Spontaneous cerebrospinal fluid (CSF) leaks are defined as leaks without identifiable etiology, often presenting as spontaneous rhinorrhea. This is thought to be a variant of idiopathic intracranial hypertension (IIH). Spontaneous CSF leak closure often requires surgery, which has proven to be less successful than their non-spontaneous counterparts. There is growing evidence that active intracranial pressure (ICP) management in the postoperative care can improve success rates. We aim to give an update about the current use of acetazolamide in the postoperative care of spontaneous CSF leak closure.
We retrospectively reviewed the charts of three patients at our center who were surgically treated for spontaneous CSF leaks. Postoperatively, two patients experienced headaches resembling those accompanying elevated ICP. However, further examination was within normal ranges. Still, acetazolamide was administered after which their symptoms subsided. Our third patient had an empty sella on preoperative imaging, a finding often associated with IIH, and therefore was given acetazolamide immediately postoperative. She experienced no signs nor symptoms of elevated ICP.
Acetazolamide is widely accepted as first line treatment in IIH and is sometimes used postoperatively after endoscopic closure of spontaneous CSF leaks associated with elevated ICP. Regular administration in the postoperative care of spontaneous CSF leak closures might be considered to increase success rates. Future studies, preferably large multicenter randomized controlled trials (RCTs), are warranted to confirm this clinical observation.
Acetazolamide, Cerebrospinal fluid leak, Endonasal endoscopic closure, Idiopathic intracranial hypertension
Cerebrospinal fluid (CSF) rhinorrhea results from communication between the subarachnoid space and sinonasal cavity. Differentiation is often made between traumatic (either iatrogenic or non-iatrogenic) and non-traumatic (spontaneous, congenital and tumor-based) causes [1]. Congenital and tumor-based leaks are beyond the range of this review, and will therefore not be discussed. Sharma, et al. found traumatic causes to be more common (61%), as opposed to Psaltis, et al. who found an almost identical distribution amongst traumatic (50.2%) vs. non-traumatic (49.8%) causes. The latter reported spontaneous fistulae to be the most commonly reported type, accounting for 41.1% of fistulae [2,3]. Treatment strategies differ according to the underlying etiology and leak location but surgical repair is often needed. An endoscopic endonasal approach is now considered the golden standard with overall success rates averaging around 90%, increasing to 96.6% when including second attempts at repair [3].
Traumatic CSF leaks often settle with conservative treatment, but the risk of ascending meningitis must be taken into consideration. A recent systematic review found iatrogenic injuries unlikely to heal spontaneously, requiring initial surgical repair. Non-iatrogenic traumatic CSF leaks however are likely to resolve spontaneously, making non-surgical management within the first days acceptable [4,5].
Spontaneous CSF rhinorrhea has no identifiable etiology and typically presents unilaterally in obese, middle-aged women [3,6]. Clinical confirmation is made by laboratory analysis of the nasal fluid for β2-transferrin or beta trace protein. Localization of the skull base defect is warranted prior to intervention, with computed tomography (CT) or magnetic resonance imaging (MRI) used as primary imaging modalities [7]. As opposed to traumatic CSF leaks, they usually necessitate surgical closure. However, the endoscopic surgical repair of spontaneous CSF leaks is often less successful than for most other causes, with a historically described recurrence rate of 25-87% vs. < 10% [8-10].
It is increasingly recognized that spontaneous CSF leaks may be associated with an elevated CSF pressure, more specifically idiopathic intracranial hypertension (IIH) [8,9,11,12]. IIH is a subtype of intracranial hypertension in the absence of other causes. It is defined by the modified Dandy criteria [13]. All criteria as seen in Table 1 must be met (Table 1). Although not exclusive for IIH, neuroimaging evidence includes complete or partial empty sella, flattening of the posterior globes, stenosis of the transverse sinus, optic nerve distension and encephaloceles [14]. Treatment options are either conservative (weight loss and pharmaceutical agents such as acetazolamide or topiramate) or surgical (CSF diversion or alternatives like endovascular stenting in case of a proven venous sinus stenosis) [15].
Table 1: The modified Dandy criteria for IIH. All criteria must be met. View Table 1
Idiopathic intracranial hypertension and spontaneous CSF leaks share similar patient demographics. They are predominantly overweight, middle-aged women and up to 72% of patients with spontaneous CSF leaks also fit the Dandy criteria for IIH [12,16-18]. Furthermore, multiple studies have demonstrated direct measurements of elevated CSF pressure in spontaneous CSF leaks, especially after surgical closure [8,11,12,17,19,20]. Following surgical repair of spontaneous CSF leaks, ICP may increase as much as 8.0 cmH2O on average [19,21]. Supposedly, up to 50-85% of spontaneous leak patients have radiographic evidence of elevated ICP [9,21]. As first postulated by Schlosser, et al., spontaneous CSF leaks may act as a release valve for increased ICP, normalizing CSF pressure until after repair of the leak site [22].
Active ICP management by postoperative acetazolamide or CSF shunting significantly increases the chances of success in primary closure to over 90% but is not yet routinely implemented [11,16,23]. It also decreases the chances of recurrence at the same or at a distant site [24]. We aim to examine the existing evidence about the use of acetazolamide in the postoperative setting after endoscopic closure of spontaneous CSF leaks.
To illustrate our subject, we describe three patients surgically treated for spontaneous CSF leaks in the University Hospitals of Leuven, Belgium. Before retrospectively reviewing their charts, a favorable ethical advice (reference no. MP010552) to use human data was obtained from the Research Ethics Committee UZ/KU Leuven. Our endpoint was their clinical outcome. Data extracted included age and gender, relevant medical history, signs and symptoms at presentation, etiology, course of their current condition, treatment method and subsequent follow-up.
Patient 1 is a 31-year old woman with a BMI of 39.03 kg/m2 and no relevant medical history. In August 2018 she presented with right unilateral rhinorrhea which started 2 months earlier during her holiday without preceding head trauma. The nasal fluid was tested for β2-transferrin which proved its origin to be CSF. Medical imaging (Figure 1) showed a bony defect in the right cribriform plate.
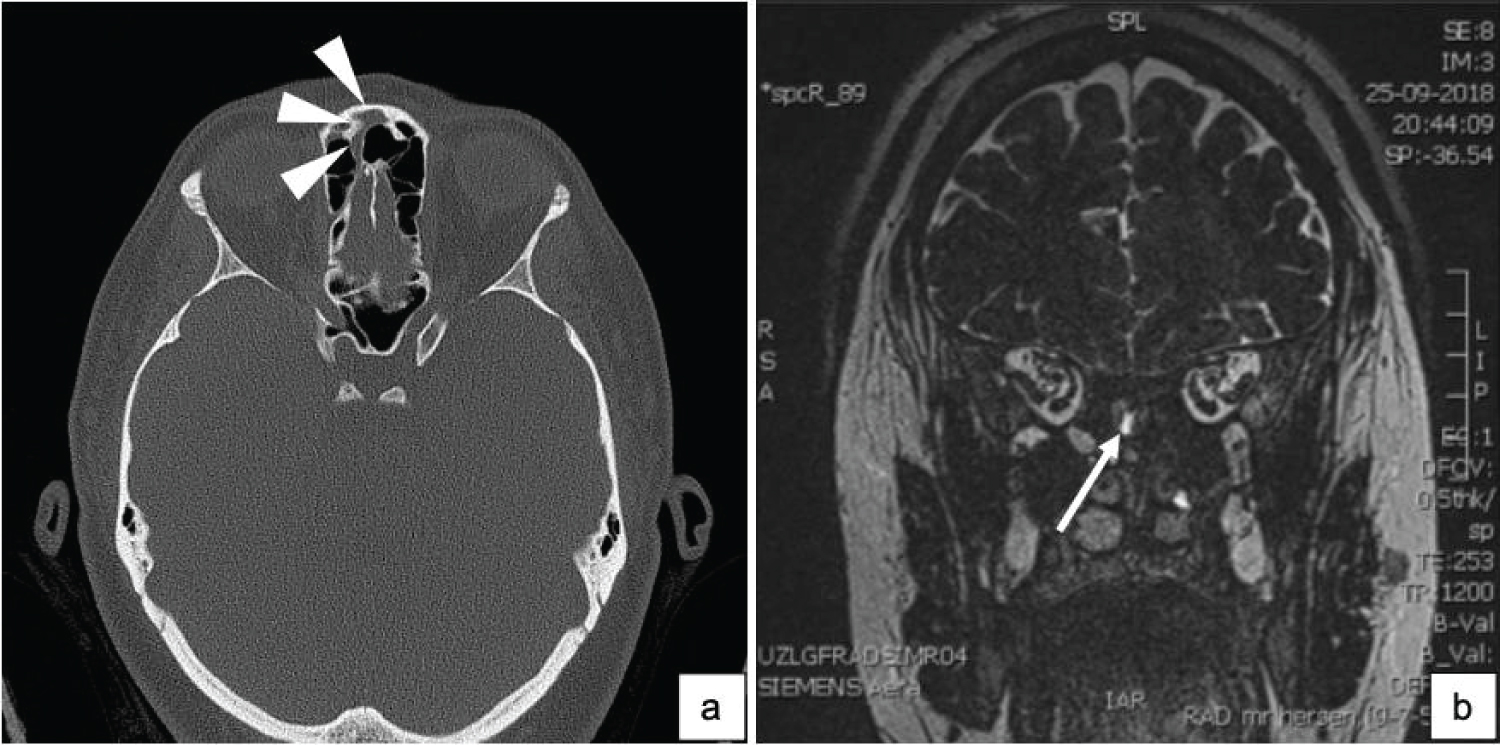 Figure 1: (a) A transverse plane of the preoperative CT scan in our first patient showing a continuity through the right cribriform plate (white arrowheads); (b) A coronal plane of the preoperative MRI showing the same continuity through the right cribriform plate (white arrow). View Figure 1
Figure 1: (a) A transverse plane of the preoperative CT scan in our first patient showing a continuity through the right cribriform plate (white arrowheads); (b) A coronal plane of the preoperative MRI showing the same continuity through the right cribriform plate (white arrow). View Figure 1
Surgical repair of the cribriform plate after intrathecal injection of fluorescein was planned a few weeks later. The leak was visualized during surgery (Figure 2) and closed with a multilayer reconstruction consisting of inlay and underlay fascia lata and overlay medial concha mucosa.
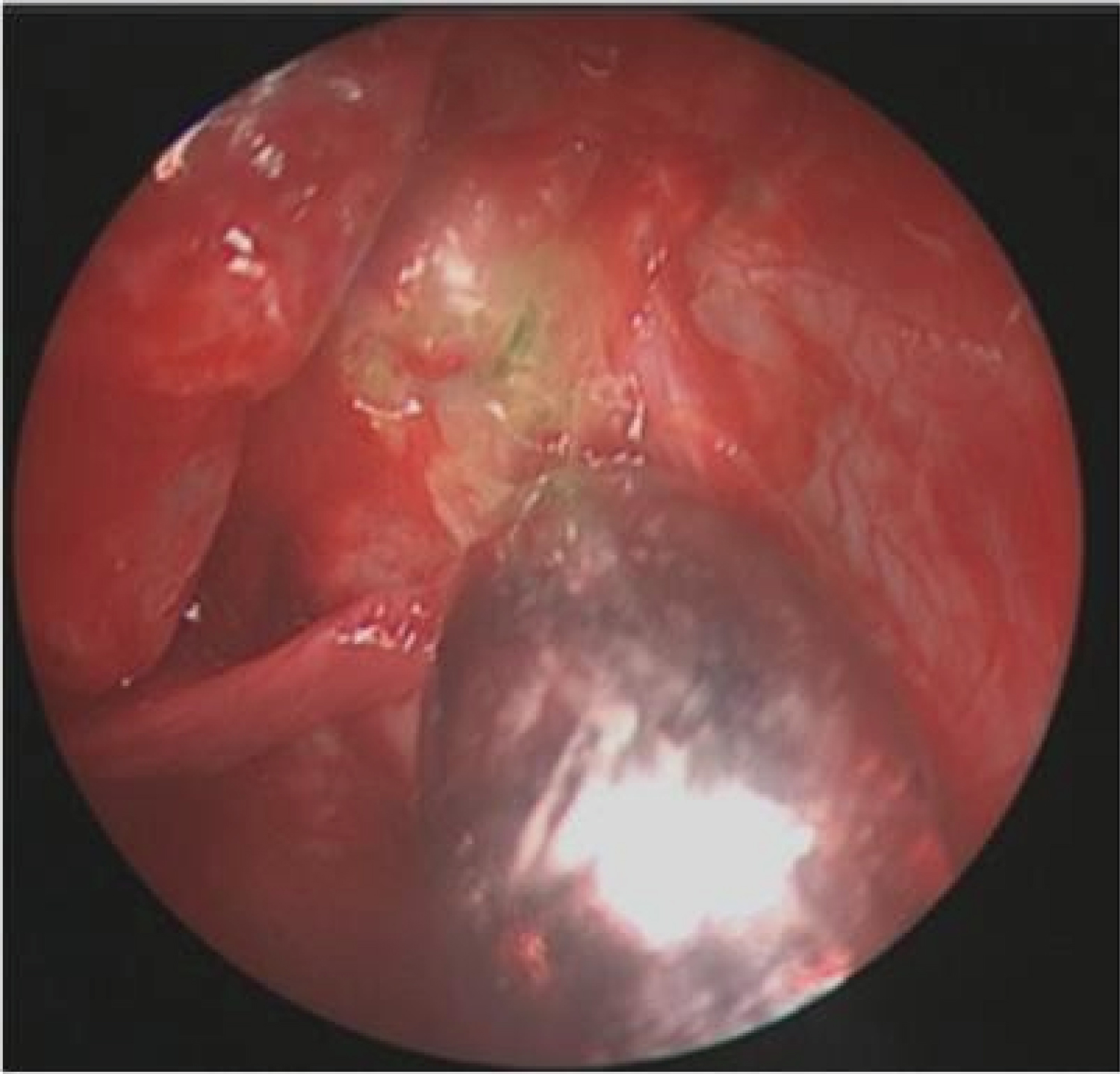 Figure 2: Intraoperative visualization of fluorescein leakage (green) in our first patient.
View Figure 2
Figure 2: Intraoperative visualization of fluorescein leakage (green) in our first patient.
View Figure 2
Postoperatively, conservative therapy was started: stool softeners, avoidance of Valsalva maneuvers and strict bed rest with 30° elevation of the head of the bed. Two days post-surgery, she developed a progressive holocranial headache with vomiting, right aural fulness and photophobia. She was afebrile and showed no other signs suggestive of meningitis. Her symptoms improved after administration of 250 mg of acetazolamide. Ophthalmological examination showed no papilledema and repeat brain MRI scan showed no radiological signs of IIH. A lumbar punction 6 weeks post-surgery showed an opening pressure of 19 cmH2O (normal range 5-20 cmH2O in lateral decubitus position). Acetazolamide was stopped 48h beforehand and was afterwards not restarted. The patient continues to do well, with no recurrence of complaints to date.
Patient 2 is a 47-year-old man with a BMI of 25.18 kg/m2 who presented in September 2017 with chronic bilateral rhinorrhea and intermittent headaches as of the summer of 2015. In his medical history we found an endoscopic sinus surgery (ESS) procedure and septoplasty in 2014, carried out in the context of chronic rhinosinusitis. During the ESS procedure the cribriform plate remained untouched. Furthermore, our patient was treated elsewhere for meningitis 2 months prior to presentation at our center. A β2-transferrin test proved the fluid origin to be CSF. Radiological examination showed a defect in the right cribriform plate. A cisternography executed pre-surgery is shown in Figure 3a. Perioperatively injected fluorescein leakage through the right cribriform plate was objectified. The leakage site was closed with inlay and underlay fascia lata and a free mucosal flap of the medial concha in overlay. On day 3 postoperatively, the patient developed a headache with nausea and vomiting. He remained afebrile and laboratory analysis was normal. A brain CT scan was normal. Administration of acetazolamide 250 mg improved his symptoms and was continued for one week. There is no recurrence of headaches or CSF leakage to date. A cisternography executed post-surgery is shown in Figure 3b.
 Figure 3: (a) A preoperative cisternography clearly showing intracranial tissue protruding through the roof of the right cribriform plate; (b) A postoperative cisternography which no longer shows protruding intracranial tissue.
View Figure 3
Figure 3: (a) A preoperative cisternography clearly showing intracranial tissue protruding through the roof of the right cribriform plate; (b) A postoperative cisternography which no longer shows protruding intracranial tissue.
View Figure 3
Patient 3 is a 43-year-old woman with a BMI of 34.83 kg/m2 without medical antecedents relevant for her current condition. She presented in September 2018 with right unilateral rhinorrhea, which spontaneously started 2 months earlier. She also intermittently experienced headaches. The nasal fluid was again confirmed to be CSF through β2-transferrin evaluation. Medical imaging showed attenuation of the lateral wall of the right frontal ethmoid on CT as well as an empty sella on MRI (Figure 4).
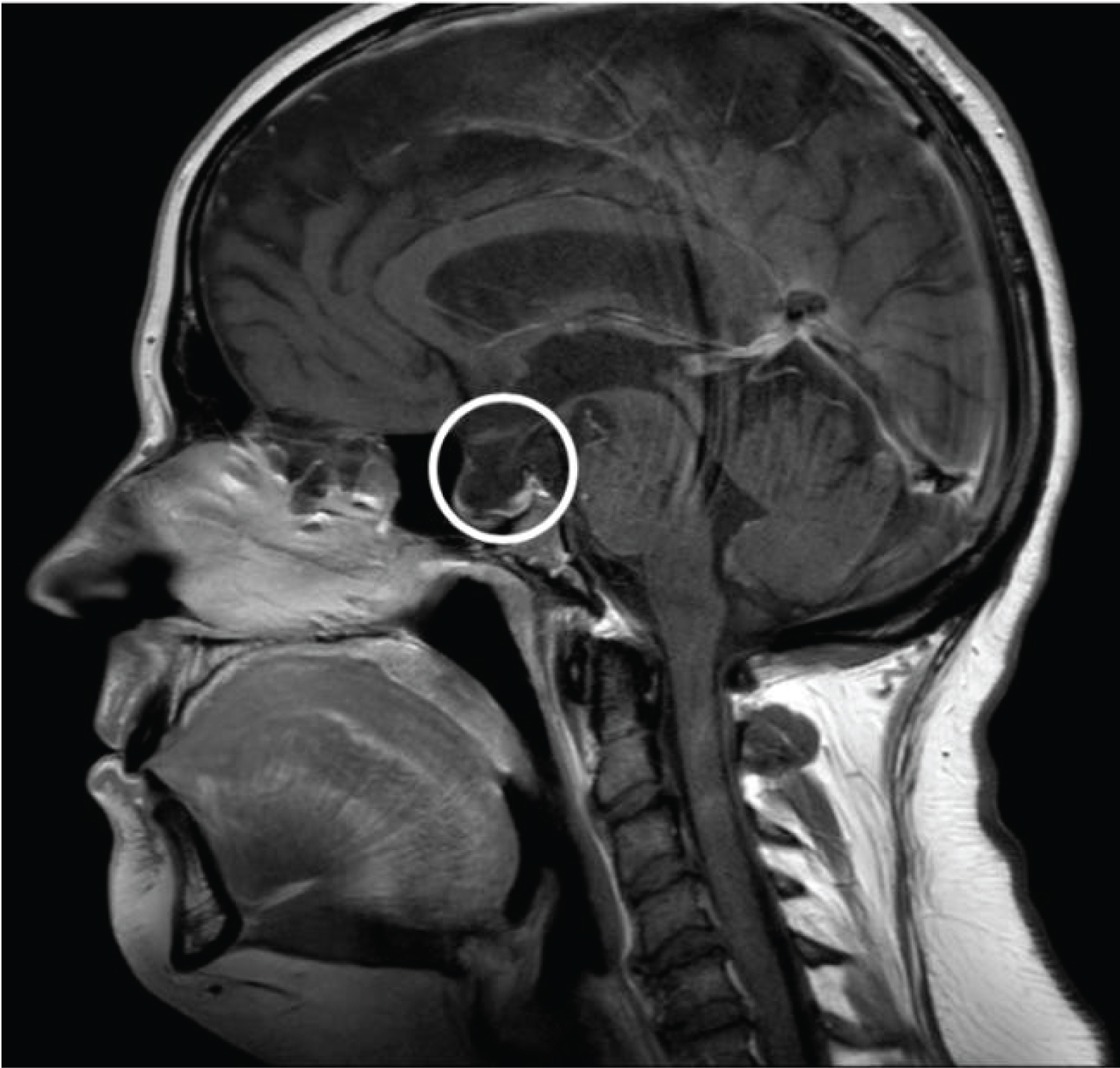 Figure 4: A sagittal view on the empty sella in our third patient (circle).
View Figure 4
Figure 4: A sagittal view on the empty sella in our third patient (circle).
View Figure 4
Endoscopic CSF leak closure after intrathecal injection of fluorescein was performed in October 2018, using a multilayer reconstruction with inlay and underlay fascia lata and conchal mucosa in overlay. Acetazolamide 250 mg once daily was started immediately postoperative because of the preoperative finding of an empty sella and other factors known to be related to IIH (female gender, overweight). She did not develop any postoperative complaints, and acetazolamide was discontinued after 7 days. Three weeks later, both an ophthalmological and neurological examination showed no abnormalities.
The current literature suggests an association between IIH and spontaneous CSF leaks, and even proposes spontaneous CSF leaks to be a direct consequence of long-existing elevated CSF pressure in IIH [25,26]. Strong pulsations of CSF in case of elevated ICP might attribute to an erosive effect on the thinnest and most vulnerable bony structures of the skull base, f.e. the sella turcica and cribriform plate. Intracranial tissue then herniates, resulting in CSF leakage or meningo (encephalo) cele formation [27]. However, this does not provide an explanation why not all patients with IIH develop spontaneous CSF leakage. Individuals with a thicker skull base might develop signs and symptoms of elevated ICP such as papilledema. Others with a thinner skull base might be more prone to erosive effects, presenting with spontaneous CSF leaks [11,28]. Spontaneous leaks in turn may allow for sufficient diversion of ICP and avoidance of complications [29]. When actively leaking, it is likely that our body institutes a new equilibrium between production and absorption of CSF. When the release valve mechanism is surgically closed, that equilibrium is again disrupted resulting in symptomatic elevated CSF pressure.
While the historical recurrence rate of spontaneous CSF leaks is high (up to 25-87%), recent manuscripts suggest that active management of ICP might improve these results to success rates comparable to those of their non-spontaneous counterparts. A recent systematic review separated the results of the reviewed studies by (1) No ICP intervention vs. (2) Active ICP intervention (i.e. acetazolamide administration or permanent CSF diversion in case of elevated postoperative CSF pressure). They found active ICP management to be associated with a significantly higher primary surgery success rate when compared to the cohort of patients without active ICP management (92.82% vs. 81.87% respectively, p < 0.001) [16]. They therefore concluded ICP measurements and active ICP management should become a standard part of the treatment of spontaneous CSF leak patients.
The studied patient population mainly consists of obese women. Weight loss through diet and/or bariatric surgical measures have both been proven to have a positive effect on CSF pressure and therefore on signs and symptoms of IIH [30,31]. Given the association with spontaneous CSF leaks, it seems likely that weight loss might decrease their incidence/recurrence as well.
Pharmacological therapy is most often acetazolamide, a carbonic anhydrase inhibitor which has proven to actively reduce CSF pressure. Chaaban, et al. administered acetazolamide to 36 patients who had confirmed intracranial hypertension (ICH) on lumbar drain after endoscopic CSF leak repair. Mean opening pressure was 32.0 ± 7.4 cmH2O 6 hours after clamping. A single dose of acetazolamide 500 mg significantly decreased the opening pressure to a mean of 21.9 ± 7.5 cmH2O [19]. In another study, 500 mg acetazolamide IV successfully reduced CSF pressure with 9.9 cmH2O on average [8]. Acetazolamide is the first choice of treatment for IIH, although U.S. Food and Drug Administration approval for this purpose is still lacking. Possible adverse effects include anorexia, electrolyte imbalance (necessitating monitoring), acidosis, paresthesias and nephrocalcinosis. Most are mild and benign, making acetazolamide safe and well tolerated up to 4 g/day [32]. A retrospective study reported that acetazolamide was not a significant factor in determining success or recurrence [24]. On the other hand, the International Consensus Statement on Endoscopic Skull-Base Surgery (ICAR; ESBS) recommends considering the use of acetazolamide in patients with spontaneous CSF leaks and elevated ICPs [4]. A consensus about the ideal dosage and time period of administration is lacking. Mentioned alternatives are furosemide, topiramate and mannitol [33].
Permanent CSF diversion is a surgical method for decreasing CSF pressure. The ventriculoperitoneal shunt is the most frequently implemented technique. It is often mentioned as a postoperative measure but has a well-known risk profile (the operative procedure itself, infection, shunt failure, ...). The ICAR; ESBS views these shunts as an option when patients are unable to tolerate medical ICP management, have persisting elevated ICPs or recurrent CSF leaks [4].
Another technique often practiced is the use of lumbar drains (LDs) for perioperative control of ICP. According to a recent systematic review, LDs are used perioperatively in up to 78% of spontaneous CSF leak patients [23]. Albu, et al. randomized 150 patients into management with or without LDs. They found no significant difference in recurrence rates, in accordance with the conclusion of Baksheshian, et al. [34,35]. However, LDs can be used for other reasons: The use of intrathecal fluorescein, reducing stress on the graft and postoperative ICP measurement for guiding therapy. The ICAR; ESBS advocates against routinely perioperative use of LDs. They state that they remain an option for the adjunctive measures mentioned above [4].
Different treatment algorithms with acetazolamide in the postoperative care of endoscopic closure of spontaneous CSF leaks have been proposed. For example, Schlosser, et al. proposed an algorithm frequently implemented by other authors. A lumbar drain is placed 24 hours preoperatively or intraoperatively. Intrathecal fluorescein is injected during surgery. Postoperatively, the lumbar drain is kept at a drainage rate of 5-10 ml/h during 24-48 hours to prevent Valsalva-induced elevations of ICP which might disrupt the reconstruction. On postoperative day 2 or 3, the LD is clamped for a few hours to allow the formation of a new steady state. The CSF pressure is then measured, and acetazolamide 500 mg or furosemide 40 mg is administered when CSF pressure is > 25 cmH2O. After 3-4 hours, CSF pressure is measured again. If the ICP is lowered with more than 10 cmH2O, patients are switched to oral diuretics for a long time period. If the ICP doesn't lower enough or if the initial postoperative ICP is severely elevated (> 35 cmH2O), permanent CSF diversion is advised [8].
Xie, et al. monitored CSF pressure perioperatively in 25 patients. They considered additional treatment not only in case of documented elevated CSF pressure, but also in case of symptoms consistent with elevated ICP. They used high-dose acetazolamide (1-2 g/day) as first-line therapy. Patients remained on acetazolamide until resolution of symptoms or underwent further ICP monitoring to reassess the effect of the diuretics if necessary. Placement of shunt was recommended in patients with persistent elevated ICP based on symptoms, physical findings or repeat monitoring despite acetazolamide treatment [36].
The treatment algorithm proposed by Seth, et al. uses acetazolamide for high risk cases (f.e. patients with a history of IIH) and observes when no increased risk is identified. If acetazolamide treatment results in recurrence or continued high CSF pressure after surgery, a ventriculoperitoneal shunt is installed [18].
None of our patients was postoperatively categorized as IIH according to the modified Dandy criteria. Nevertheless, two of our patients clearly showed symptoms suggestive of elevated ICP. Our third patient had an empty sella on preoperative radiographic evaluation, a typical radiological feature of IIH. It is supposedly also found in up to 77.4-100% of spontaneous CSF leak patients [9,18]. Their high level of clinical suspicion prompted our surgeons to administer acetazolamide. All three did well afterwards, suggesting their signs and symptoms may have been caused by a rebound intracranial hypertension or even in the context of unrecognized IIH. In 2012, Shaw, et al. also presented three cases who did not fit the modified Dandy criteria for IIH. However, given the presence of comorbidities often associated with IIH, they were treated as if they did after which they were relieved of their symptoms. The authors hypothesized that IIH can be a waxing and waning condition, sometimes making clinical suspicion superior to diagnosis through lumbar punctures or radiographic imaging [33]. However, we acknowledge that if there was underlying IIH in our cases this provides no explanation why such a short period of acetazolamide administration suffices in resolving the underlying cause. Another possible explanation is that their signs and symptoms might be categorised as rebound intracranial hypertension.
The evidence strongly promotes active ICP management in the endoscopic closure of CSF leaks. We hypothesize that a routinely administration of acetazolamide postoperatively might even prove to be efficient enough in decreasing ICP in a proportion of patients. This might increase success rates as well as prevent postoperative signs or symptoms as found in our described cases. This without increasing the complication rate, given the fact that less LDs and shunts would be installed and acetazolamide is generally well-tolerated and safe. If patients still develop signs and symptoms of elevated ICP, an objective evaluation would be appropriate to further determine the best treatment strategy. However, we understand that our observation is not sufficient to support this hypothesis. Furthermore, the duration of administration as well as the doses needed for postoperative ICP control remain without consensus and are merely experience-based. A recent retrospective analysis provides some support: 35 patients were surgically treated for spontaneous CSF leaks. All patients received lumbar drainage for 2-3 days postoperatively and were administered acetazolamide 500 mg twice daily for 6-8 months or until resolution of any other preoperatively found clinical symptom. No permanent CSF diversions were needed, with a primary success rate of 100% [17]. Future studies are needed before drawing definitive conclusions, preferably large multicenter randomized controlled trials comparing routinely administration of acetazolamide and one of the treatment algorithms above.
None.
All authors warrant that the article is original, does not fringe upon any copyright or other proprietary right of any third party, is not under consideration by another journal, and has not been previously published. The authors confirm that they have reviewed and approved the final version of the manuscript.
None of the authors has a conflict of interest regarding this paper.