As per Guidelines for surgical management of Traumatic Brain Injury by Brain Trauma Foundation & The Congress of Neurological surgeons, surgery is indicated in Acute subdural haematoma if CT scan shows midline shift > 5 mm, or haematoma thickness > 10 mm regardless of patient's Glasgow coma scale score. However, nothing specified separately for sub-acute subdural haematoma. Mostly same criteria are being followed for selecting patients for surgery in sub-acute and chronic subdural haematoma. Such patient of sub-acute subdural haematoma, whose CT scan head shows midline shift > 5 mm, or haematoma thickness > 10 mm, presented here kept on clinico-radiological assessment showed complete resolution. Clinico-radiological assessment is a good treatment option, ethically always should be offered to such patients avoiding unnecessary surgical interventions and its complications. Also reduces workload on Neurosurgical operation theatres and expenditure on health care. However large study needs for support.
Sub-acute subdural haematoma (SASDH) is an entity not separately addressed properly. The hypo-perfused tissue in the acute phase might become hyper-perfused during the sub-acute phase owing to impaired auto-regulation, and the hyper-perfusion may be responsible for the development of the SASDH [1]. There are two main mechanisms for the spontaneous resolution of acute subdural haematomas: Dilution in subarachnoid space and redistribution of the haematoma in the subdural space [2]. Till today there is no clinical or radiological criteria over which one can predict about progression or resolution of SASDH. Sub-acute subdural haematoma is a poorly individualised neurological entity, often equated clinically to chronic subdural haematomas [3] but its sudden deterioration clinically put it with acute sub-dural haematoma. Although SASDH is being treated by burr hole surgery but there are no clear-cut guidelines as when surgery is to be performed [4]. As per Guidelines for surgical management of Traumatic Brain Injury by Brain Trauma Foundation & the Congress of Neurological surgeons, surgery is indicated in Acute subdural haematoma if CT scan shows midline shift > 5 mm, or haematoma thickness > 10 mm regardless of patient's Glasgow coma scale score [5]. Guidelines did not specifically mention about indication of surgery in SASDH separately.
A 55-year-old male, a known hypertensive presented with continuous headache for last two weeks. Headache was mild, diffuse, no diurnal variation, not associated with vomiting, seizures. He took analgesics but headache persisted. Neurologically patient was normal. CTScan head dated 4th Aug'2016 (Figure 1) showed left frontoparietal sub-acute subdural haematoma (11 × 8 × 1.6 cm) with 8 mm midline shift to right side. Repeat CT scan dated 6th Oct'2016 (Figure 2) showed chronic subdural haematoma at the same site where sub-acute subdural haematoma was present. Further, CTScan dated 15th Dec' 2016 showed complete resolution of subacute subdural haematoma (Figure 3). Altogether, neurologically patient was normal throughout.
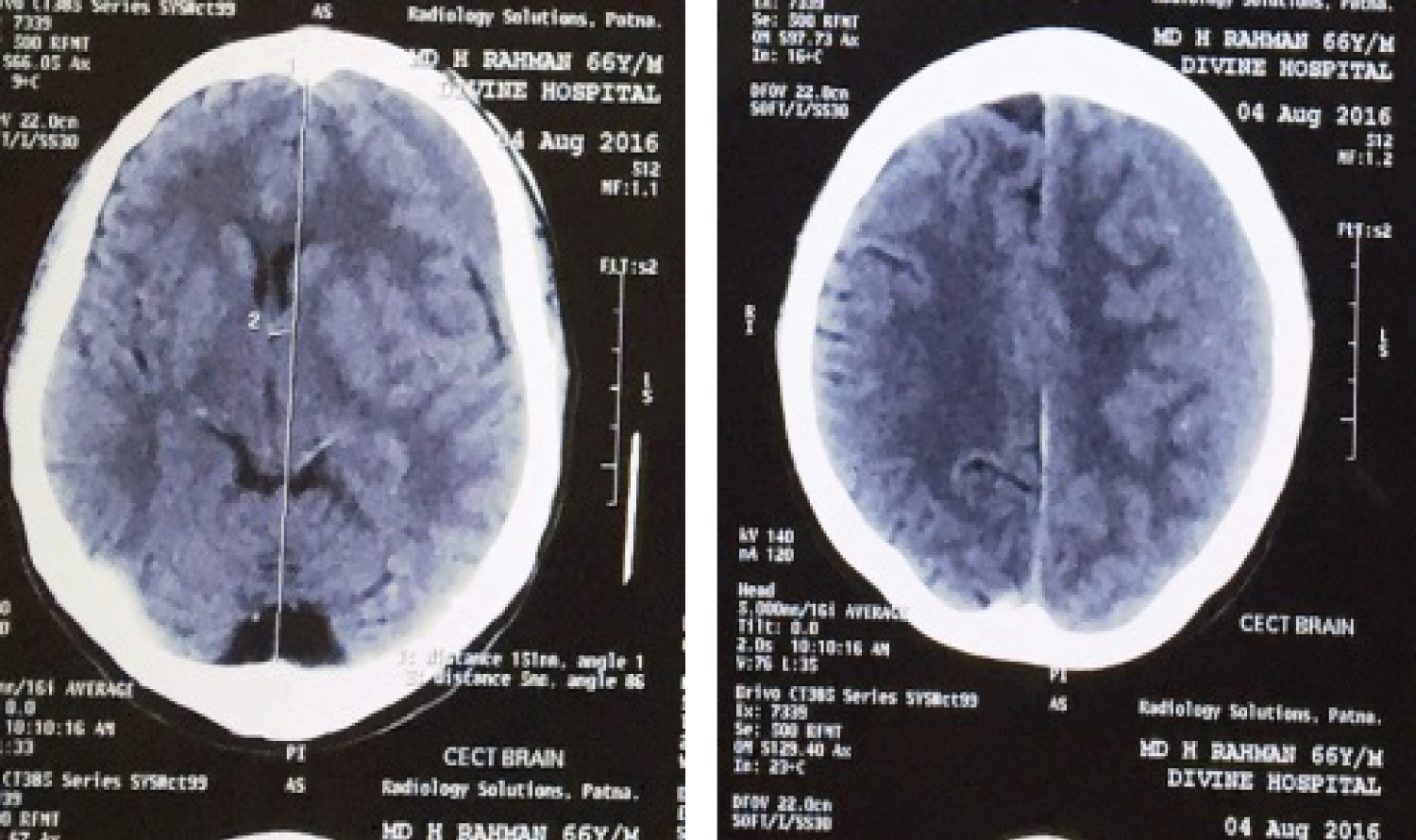 Figure 1: CT Scan dated 4th Aug'2016 showing left fronto parietal sub-acute subdural haematoma (11 × 8 × 1.6 cm) with 8 mm midline shift to right side. View Figure 1
Figure 1: CT Scan dated 4th Aug'2016 showing left fronto parietal sub-acute subdural haematoma (11 × 8 × 1.6 cm) with 8 mm midline shift to right side. View Figure 1
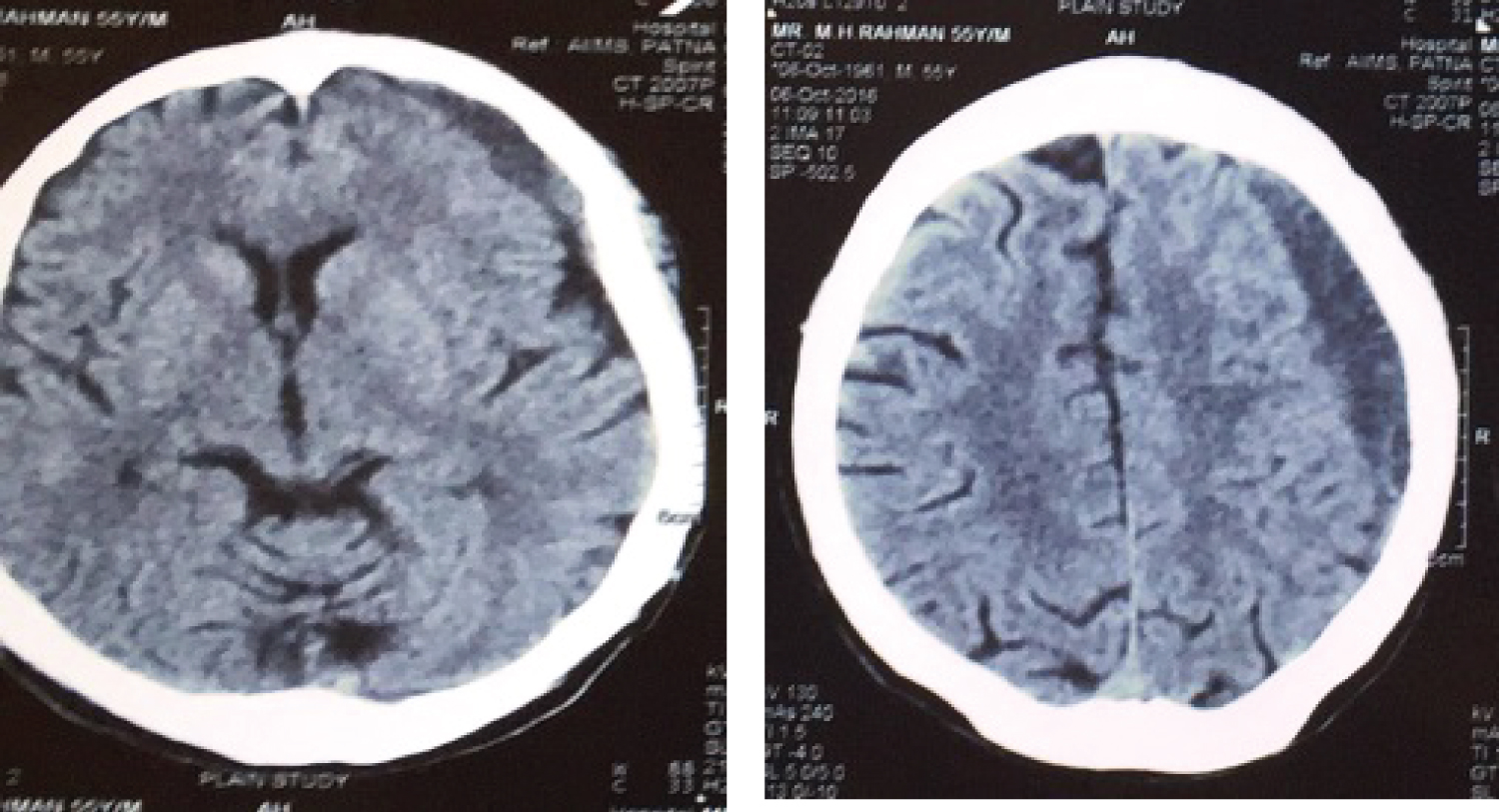 Figure 2: Repeat CT Scan dated 6th Oct'2016 showing chronic subdural haematoma at the same site where subacute subdural haematoma was present.
View Figure 2
Figure 2: Repeat CT Scan dated 6th Oct'2016 showing chronic subdural haematoma at the same site where subacute subdural haematoma was present.
View Figure 2
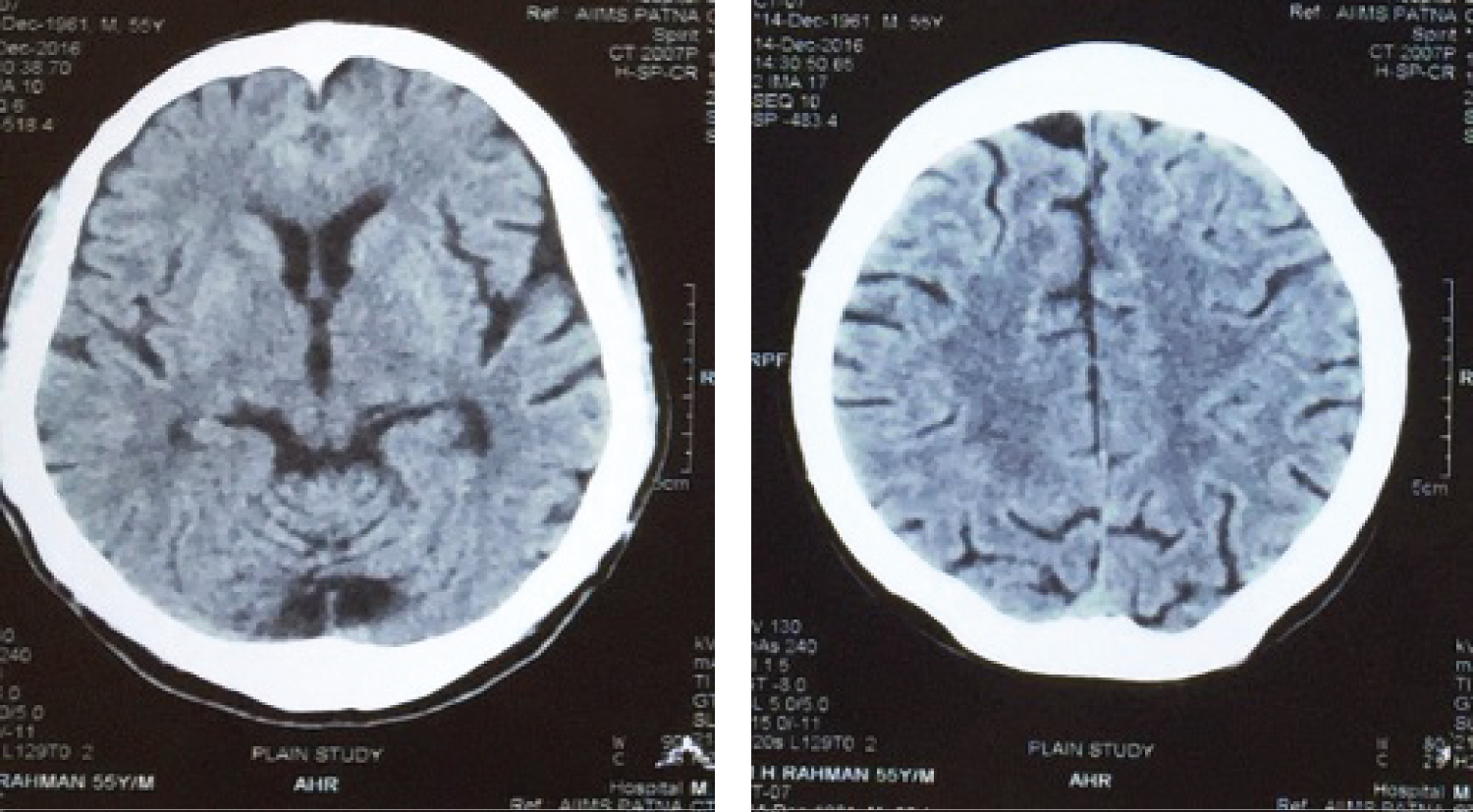 Figure 3: CT Scan dated 15th Dec'2016 showing complete resolution of sub-acute subdural haematoma at left front parietal region.
View Figure 3
Figure 3: CT Scan dated 15th Dec'2016 showing complete resolution of sub-acute subdural haematoma at left front parietal region.
View Figure 3
Patient had significant sub-acute subdural haematoma radiologically with thickness of 16 mm and midline shift of 8 mm and persistent headache, no vomiting, without any neurological deficit. As per Guidelines for surgical management of Traumatic Brain Injury by Brain Trauma Foundation & the Congress of Neurological surgeons, Surgery is indicated in such patient. But considering his clinical condition, patient was followed with repeat CTScan's and neurological assessment at regular follow up. Patient recovered completely with due course of time, and there was complete resolution of sub-acute subdural haematoma over a period of four month and eleven days.
Patients with significant SASDH (with midline shift > 5 mm or maximum haematoma thickness > 10 mm) without any Neurological deficit and radiologically indicating surgical treatment as proposed in guidelines for the Surgical Management of Traumatic Brain Injury by Brain Trauma Foundation and the Congress of Neurological Surgeons released in 2006. Such cases should be followed with repeat CT Scans and neurological assessment to avoid unnecessary surgical intervention in patients who may recover completely with due Course of time. There are no criteria indicating that which SASDH will resolve. Outcome of this case report is to draw attention of Neurotrauma Surgeons to give chance for spontaneous regression of SASDH before surgical intervention. It will save patients from unnecessary surgery and its complications. Which will definitely reduce workload on Neurosurgical operation theatres & expenditure on health care. However, large study needs to support.
None.