Dermoid Cysts are considered congenital lesions, but not all of them are diagnosed at birth. Dermoid cyst involving subgaleal temporal area with no intracranial extension is a rare scalp swelling.
We report a case of 37-year-old female patient presented with a history of a scalp swelling since birth. The swelling increased in size progressively. Magnetic resonance imaging of the brain revealed extracranial cystic lesion over the temporal bone with no intracranial extension. Cyst was excised completely with no postoperative complications. On histopathology it was dermoid cyst.
Early resection mayavoid more extensive surgery, and a shorter skin incision with less risk of wound infection mayallow an improved cosmetic outcome.
Temporal bone, Cyst, Dermoid, Scalp
We report a case of 37-year-old female patient presented with temporal scalp swelling since birth. The swelling increased in size very slowly and progressively. On examination, there was a soft, fluid-filled lesion over the temporal bone, which was non tender and non pulsatile. There was no bruit over the swelling. Magnetic resonance imaging of the brain revealed extracranial well-defined cystic swelling over the left temporal bone with no intracranial extension, measuring approximately 20 × 45 × 30 mm in transverse, anterior-posterior, and craniocaudal dimensions. It was cystic in appearance, with hyperintense signals on T2-weighted sequence, with no flow voids (Figure 1a) and hypointense signals on T1-weighted sequences (Figure 1b) showing no surrounding edema on fluid-attenuated inversion recovery (FLAIR). There was no contrast enhancement (Figure 1c). Intraoperatively, a soft, cystic, fluid filled lesion over temporal bone, which was densely adherent to underlying tissue (Figure 1d). Cyst was excised completely with no postoperative complications. On histopathology it was dermoid cyst.
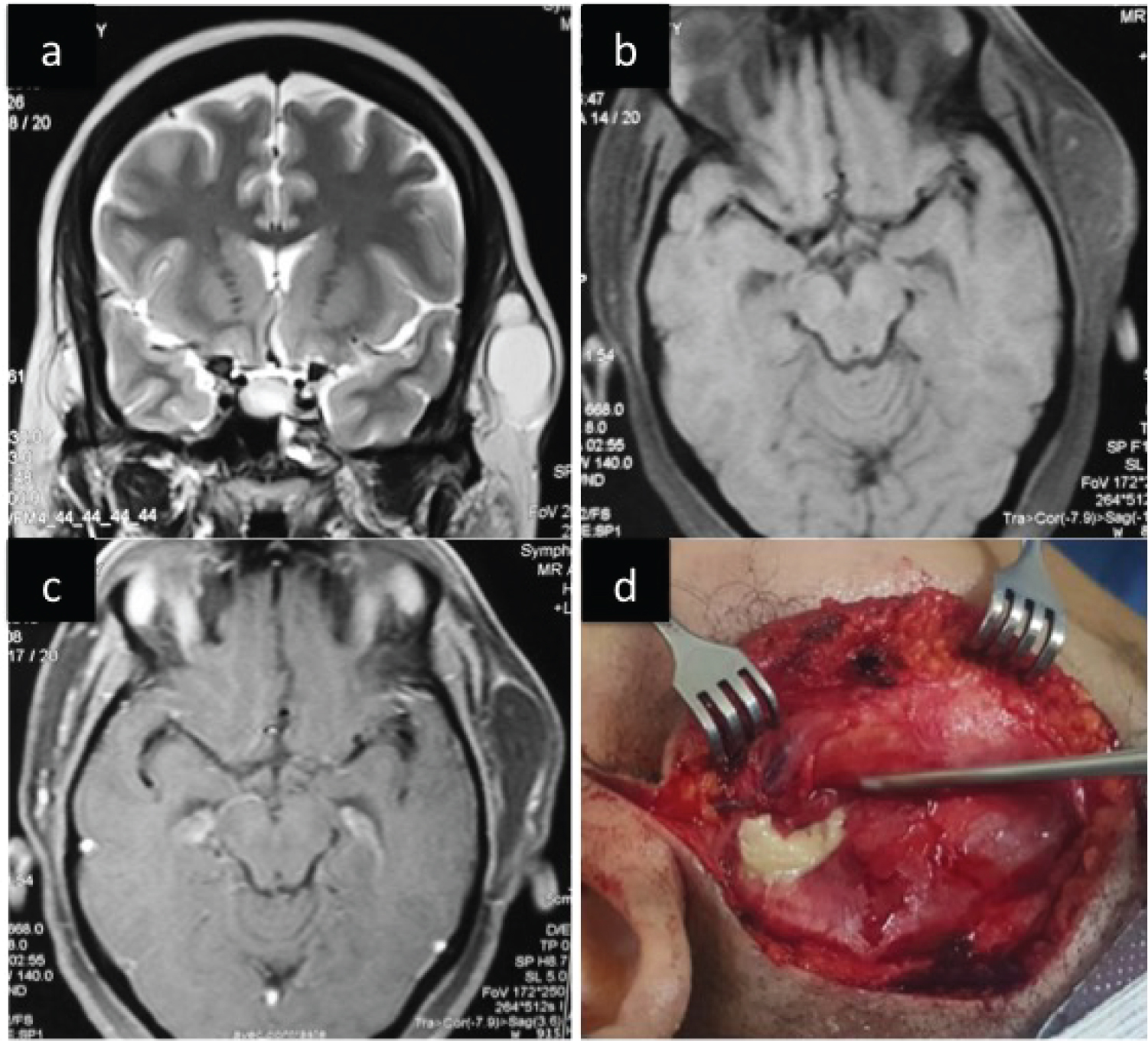 Figure 1: It was cystic in appearance, with hyperintense signals on T2-weighted sequence, with no flow voids (Figure 1a) and hypointense signals on T1-weighted sequences (Figure 1b) showing no surrounding edema on fluid-attenuated inversion recovery (FLAIR). There was no contrast enhancement (Figure 1c). Intraoperatively, a soft, cystic, fluid filled lesion over temporal bone, which was densely adherent to underlying tissue (Figure 1d).
View Figure 1
Figure 1: It was cystic in appearance, with hyperintense signals on T2-weighted sequence, with no flow voids (Figure 1a) and hypointense signals on T1-weighted sequences (Figure 1b) showing no surrounding edema on fluid-attenuated inversion recovery (FLAIR). There was no contrast enhancement (Figure 1c). Intraoperatively, a soft, cystic, fluid filled lesion over temporal bone, which was densely adherent to underlying tissue (Figure 1d).
View Figure 1
Dermoid cysts are considered congenital lesions, but not all of them are diagnosed at birth [1]. Dermoid cysts are benign soft tissue tumors that develop from abnormal sequestration and inclusion of the surface ectoderm along the lines of skin fusion during embryologic development [2]. In the literature, midline scalp cysts present a higher probability of intracranial extension because they are on a line of embryonic fusion. Early resection mayavoid more extensive surgery, and a shorter skin incision with less risk of wound infection mayallow an improved cosmetic outcome [3].
The author has no conflicts of interest to declare.