Surgical intervention in posterior fossa extradural haematoma (PFEDH) carries very good results. But there are no defined indications for surgical evacuation when patient is asymptomatic and normal neurologically, even in the guidelines for surgical management of traumatic brain injury by 'the brain trauma foundation & the congress of neurological surgeons'. Haematoma volume > 10 ml, haematoma thickness > 15 mm, perimesencephalic cisterns obliteration, fourth ventricle displacement and hydrocephalus, are the criteria considered for surgical evacuation by most of neurosurgeons. Patient presented here was clinically asymptomatic with left PFEDH (volume 20 cc and thickness 20 mm) which should have undergone immediate surgical removal, treated conservatively showed complete resolution in six weeks' time. Conservative treatment seems to be a justified approach in asymptomatic PFEDH. However, a larger study is needed to further support these findings.
Posterior fossa extradural haematoma, Glasgow coma scale, CT scan head
Posterior fossa extradural haematoma (PFEDH) often requires urgent surgical removal because of availability of limited space as compared to supratentorial compartment. According to the guidelines for surgical management of traumatic brain injury by 'the brain trauma foundation & the congress of neurological surgeons [1], extra dural haematoma with volume greater than 30 ml should undergo surgical evacuation, regardless of Glasgow coma scale [2]. PFEDH is not described separately in these guidelines. There are no definite guidelines when to operate and when not to operate a PFEDH in neurologically normal patients. According to some authors different criteria for surgical evacuation of PFEDH included are haematoma volume > 10 ml [3], haematoma thickness > 15 mm, perimesencephalic cisterns obliteration, fourth ventricle displacement and hydrocephalus [4]. Patient presented here was left PFEDH (volume 20 cc) and should have undergone immediate surgical removal. However, the patient was treated conservatively and showed complete resolution in six weeks time.
A six-year-old boy sustained trauma due to fall from stairs (about seven feet height) and came to the hospital five days later. After trauma there was transient loss of consciousness for half an hour with repeated vomiting, which regressed completely in two days. On examination, pulse was 90 per minute, Glasgow Coma Scale was 15/15. Neurological examination was normal. CT scan head (Figure 1) showed left posterior fossa extradural haematoma (50 × 20 × 40 mm, volume 20 cc). Patient was treated conservatively, kept under regular clinical and radiological observation. Neurologically, patient remained normal throughout. Left PFEDH haematoma showed marked resolution in CT scan head done after three weeks (Figure 2) and resolved completely in CT scan head done after six weeks (Figure 3).
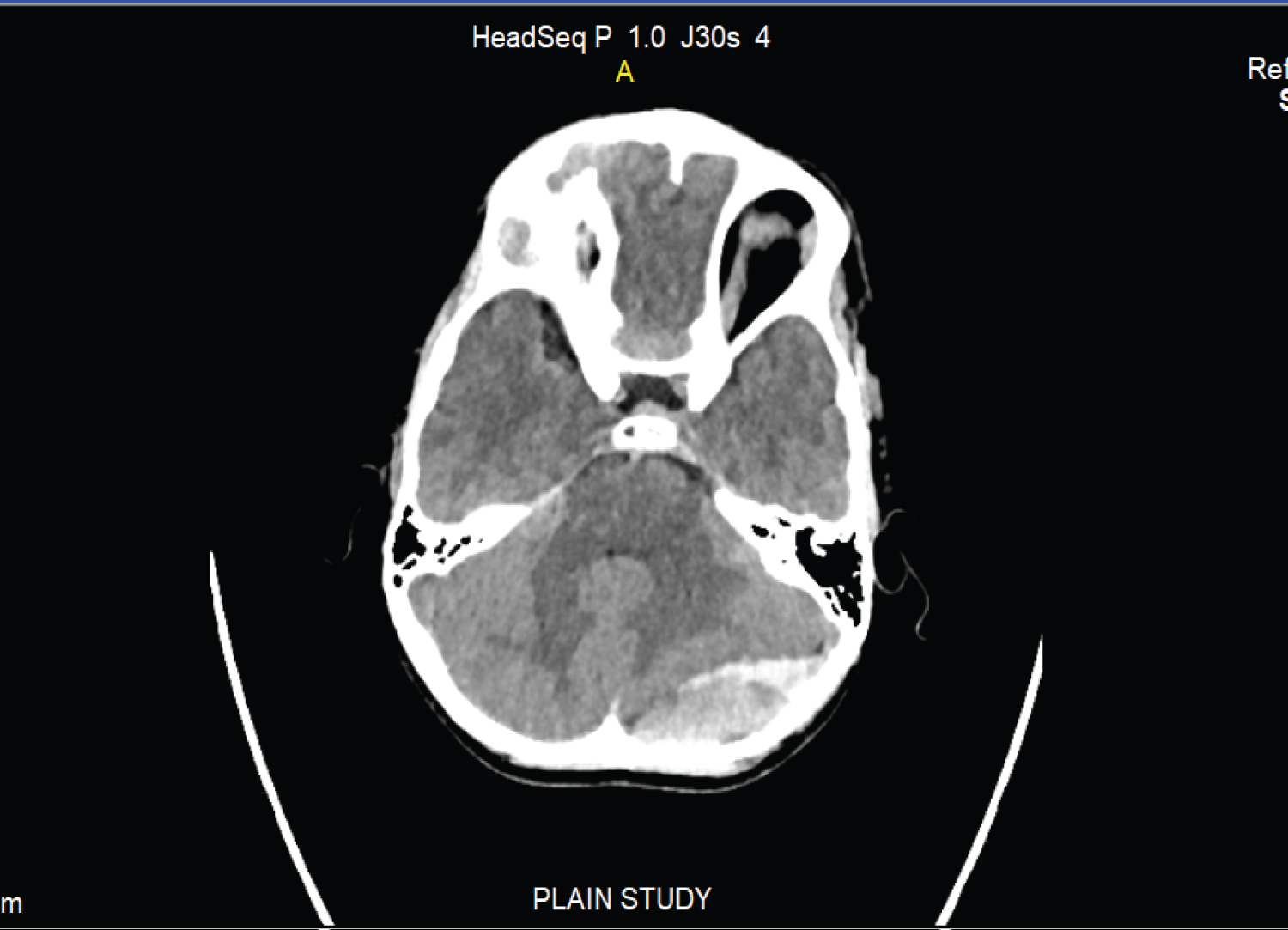 Figure 1: CT scan head (5th post injury day) showed left posterior fossa extradural haematoma (50 × 20 × 40 mm, volume 20 cc). View Figure 1
Figure 1: CT scan head (5th post injury day) showed left posterior fossa extradural haematoma (50 × 20 × 40 mm, volume 20 cc). View Figure 1
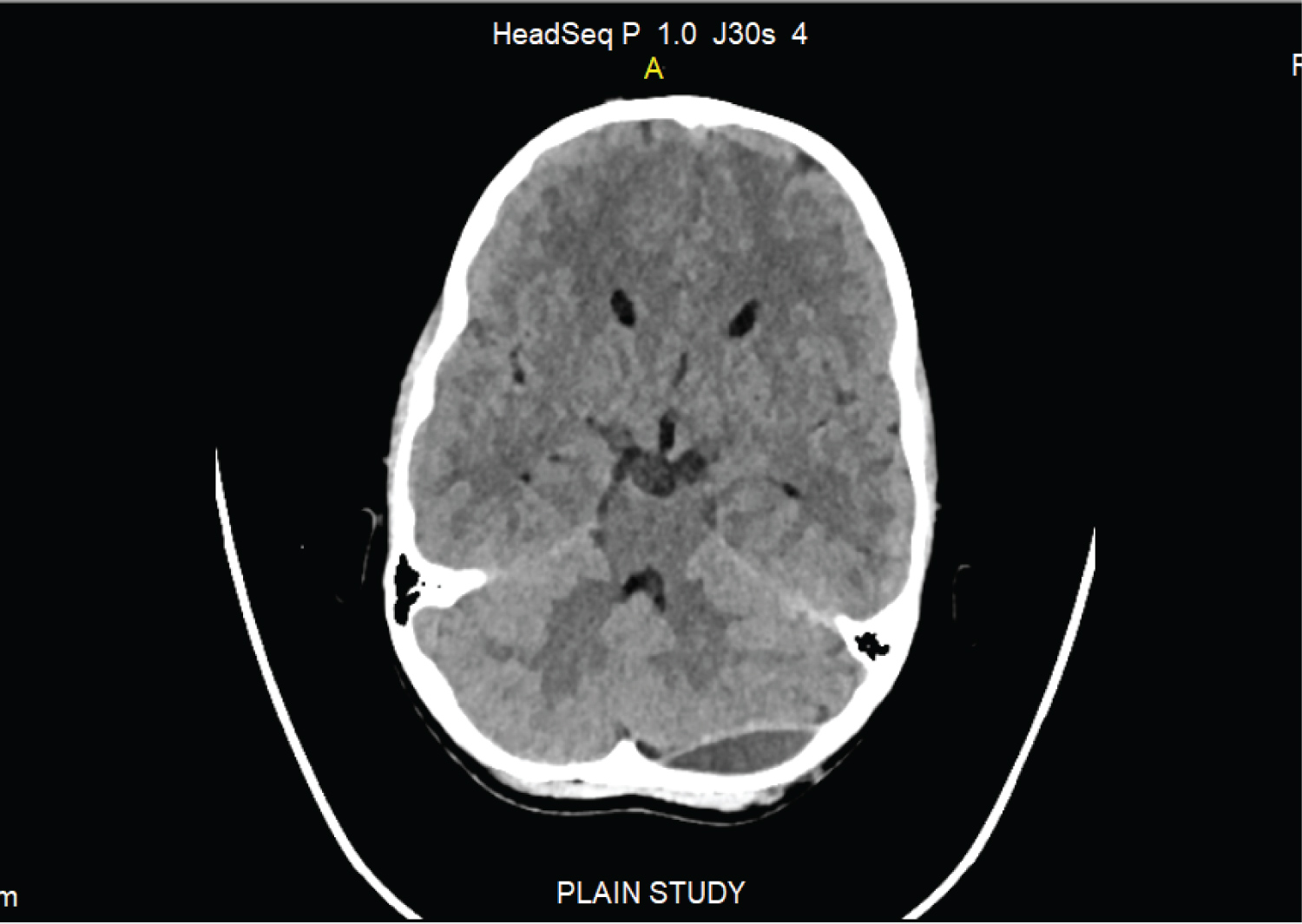 Figure 2: CT scan head (3 weeks after injury), resolving left posterior Foss extra dural haematoma. View Figure 2
Figure 2: CT scan head (3 weeks after injury), resolving left posterior Foss extra dural haematoma. View Figure 2
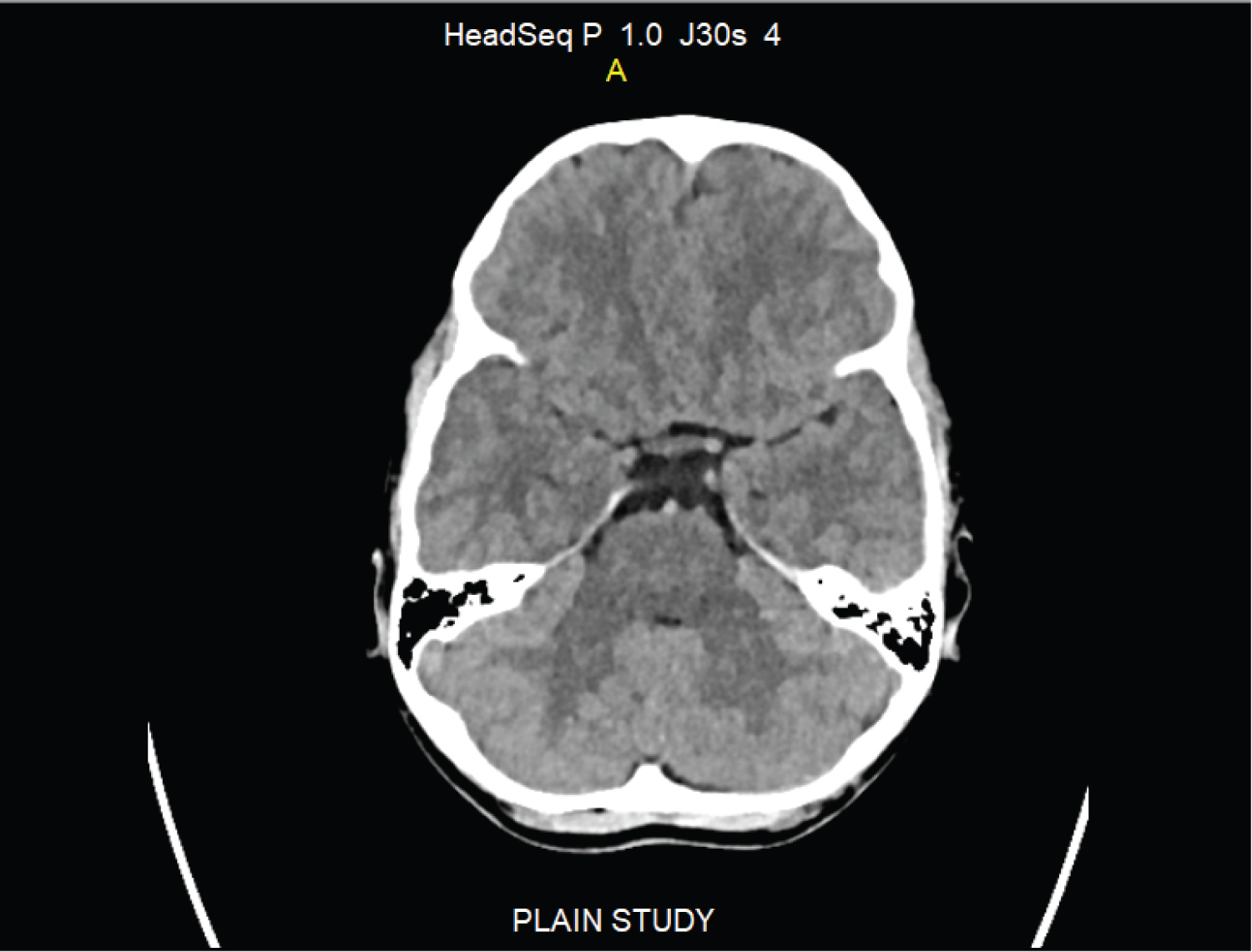 Figure 3: CT scan head (6 weeks after injury) showing complete resolution of left posterior fossa extra dural haematoma.
View Figure 3
Figure 3: CT scan head (6 weeks after injury) showing complete resolution of left posterior fossa extra dural haematoma.
View Figure 3
Traumatic PFEDH is very rare, approximately 0.3% of all craniocerebral injuries [5], and 2.7-11% of all extradural haematomas [6]. All PFEDH which are symptomatic should be operated as early as possible. According to the guidelines for surgical management of traumatic brain injury by 'the brain trauma foundation & the congress of neurological surgeons,' extra dural haematoma with volume greater than 30 ml should undergo surgical evacuation, regardless of GCS. PFEDH is not described separately in these guidelines. There are no definite guidelines when to operate and when not to operate a PFEDH in neurologically normal patients. According to some authors different criteria for surgical evacuation of PFEDH included are haematoma volume > 10 ml, haematoma thickness > 15 mm, perimesencephalic cisterns obliteration, fourth ventricle displacement and hydrocephalus. In this patient PFEDH volume was 20 ml, haematoma thickness was 20 mm, perimesencephalic cisterns and fourth ventricle obliterated, which should have been surgically evacuated immediately, according to most of the authors. Patient's family was reluctant in opting for any surgical intervention, hence, the patient was treated conservatively and was kept under clinical & radiological assessment regularly. PFEDH resolved completely in six weeks' time, saving patient from unnecessary surgical intervention and risks from anaesthesia & surgery. This suggests that in patient of asymptomatic PFEDH with significant volume, conservative treatment is a potential approach as shown by other studies. Resolution of extradural haematoma have also reported by Zakaria, et al. [7,8]. This case report highlights that neuratrauma surgeons should consider conservative treatment as one of the possible treatments in asymptomatic PFEDH with significant volume.
Conservative treatment with regular clinical and radiological observations in asymptomatic PFEDH with significant volume (more than 10 cc) and haematoma thickness more than 15mm, is a possible treatment option. However, a larger study is needed to further support these findings.
None.