Arachnoid cysts are common findings on neuroimaging and account for approximately 1% of all intracranial lesions. The cerebellopontine angle is the second most common location. When arachnoid cysts become symptomatic due to cyst growth, or rarely, cyst rupture, they create mass effect on adjacent neurovascular structures and may require neurosurgical management. This involves a posterior fossa decompression and cyst fenestration with or without cyst fluid diversion. We present a case of a 40-year-old male who presented with a cerebellopontine angle arachnoid cyst with symptomatic spontaneous intracystic hemorrhage successfully managed conservatively, as well as a review of the literature.
Arachnoid cyst, Cerebellopontine angle, Intracystic hemorrhage, Cerebrospinal fluid
AC: Arachnoid Cyst; CPA: Cerebellopontine Angle; CSF: Cerebrospinal Fluid
Arachnoid cysts (AC) are common findings on neuroimaging and account for approximately 1% of all intracranial lesions. They are developmental collections of cerebrospinal fluid (CSF) enveloped by an arachnoid membrane contiguous with the subarachnoid space. These lesions most commonly occur within the middle cranial fossa, with the cerebellopontine angle (CPA) being the second most common location, accounting for approximately 5.2% of all AC [1,2]. The majority of AC are asymptomatic with a benign natural history; however, they can become symptomatic. This is thought to be due to cyst growth and mass effect on adjacent neurovascular structures, or rarely, after cyst rupture with a combination of intracystic and/or extra-axial intracranial hemorrhage. AC hemorrhage has been reported at rates of 2.3-4.6% however these rates are likely overreported as there is a likely underreported prevalence of all AC as so many are undiagnosed and asymptomatic [3]. Symptomatic AC are commonly treated with surgical resection, with or without shunting. To our knowledge, we present the first report of a CPA AC with spontaneous intracystic hemorrhage in an adult successfully managed conservatively, along with review of the literature.
A 40-year-old male presented with acute onset headache and neck pain which began three days prior to presentation. Due to a progressively worsening headache, along with nausea and vomiting, he presented to our emergency department. The patient had untreated hypertension and was noted to have a presenting blood pressure of 231/133. Physical examination revealed intact neurological function. Computed tomography (CT) of the head was performed and demonstrated a 3.3 × 1.8 cm extra-axial homogeneously hyperdense mass in the left CPA causing regional mass effect on the brainstem and nearby neurovascular structures, with mild dilation of the third and fourth ventricles (Figure 1). MRI of the brain demonstrated a well-circumscribed T1 isointense, T2 hypointense, faint homogeneously gadolinium enhancing, extra-axial mass which appeared to be arising from the left petrous temporal bone with extension into the internal auditory canal. There was a focal area of T1 hyperintensity interpreted as calcification. Imaging characteristics of the lesion were thought to be most consistent with a meningioma with intratumoral hemorrhage. Additionally, T2 hyperintensities in the white matter were present, consistent with a history of uncontrolled hypertension. Conventional diagnostic angiography was negative for tumor blush or underlying vascular malformation.
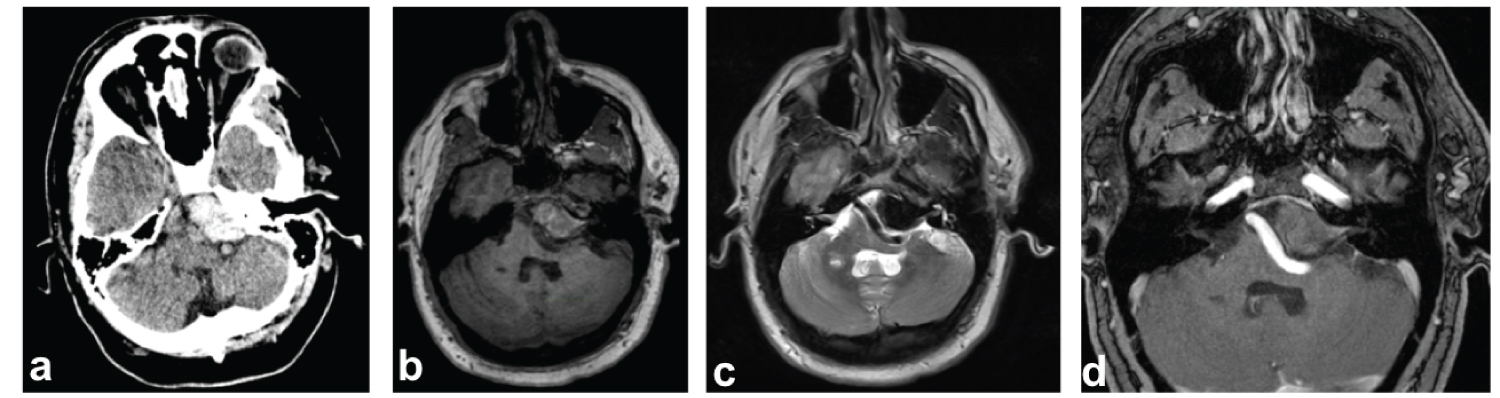 Figure 1: Cerebellopontine angle arachnoid cyst with intracystic hemorrhage. Non-contrast CT. a) Of the head demonstrating a 3.3 × 1.8 cm hyperdense lesion in the left cerebellopontine angle. Axial MRI images with T1 non contrast isointensity; b) T2 hypointensity; c) T1 post gadolinium contrast with minimal enhancement; d) Showing a left cerebellopontine mass which appears to arise from the posterior petrous temporal bone with extension into the left internal auditory canal.
View Figure 1
Figure 1: Cerebellopontine angle arachnoid cyst with intracystic hemorrhage. Non-contrast CT. a) Of the head demonstrating a 3.3 × 1.8 cm hyperdense lesion in the left cerebellopontine angle. Axial MRI images with T1 non contrast isointensity; b) T2 hypointensity; c) T1 post gadolinium contrast with minimal enhancement; d) Showing a left cerebellopontine mass which appears to arise from the posterior petrous temporal bone with extension into the left internal auditory canal.
View Figure 1
The patient continued to experience brittle hypertension despite continuous IV medication which delayed our initial planned surgical intervention of a retrosigmoid craniotomy and resection of the mass. He eventually required four oral anti-hypertensive medications at high doses in order to control his blood pressure. In light of his intact neurological examination, as well as difficulty with medical optimization of his uncontrolled hypertension, the decision was made to pursue resection on an elective basis as an outpatient once he was maintained on a stable medication regimen. He was discharged from the hospital without issue. He underwent a repeat MRI of the brain approximately 8 weeks later. The repeat MRI demonstrated complete resolution of hemorrhage and gadolinium enhancement (Figure 2). All that remained was a T2 hyperintense signal most consistent with a left CPA arachnoid cyst. His headaches had resolved at this time. Six month follow up MRI showed stable size and morphology of the CPA AC indicating successful durability and safety conservative observation alone.
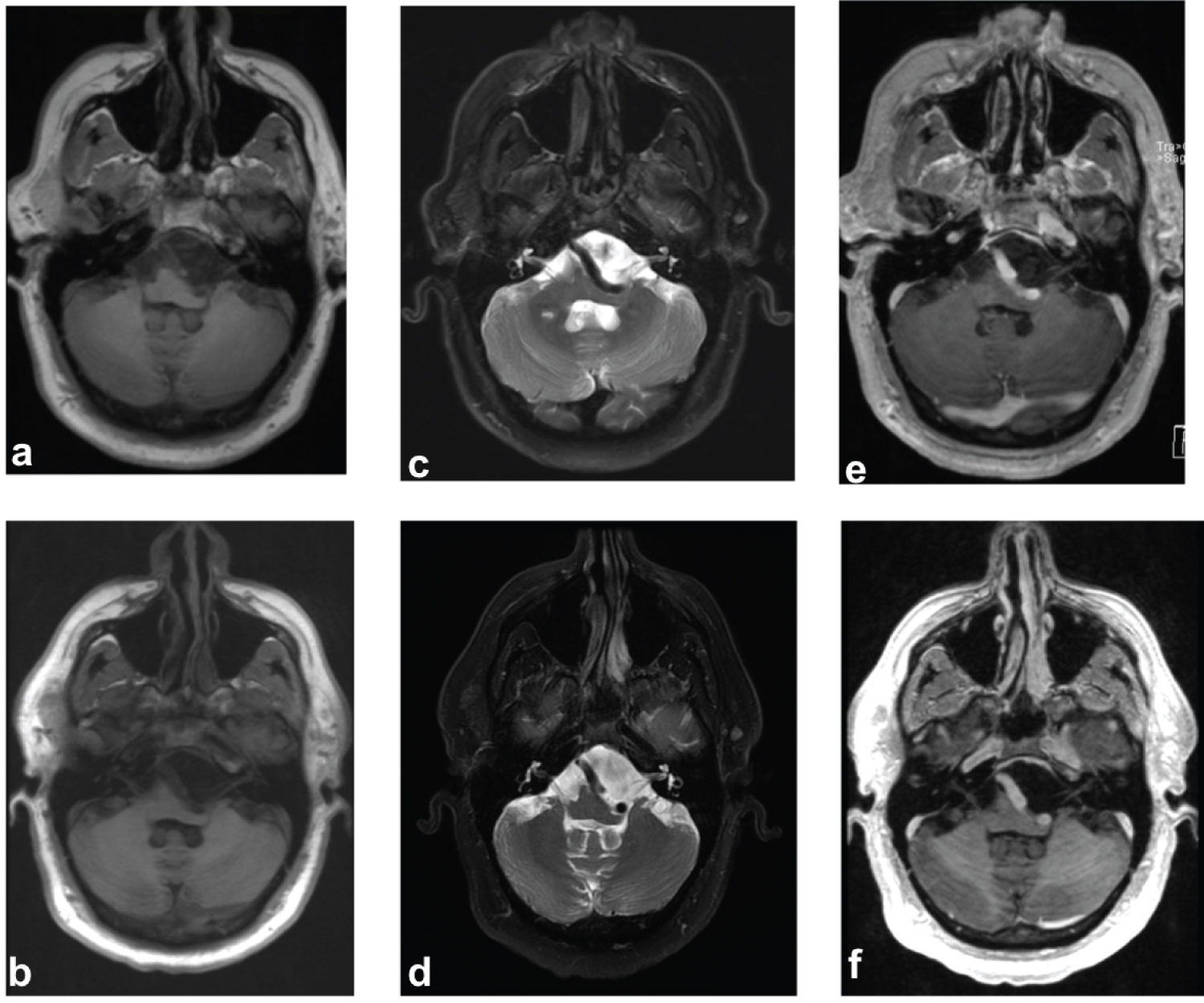 Figure 2: Resolution of intracystic hemorrhage at 8 weeks (top row) and 6 months (bottom row) after presentation. a,b) Axial MRI images with T1 non contrast; c,d) T2 weighted; e,f) T1-post gadolinium; a,c,e) Showing a left CPA mass with complete resolution of intracystic hemorrhage at 8 weeks; b,d,f) 6 months. Note the T1-hypointense/T2-hyperintense signal within the extra axial cyst that is consistent with CSF signal and resolution of hemorrhage within a CPA arachnoid cyst.
View Figure 2
Figure 2: Resolution of intracystic hemorrhage at 8 weeks (top row) and 6 months (bottom row) after presentation. a,b) Axial MRI images with T1 non contrast; c,d) T2 weighted; e,f) T1-post gadolinium; a,c,e) Showing a left CPA mass with complete resolution of intracystic hemorrhage at 8 weeks; b,d,f) 6 months. Note the T1-hypointense/T2-hyperintense signal within the extra axial cyst that is consistent with CSF signal and resolution of hemorrhage within a CPA arachnoid cyst.
View Figure 2
Arachnoid cysts of the cerebellopontine angle are uncommon with a prevalence of 5.2% [1]. Most typically, CPA arachnoid cysts are incidental findings in asymptomatic patients and can be safely monitored with serial imaging. Patients with symptomatic CPA AC can present with a variety of symptoms due to brainstem or cranial nerve compression [2] including sensorineural hearing loss [4,5] diplopia [6], trigeminal neuralgia [7], vertigo [8], hemifacial spasm [9], facial paresis [10], glossopharyngeal neuralgia [11], hoarseness and dysphagia [12]. Jallo, et al. reviewed 33 cases of CPA AC and discussed optimal surgical management. The authors stated that AC which demonstrate progression in regard to size, symptoms of neural compression, hydrocephalus or refractory headaches/emesis require surgical intervention. They recommend suboccipital craniotomy and cyst fenestration [2]. There has not been a discussion in the literature regarding conservative management of spontaneous intracystic hemorrhage in CPA AC.
Intracystic hemorrhage is a rare complication of arachnoid cysts. There are several cases in the literature of patients with supratentorial arachnoid cysts who present with simultaneous subdural hematoma in addition to intracystic hemorrhage. In this scenario, intracystic hemorrhage can be masked on initial radiological examination secondary to the presence of an extra-axial hematoma which occurs secondary to extravasation of blood into the subdural or epidural space [3,13-15]. Only two reported cases of intracavitary hemorrhage in an infratentorial arachnoid cyst have been reported [16,17]. Both cases involved a retroclival arachnoid cyst. In both instances, hemorrhage was thought to be spontaneous as is true in our presented case. The patients both underwent suboccipital craniotomies (Table 1).
Table 1: Published studies of adults with spontaneous intracystic posterior fossa AC hemorrhage. View Table 1
Isolated intracystic hemorrhage, without associated subdural or subarachnoid hemorrhage, is a rare complication. The exact pathophysiologic mechanism behind intracystic rupture is not clearly defined, but several mechanisms have been proposed [13]. Reported cases have occurred both spontaneously as well as in the setting of trauma. Cress, et al. reviewed 14 pediatric cases of patients with intracystic AC hemorrhage with or without concurrent extra-axial collection and noted that larger size of AC (> 5 cm) and recent history of head trauma (including minor head trauma) within prior 30 days were significantly associated with AC rupture [3]. The authors purported that unrecognized trauma can cause flow changes within CSF, which become magnified within an AC. As arachnoid cysts are less compliant than the surrounding subarachnoid CSF spaces, this phenomenon can lead to rupture of vessels within the cyst wall or by bridging veins, resulting in intracystic or subdural hemorrhage, respectively [15].
However, our adult patient presented with spontaneous posterior fossa intracystic hemorrhage in the setting of profound hypertension and denied any history of trauma. In this scenario, other mechanisms of hemorrhage could be more likely. Previous microscopic analyses of AC walls have shown a mesothelial cell layer in close proximity with bridging veins. Differences in osmotic gradient between subarachnoid and intracystic fluid, fluid entrapment due to a slit-valve mechanism, as well as independent fluid production by these mesothelial cells lining cyst walls may explain spontaneous cyst enlargement [18]. If a sufficient intracystic pressure is attained to breach the wall, the surrounding vasculature could be interrupted [19]. Recurrent episodes of this disruption of friable blood vessels within the cyst wall is thought to be a potential source of microhemorrhage within AC. Recurrent microhemorrhages or a large intracystic hemorrhage can cause an increase in size of the AC over time which can eventually cause rupture of the cyst into the subarachnoid and even subdural space [14].
Specifically, in our patient, we propose that his chronic untreated hypertension may have further exacerbated the risk of hemorrhage from these already vulnerable vessels through mechanisms similar to those which have previously been well-described in hypertensive intracerebral hemorrhage. In this model, chronic microvascular changes such as progressive hypertrophy of the tunica media within the wall of the arteriole lead to a progressive hypoxic degeneration and fibrinoid necrosis of the smooth muscle layer. This process leads to collagen deposition and results in a weakening of the arteriolar wall. In some cases, amyloid proteins can deposit in the vessel wall, whereas others develop Charcot-Bouchard aneurysmal dilatations in these vessel walls. These are the likely points of rupture in the setting of elevated systolic blood pressures [20].
Cerebellopontine angle arachnoid cysts are rare intracranial lesions. Pure intracystic hemorrhage within these lesions is even more rare. Patients who present with symptomatic lesions with associated subdural hematoma or with neurological deterioration should be considered for emergent decompression and cyst fenestration. However, in the setting of acute intracystic hemorrhage in an individual who is neurologically intact we propose conservative management. Medical management of risk factors for hypertensive hemorrhages should be targeted in individuals with nontraumatic spontaneous intracystic hemorrhage. We caution that the presence of a well-circumscribed, spontaneous extra-axial, posterior fossa hemorrhage should raise suspicion for an underlying AC.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with human participants or animals performed by any of the authors.
For this type of study formal consent is not required. No identifiable information was included in this manuscript.
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers' bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
No funding was received for this research.
All authors contributed substantially to the conception or design of the work. JP and AK and ROA responsible for critical revision for important intellectual content and the final approval to be published. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.