Pituitary apoplexy followed by cerebral ischaemia is very rare and life-threatening clinical syndrome. Ischemia is a rare complication after pituitary apoplexy. Cerebral ischemia due to pituitary apoplexy has been linked to two mechanisms; this can occur through one of two mechanisms-direct compression of the artery or vasospasm caused by vasoactive factors/agents released from haemorrhagic or necrotic material of the pituitary adenoma.
A 42-year-old male patient with known chronic myeloid leukemia (CML) disease presented to our clinic with vomiting, severe headache which started about 3 days earlier and visual impairment. The cranial MRI with multiplanar and multi sequencies obtained specifically for the pituitary gland Pre-Post gadolinium contrast showed an enlarged sella turcica with large sellar and suprasellar heterogenous mass lesion. Patient underwent transsphenoidal excision of the pituitary tumor. The second day after operation the patient had severe headache and became confused. An emergency cranial CT scan was perfomed and demonstated massive hypodensity areas in the right temporal and frontoparietal lobes, which suggested a decrease in perfusion as well as right side global brain edema and ischemic infarct.
Although, clinicians focus on visual disturbance and endocrine problems in pituitary apoplexy, should be kept in mind that patients may have cerebral infarction in different regions with the effect of vasospasm and we should be aware of this aspect.
Cerebral infarction, Pituitary apoplexy, Vasospasm, Cerebellar ischeamia, Decompressive craniectomy, Chronic myeloid leukemia
Pituitary apoplexy is a rare, life-threatening clinical syndrome characterised by sudden onset of headache, vomiting, visual disturbance, ophthalmoplegia and sometimes altered consciousness [1].
Ischemia is a rare complication after pituitary apoplexy. Cerebral ischemia due to pituitary apoplexy has been linked to two mechanisms; this can occur through one of two mechanisms-direct compression of the artery or vasospasm caused by vasoactive factors/agents released from haemorrhagic or necrotic material of the pituitary adenoma [2,3].
We report the case of cerebral and cerebellar infarct after pituitary apoplexy caused by vasospasm and vasoactive agents released rather than direct vascular compression.
A 42-year-old male patient with known chronic myeloid leukemia (CML) disease presented to our clinic with vomiting, severe headache which started about 3 days ago and visual impairment. The neurological examination was intact with GCS 15/15. The left eye seeing was blurred. The fundoscopic examinatin revealed normal optic discs. The pupils were isochoric, 2/2 with positive light reaction.
The plain cranial computed tomograghy (CT) scan done and demonstrated a large sellar and suprasellar with intrinsic hemorrahage mass lesion measuring 28 × 38 × 21 mm (Figure 1). The hemmorhagic pituitary mass made us thinking about Pituitary Apoplexy so we planned for cranial magnetic resonance ımaging (MRI). The cranial MRI with multiplanar and multi sequencies obtained specifically for the pituitary gland Pre-Post gadolinium contrast showed an enlarged sella turcica with large sellar and suprasellar heterogenous mass lesion showing figure of snowman in the coronal images (Figure 2).
 Figure 1: Sagittal CT scan showing a large sellar and suprasellar with intrinsic hemorrahage mass lesion.
View Figure 1
Figure 1: Sagittal CT scan showing a large sellar and suprasellar with intrinsic hemorrahage mass lesion.
View Figure 1
 Figure 2: a) T2-weighted MRI showing figure of snowman in the coronal image; b) T1-weighted coronal MRI showing a mixed intensity enhancing intrasellar mass.
View Figure 2
Figure 2: a) T2-weighted MRI showing figure of snowman in the coronal image; b) T1-weighted coronal MRI showing a mixed intensity enhancing intrasellar mass.
View Figure 2
According to patient's medical background of Chronic myeloid leukemia we consulted hematologists for the early operation, we got the permission for operation with platelets replacement. The patient had been diagnosed with CML for 4 years and was using imatinip. In the examinations performed before the operation, the number of white blood cells was 17530/μL, and the number of platelets was 53 × 103/μL . DIC screen panel PT: 15.5 PTT: 28.4 INR: 1.4. In additıon, since cortisol level was 9.6 in basal hormones checked preoperatively, dexamethasone was initiated by endocrinology. The patient underwent transsphenoidal excision of the pituitary tumor. At the surgery the tumor was necrotic and hemorrhagic by appearance. Histological examination of the specimen revealed diffuse necrosis and hemorrhagic infarcts in the pituitary adenoma, compatible with pituitary apoplexy. Leukemic infiltration was not seen.
The second day after operation the patient had severe headache and became confused. GCS dropped to 12/15. An emergency cranial CT scan was perfomed and demonstated massive hypodensity areas in the right temporal and frontoparietal lobes, which suggested a decrease in perfusion as well as right side global brain edema and ischemic infarct (Figure 3). As the patient's neurologic condition was deteriorating we perfomed an emergency rightside cranial decompression. Mannitol treatment was applied to the patient for brain edema. The blood test results after first operation didnt show the very high number of leukocytes, 40,000/μL (leukocytosis) to cause thrombosis as the patient had CML. Increase of leukocytes is frequent after surgery. Nevertheless, flow cytometry was performed by consulting the patient with hematology. In flow cytometry, an atypical cell group with a total of 90% localized CD34/CD117 blast was found on CD45. The patient admitted in the blast phase of CML. After the operation the patient didnt recover soon and remained under ventilator support. The patient's neurological examination continued to deteriorate. We perfomed cranial CT scan and suprisingly observing both massive cerebral and cerebellar infarcts (Figure 4). This strongly suggests that rather than direct vascular compression by the tumor there must be other strong vasoactive agents secreted by the tumor itself which leads to massive vasospasms. In the postoperative period, fresh frozen plasma and nimodipine were given to the patient for the treatment of vasospasm.
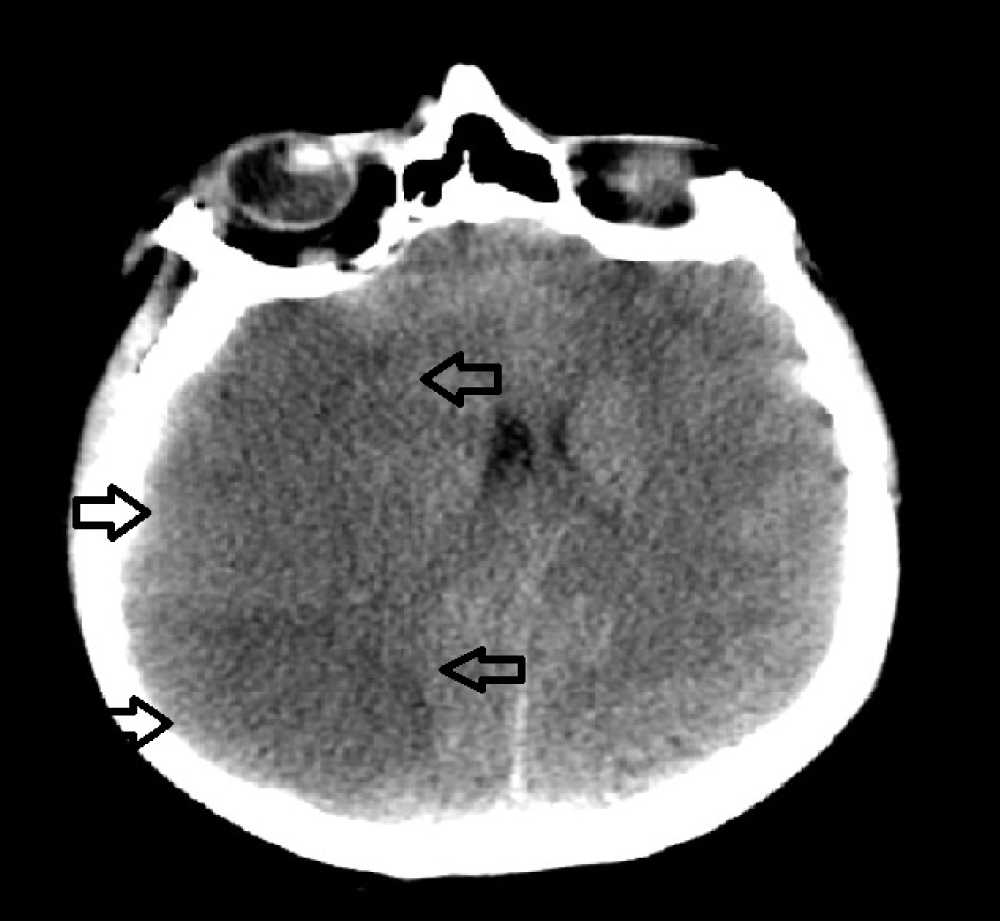 Figure 3: Post-operative axial CT scan showing right temporoparietal infarcts and brain edema.
View Figure 3
Figure 3: Post-operative axial CT scan showing right temporoparietal infarcts and brain edema.
View Figure 3
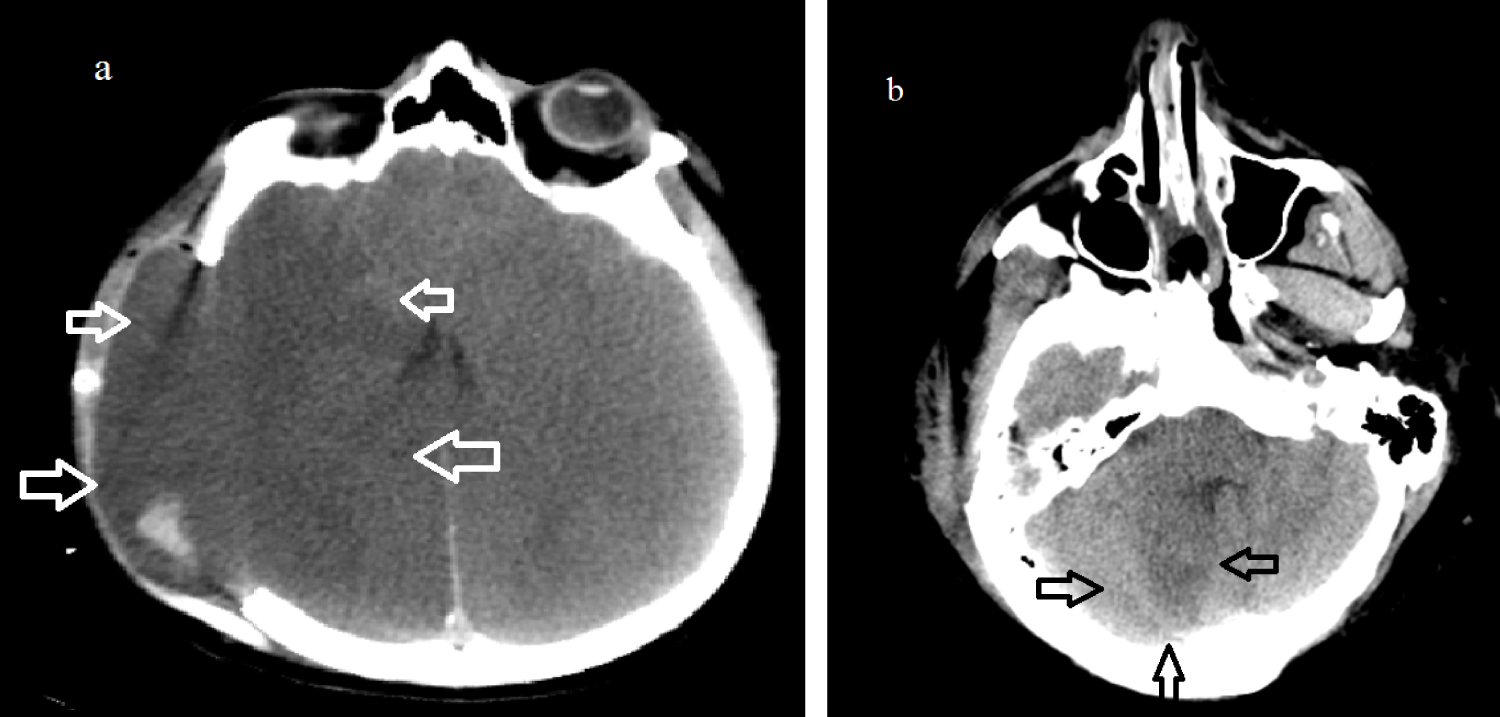 Figure 4: a) Axial CT scan showing massive right temporoparietal infarcts after cranial decompression; b) CT scan showing low density area in the right cerebellar.
View Figure 4
Figure 4: a) Axial CT scan showing massive right temporoparietal infarcts after cranial decompression; b) CT scan showing low density area in the right cerebellar.
View Figure 4
The patient's Kidney function tests were not good enough so we could not perfom neither digital subtraction angiography (DSA) nor Contrast enhanced CT Angiography to prove vasospasm. The preoperative creatinine value of 1.04 mg/dL was measured as 4.42 mg/dL in the postoperative period. Due to massive cerebral edema the patient was receive mannitol treatment. Therefore, the patient was considered as acute renal injury.
Hence we perfomed MR Angiography which showed massive vasospasm on both anterior and posterior circulation of brain blood vessels (Figure 5).
 Figure 5: MR Angiography showing massive vasospasm due to the absence of both anterior and posterior circulation of the cerebral blood vessels.
View Figure 5
Figure 5: MR Angiography showing massive vasospasm due to the absence of both anterior and posterior circulation of the cerebral blood vessels.
View Figure 5
In spite of providing the required treatments for vasospasm our patient died five days later after cranial decompression surgery.
Pituitary apoplexy is a life threatening clinical condition with reported incidence of 0.6-22% [4]. Pituitary apoplexy is the process where hemorrhage occurs within a pituitary adenoma due to excessive tumor infarction. It can be symptomatic causing headache, acute visual disturbances or disturbed conscious level, or asymptomatic [5]. Pituitary apoplexy complicated by cerebral infarction is a rarely reported condition, currently only 25 cases have been reported in the literature [6]. In apoplexy, two possible mechanisms are emphasized, one of which is ischemia due to cerebral artery occlusion [7,8]. The other is vasospasm which may be caused by the release of potent vasoactive agents or as a result of subarachnoid hemorrhage [9]. In suprasellar tumors, hypothalamic damage may also occur with liberation of spasmogenic factors from the damaged hypothalamic tissue [10]. Pozzati, et al. attributed vasospasm in their patient to vasoactive substances liberated from the pituitary tumour, as the vasospasm was very different from that seen in subarachnoid haemorrhage [9]. Ahmed, et al. reported two pituitary apoplexy cases with cerebral ischemia due to both compression and vasospasm [2] Abbas, et al. showed that mechanism of injury by a pituitary apoplexy which is the bilateral streching and compression of the ACA, causing irreversible cerebral ischemia of the ACA territories [11].
On the other hand, our case was a patient with CML and it may be thought that cerebral ischemia occurred due to leukocytosis.
Since, in leukemias such as CML, there is hyperleukocytosis and such high leukocyte counts increase blood viscosity [12].
Hyperleukocytosis, defined as a white blood cell (WBC) count greater than 100,000/μL, often is associated with increased morbidity and mortality in patients with leukemic processes. Most authors have reported reaching a peripheral blood count of less than 100,000/μL as the goal of leukapheresis [13].
In our case, we did not consider cerebral ischemia due to leukocytosis because the leukocyte value of the patient was not at a level to show leukapheresis need. However, it should be considered that the patient's CML in the blast phase may cause cerebral ischemia in the patient.
In our case report we show rare and unreported cerebellar ischaemia by the pituiter apoplexy. We would like to highlight that the presence of infarction in the cerebellum, rather than infarct of anterior circulation, can occur due to the effect of vasogenic agents.
Cerebral ischemia is a rare but life-threatening condition in patients with pituitary apoplexy and it may occur with different mechanisms.
Although, clinicians focus on visual disturbance and endocrine problems in pituitary apoplexy, should be kept in mind that clinicians and surgeons may have cerebral infarction in different regions with the effect of vasospasm and we should be aware of this aspect.