistically dependent on the age, sex and province of origin of the patients (p < 0.001, p = 0.040 and p < 0.001 respectively), as well as a change over time (p = 0.000).
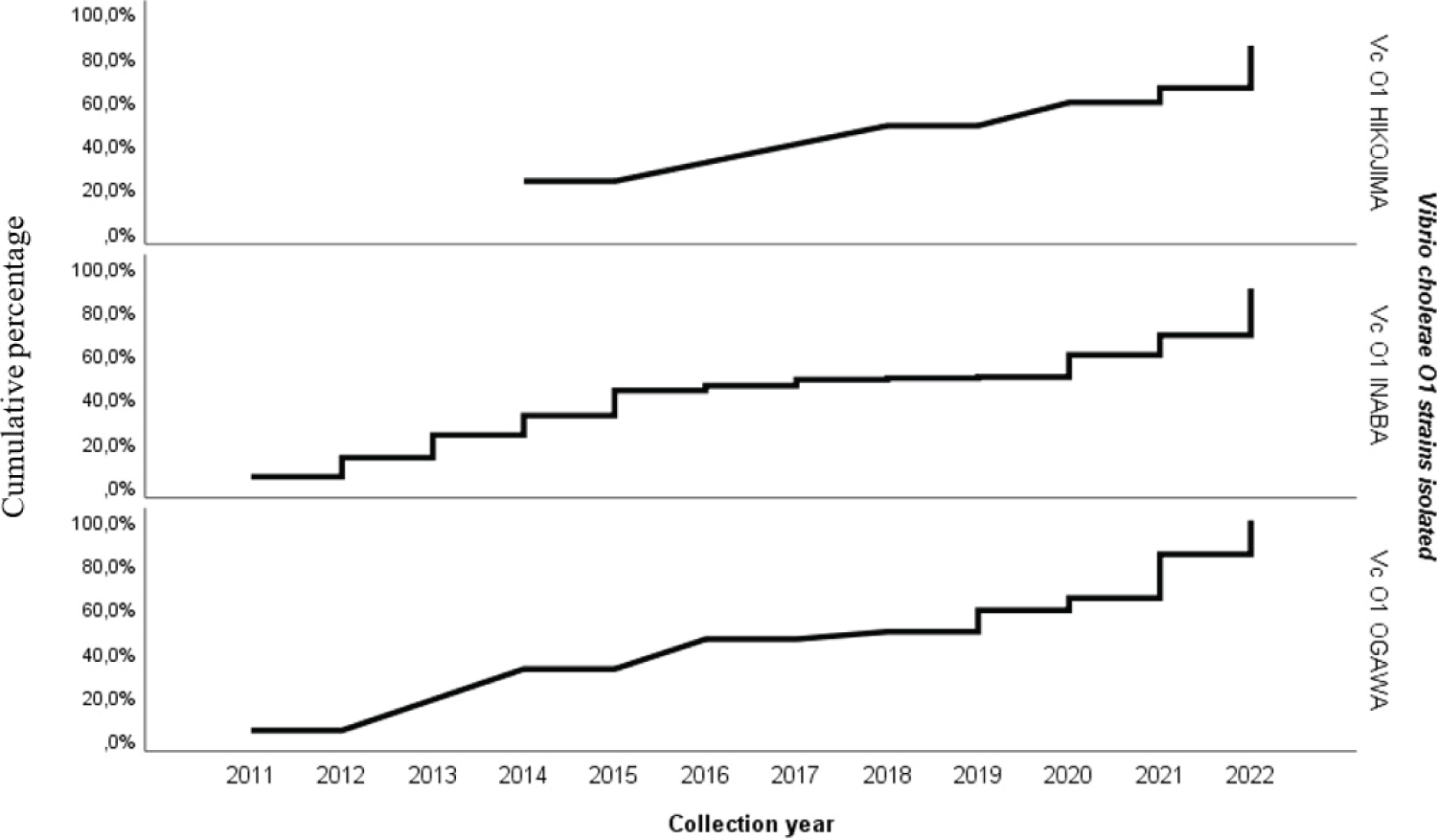 Figure 4: Isolation trend of the 3 strains of Vibrio cholerae O1 over time, during cholera epidemics in eastern DRC from January 1, 2011 to June 30, 2022 (n = 4382).
View Figure 4
Figure 4: Isolation trend of the 3 strains of Vibrio cholerae O1 over time, during cholera epidemics in eastern DRC from January 1, 2011 to June 30, 2022 (n = 4382).
View Figure 4
Table 2: Variations of Vibrio cholerae O1 serotypes isolated according to age, sex and geographical origin (Province), in eastern DRC between January 2011 and June 2022 (n = 4382).View Table 2
The majority of Vibrio cholerae O1 strains isolated in this study were resistant to ampicillin (74.7%), nalidixic acid (83.8%), chloramphenicol (68.8%) and sulfamethoxazole/trimethoprim (82%). On the other hand, quinolones (except nalidixic acid), macrolides (except erythromycin) and cyclins remained relatively sensitive (Table 3).
Table 3: Distribution of susceptibility profiles of isolated Vibrio cholerae O1 strains to ten antibiotics tested (n = 4382). View Table 3
The prevalence of cholera in our study was 26.99%. In Senegal, Ndour CT, et al. [18] reported a lower prevalence than ours, i.e. 18.8% during the 2004-2005 cholera epidemic in Dakar, probably related to the short duration of the study. Whereas, Dengo-Baloi LC, et al. [19] reported a prevalence close to ours (33.5%) in Mozambique between 2012 and 2015. The majority of cholera cases (363 out of 1093, i.e. 33.2%) from the series of Miwanda B, et al. [7] in the DRC between 1997 and 2012 came from the province of North Kivu. This corroborates our study in which more than half (72.46%) of our patients came from the province of North Kivu. From January 1, 2011 to June 30, 2022, eastern DRC reported cases of cholera continuously. We observed nearly 50% of positive cases in 2011 and 2015, then a temporary drop in cases was noted between 2020 and 2021 (17 and 16% respectively) before doubling in the first half of 2022 alone (681 case, i.e. 26%). These results can be superimposed on those of Muyembe JJ, et al. [9] who showed that, between 2000-2011, the annual incidence of cholera in the DRC was highest in the eastern provinces bordering the Great Lakes.
They add that nearly 50% of cholera cases reported in Africa come from the Great Lakes regions. The WHO for its part reports that the eastern provinces of the DRC are said to be "hot spots" of cholera containing more than half of the cases of cholera in the country [8,13]. This fluctuating prevalence of cholera found in our study could be explained on the one hand by the persistence of armed conflicts for several decades in this part of the country, leading to massive population movements, thus increasing promiscuity and exacerbating the precariousness linked to bad water, hygiene and sanitation conditions, and on the other hand by a low socio-economic level of the population as well as a lack of access to care and sanitary infrastructures. This thesis is supported by several other authors [9,20-22]. For their part, Batumbo Boloweti D, et al. [22], in their recent study published in 2020 demonstrated that volcano-tectonic activity in the province of North Kivu would control cholera epidemics in the East African Rift. All this could also explain the predominance of cases in the province of North Kivu in particular, but also naturally by the fact that our research setting is located in this province.
In addition, the year 2020-2021 coincides with the emergence of the COVID-19 pandemic having impacted all health systems and thus could explain a low notification of cases on the one hand, but also the restriction measures (covers fire, social and physical distancing) and the strengthening of hygiene measures could promote a drop in cholera cases on the other hand. This corresponds to the data reported in 2020 by the WHO and the GTFCC [5]. Furthermore, the overall prevalence of cholera reported in our study could be underestimated due to the under-reporting of several cases as mentioned in the report on the multisectoral strategic plan for the elimination of cholera in the DRC between 2018 and 2022 [23]. The WHO, for its part, estimates that only 5 to 10% of cholera cases occurring each year are officially reported [5].
According to the WHO, children under 5 are the most affected by cholera, but all age groups are affected [24]. More than 60% of cholera cases in the series by Ousmane Moussa T, et al. [25] in Mali involved children under 5-years-old. On the other hand, in their series, Doudou Tubaya d, et al. [26], in 2007 in Lubumbashi in the DRC and Ndour CT, et al. [18], in 2004-2005 in Dakar- Senegal, had respectively reported a predominance of the male sex (59 % and 60%) with an average age of 21.9 ± 17 years and 30 ± 17 years with a predominance of the 10 to 29-year-old bracket (50%). In our series, children under 15 alone represented more than half of the cases (57.8%) with a median age of 11 years [IQR: 4-25]. Those under 5-years-old accounted for 27.1%. The male gender was slightly predominant (51.5%) with a sex ratio of 1.06. This predominance of cholera in children under 15 reflects their fragility and increased exposure to the disease.
Anticholera immunity would also play a role in this context, as demonstrated by several recent studies [27-32]. On the other hand, sex has hardly any particularity during a cholera epidemic and its frequency in our series could be explained by the men's capacity for mobility, which would thus favor their contamination; but also professional activities including fishing in this part of the Great Lakes with a tendency to risk consuming water and/or fish products, food contaminated by Vibrio cholerae. In the study by Bompangue, et al. [21] on the dynamics of cholera epidemics in the African Great Lakes region, the case of the DRC, more than 90% of the subjects were fishermen (more than two out of three). In November 2020, Togo reported that 19 out of 67 cholera cases (28%) were fishermen with a M/F sex ratio of 1.48 [33].
On the other hand, Lamond E and Kinyanjui J [34], in their report published in 2012 on guidelines for cholera epidemics, believe that women are more exposed than men, because they are the most often carers of sick in the household and they do not necessarily know the precautions to take to avoid transmission.
Serogroups O1 (classical and El Tor biotypes) and O139 are the main pathogens involved in cholera epidemics. Serogroup O1 strains are classified into three serotypes (Ogawa, Inaba and Hikojima) and are responsible for the majority of cholera cases [35]. In Mozambique, out of 1522 stool analyzes suspected of cholera carried out between 2012 and 2015, Dengo-Baloi LC, et al. [18] reported 510 strains of Vibrio cholerae O1 El Tor serotype Ogawa. Similarly, 97.1% of the Vibrio cholerae O1 strains in the series by Mandal J, et al. [36] in India between 2008 and 2010 were of the Ogawa serotype against only 2.9% of the Inaba serotype. On the other hand, all the isolates of Vibrio cholerae O1 in the series of Chandralekha C, et al. [37] were of the El Tor biotype and the Hikojima serotype. No other serotypes were found in this study.
In our series, out of 100% of the stool samples taken, which made it possible to isolate 4382 strains of Vibrio cholerae O1 of the El Tor biotype, Inaba (2522 cases, i.e. 57.6%) and Ogawa (1777 cases, i.e. 40.6 %) were the two most common serotypes. As for the Hikojima serotype, it accounted for only 1.9% of cases (83 out of 4382 cases). However, in a study looking at the genetics of Vibrio cholerae LPS, it was shown that an O1 strain can frequently switch from one serotype to another during a single outbreak. This reduces the epidemiological interest of serotype determination [35]. On the other hand, some studies have reported that the Hikojima serotype is known to be very unstable and has been shown to interconvert and undergo serotype switching [38]. Our study therefore suggests the value of close monitoring and surveillance of the prevalent serotype.
Antibiogram results revealed very high resistance levels of Vibrio cholerae O1 strains to ampicillin (74.7%), nalidixic acid (83.8%), erythromycin (73.6%), chloramphenicol (68.8%) and sulfamethoxazole/trimethoprim (82%). The molecules recommended by the WHO (macrolides, quinolones, cyclins) [39] remained relatively sensitive, but with some strains resistant to certain first- or second-line molecules. Several authors have reported almost concordant results [22,40,41]. Thus, the importance of the antibiogram in the face of any cholera epidemic is no longer debatable and is essential with a view to good early management of serious cases and early detection of resistant strains in order to best adapt the disease antibiotic therapy.
The distribution of the 3 serotypes of Vibrio cholerae O1 isolated in our study was statistically dependent on the age (p < 0.001), sex (p = 0.040) and province of origin (p < 0.001) of the patients.
Among the 83 Hikojima serotype strains, the majority (30.1%) proportionally affected children under 5-years-old and subjects ≥ 25-years-old, including 56.6% males (sex ratio of 1.3) from mostly from the province of South Kivu (53/83, or 60.2%). As for serovar Inaba, it was found more in female subjects (1263/2522, or 50.1%) aged ≥ 25 years (749/2522, or 29.7%) and the majority of them (2134/2522, or 84.6%) came from the province of North Kivu. In addition, the Ogawa serovar remained predominant (581/1777, or 32.7%) in male children aged 5 to 14 years (952/1777, 53.6%). This heterogeneous distribution of the different strains encountered in our study could be partly explained by the fact that the majority of our samples came from the province of North Kivu (3175/4382 cases, or 72.46%). However, the Hikojima serovar being described as most often an environmental strain, would explain its predominance in adults aged ≥ 25 years, mostly men because of their mobility and activity, and easily contaminate those under 5 years of age. Similar results have been reported by Slathia P, et al. [42], as well as Chandralekha C, et al. [37]. In many African countries, Vibrio cholerae O1 serotype Ogawa has been the strain most frequently isolated and associated with cholera epidemics [41].
In addition, our study also showed that the different strains of Vibrio cholerae O1 isolated were statistically related to a time course (p = 0.000) with an emergence of Hikojima serovars (from 0% during the first 7 years of the study at nearly 90% between 2021 and 2022) and Ogawa (from less than 2% in the first 5 years to 99.2% between 2018 and 2022). This corresponds to the data published by the WHO on the emergence of cholera cases in Africa, particularly in "hot spot" areas, thus recommending combined environmental and clinical surveillance [43,44].
Furthermore, it has been shown that the Hikojima serotype is also a transitional form between the first two serotypes, rare and unstable and can be observed when a strain undergoes a serotype change from Ogawa to Inaba and does not occur in the nature [45].
This study has enabled us to observe that, despite the multiple efforts implemented to prevent cholera epidemics in the Democratic Republic of Congo (DRC), the eastern part of the country is still one of the hot spots for cholera epidemics. The latter remain a major public health problem becoming a real clinical landscape in the DRC. All 3 serotypes were found with a heterogeneous distribution in the eastern provinces of the DRC, North Kivu being the most affected province. The persistence of armed conflicts leading to massive population movements, the difficulties of access to drinking water, the high population density would favor among other things this emergence of cholera. Children under 14 are the most affected by this disease, with a peak in those under 5 due to their fragility and increased exposure to the disease. This therefore requires the implementation of sustainable interventions linked to the improvement of access to drinking water, hygiene and sanitation conditions in the areas affected by cholera epidemics (endemic and epidemic) at the level support structures and the community. A prioritization of operational research aimed at improving cholera control strategies, namely geopolitical studies of epidemics (Governance and management of cholera epidemics, conflicts, population movements and cholera dynamics), socio-anthropological and impact studies economic development is also necessary in order to prevent epidemics and reduce the prevalence of this disease in this part of the DRC.
The authors declare no conflict of interest.
Authors have not received any financial support from any organization or individual.
The authors are grateful to all the staff of the public health laboratory of North Kivu AMI LABO for having actively participated in this study and allowing it to be carried out in complete peace of mind.
This study presented some limitations: first we noted the absence of clinical data from patients since the study was carried out in the laboratory; then the absence of data on the methods of contamination of our patients, which could allow a good targeted strengthening of the management of cholera cases.