Background: Reporting of hepatitis C virus (HCV) ribonucleic acid (RNA) test results is a critical public health activity to facilitate the elimination of HCV. Comprehensive surveillance of both positive and negative HCV RNA test results is essential to informing and monitoring public health strategies for HCV elimination.
Methods: To get the most up-to-date information on the reporting requirements of HCV RNA test results for all fifty states in the United States (US) and Washington, DC (which will be referred to as "states" henceforward), we examined sources like state HCV reporting guidelines and HCV case report forms. For states that we could not find information on, we contacted via email and/or phone call sources like state-based HCV senior epidemiologists and HCV surveillance managers.
Results: Ultimately, we found that ~98% of states require reporting of positive HCV RNA test results, but only ~53% of states require reporting of negative HCV RNA test results.
Conclusion: All states should have requirements for the reporting of positive and negative HCV RNA test results.
Hepatitis C Virus (HCV), HCV surveillance, HCV RNA test results, HCV elimination
HCV: Hepatitis C Virus; RNA: Ribonucleic Acid; US: United States; CDC: Centers for Disease Control and Prevention
It is estimated that 2.5-4.7 million people in the US live with an HCV infection [1]. A more robust estimate of the prevalence of HCV infection in the US is not yet feasible. One reason for that is that not all states require positive and negative HCV RNA test results to be reported. A positive HCV RNA test result indicates a current infection, while a negative HCV RNA test result indicates a past infection that was treated or spontaneously cleared.
The Centers for Disease Control and Prevention (CDC) recommend both positive and negative HCV RNA test results be reported to local public health departments [2]. While the required reporting of positive HCV RNA test results has been in place for years, only recently have states moved towards requiring the reporting of negative HCV RNA test results. A recent survey of 43 US health jurisdictions found that 17 of them (40%) required negative HCV RNA test results to be reported [2]. 12 jurisdictions (28%) received negative HCV RNA test results, but they did not require this reporting [2]. Some were in the process of updating local laws or regulations to do so [2].
In this study, we collected information on the reporting requirements of HCV RNA test results for all states.
To determine the frequency and distribution of reporting requirements of HCV RNA test results in the US, we used various sources. First, we examined state HCV reporting guidelines published on state department of public health websites as well as available HCV case report forms and HCV strategic plans. For states that we could not find web-based information on, we contacted state-based HCV senior epidemiologists, HCV surveillance managers, viral hepatitis prevention coordinators, or HCV nursing program coordinators via email or telephone. After obtaining information on the reporting requirements of HCV RNA tests results from all states, we categorized each state into one of three categories: 1) Requires the reporting of positive and negative HCV RNA test results, 2) Requires the reporting of only positive HCV RNA test results, and 3) Does not require the reporting of either positive or negative HCV RNA test results.
Finally, we visualized the distribution of reporting requirements across the US using Map Chart ( https://www.mapchart.net/usa.html ).
Figure 1 depicts the HCV RNA reporting requirements for all states. The proportion of states that require positive HCV RNA test results to be reported is ~98% (50/51). Idaho is the only state that does not require any HCV RNA test results to be reported. The proportion of states that require negative, in addition to positive, HCV RNA test results to be reported is ~53% (27/51).
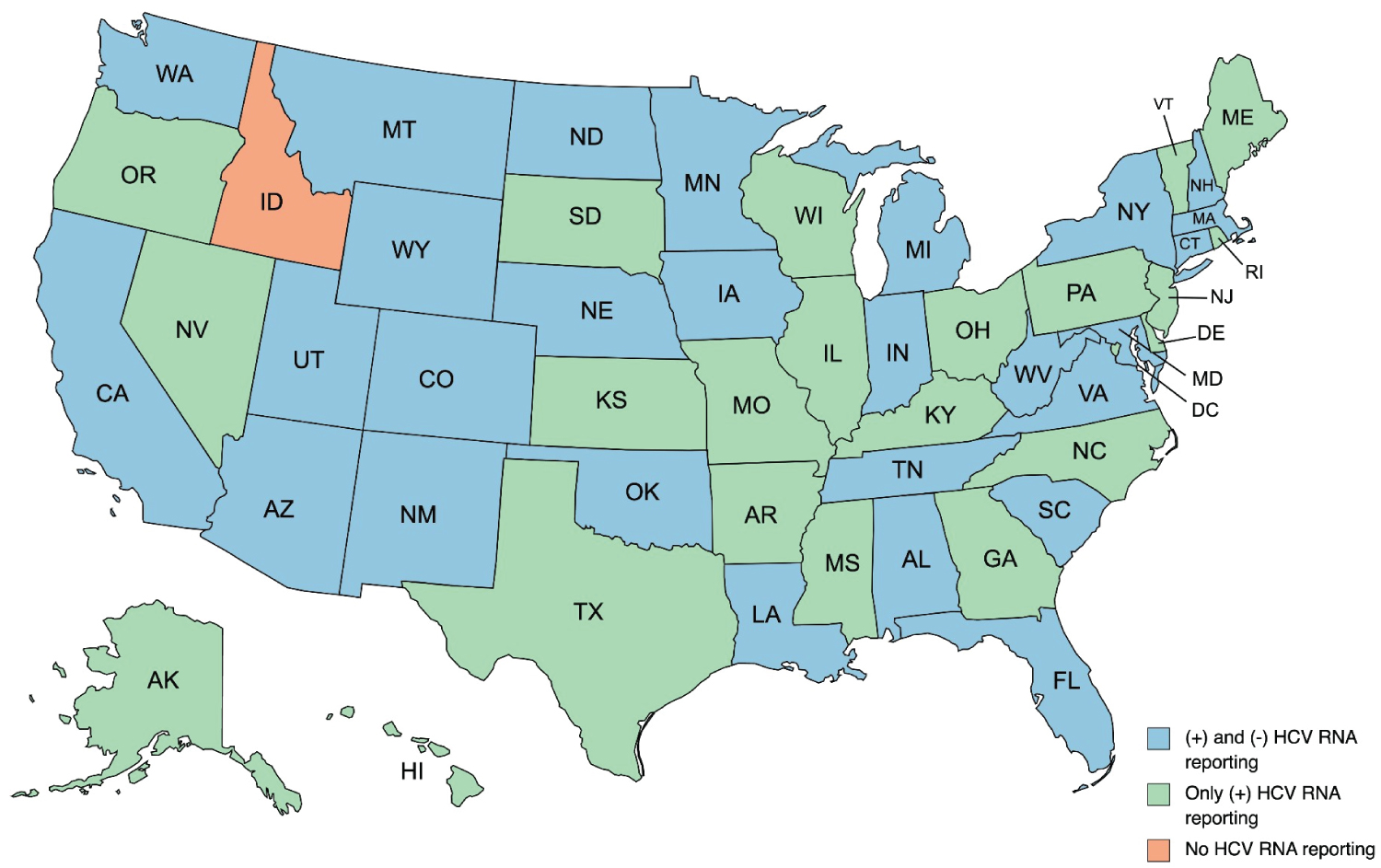 Figure 1: Reporting requirements of HCV RNA test results for all fifty US states and Washington, DC (as of April 2023).
View Figure 1
Figure 1: Reporting requirements of HCV RNA test results for all fifty US states and Washington, DC (as of April 2023).
View Figure 1
It is encouraging to see that almost all US states require reporting of positive HCV RNA test results. However, only about half of the states require negative HCV RNA test results to be reported.
Some states that require only positive HCV RNA test results to be reported are planning to update regulations so that negative HCV RNA test results can be reportable. For example, Hawaii and Kansas are at this stage. We recommend that each state that does not require negative HCV RNA test results to be reported seek local technical assistance from state epidemiologists in the Council of State and Territorial Epidemiologists as soon as possible in order to update reporting requirements so that they are consistent with the CDC’s recommendations.
Making negative HCV RNA test results reportable could help in planning better ways to meet the US’s target of HCV elimination by 2030 [3]. Only three states (Connecticut, South Carolina, and Washington) are on track to achieve elimination by 2030 [4]. Without the required reporting of negative HCV RNA test results, the true number of active HCV infections is unknown. It is not possible to determine which people with a history of a positive HCV RNA test result have resolved their infection either spontaneously or with treatment. A more accurate number of infections can help states respond with interventions targeted to specific populations or geographic areas to get closer to HCV elimination. In addition, having negative HCV RNA test results reportable increases awareness regarding acute infections, both new and re-infections, and completeness of testing programs [2]. Even localities performing HCV case management, where public health staff contact reported cases regarding their positive RNA test result [5], benefit from the required reporting of negative HCV RNA test results. A negative HCV RNA test result, which identifies a case as treated or spontaneously cleared, saves public health staff time and resources from performing unnecessary case management. Finally, given the increasing incidence of acute HCV cases that are related to the ongoing opioid epidemic [6] implementing the reporting of negative HCV RNA test results can help identify populations of people who inject drugs that are accessing treatment and not accessing treatment. Treating HCV in people who inject drugs is time-sensitive, as left untreated, one active injector can infect up to twenty others with HCV within the first three years of infection [7].
In summary, we have found that the required reporting of positive HCV RNA test results is widespread, but the required reporting of negative HCV RNA test results is lagging. For an accurate estimate of the prevalence and incidence of HCV in the US, both positive and negative HCV RNA test results should be reportable. In light of increased efforts toward the national elimination of HCV, an accurate estimate would be essential to inform public health planning and policy development.
N/A.
All authors have contributed equally.