Squamous cell carcinoma of cutaneous origin is an insidiously developing cancer, and seldom metastasises. Patient and lesion characteristics that predispose to more aggressive biological behaviours include immune incompetence, recurrence following excision and those demonstrating invasion of local lymphovascular and neural structures. An immunosuppressed elderly man with a history of cutaneous squamous cell carcinoma with lymph node involvement, presented to our tertiary centre with personality and cognition changes. Cerebral magnetic resonance imaging demonstrated a left frontal lesion which was eventually revealed to be metastatic squamous cell carcinoma. The clinical context, radiology, histopathology, and immunohistochemistry were highly suggestive of the known cutaneous lesion as the origin. Cutaneous squamous cell metastases to the cerebrum are exceptionally rare and to our knowledge, have only been reported thrice previously. The mechanisms of the pathogenesis of this sequela are not well understood. Our case report highlights relevant epidemiology and features of this disease that are negatively prognostic. Patients with high-risk features and characteristics, especially immunosuppression, should be closely monitored to prevent, detect, and treat, malignant transformation of these lesions. Further case-based characterisations such as this, may assist in elucidating the nature of this pathology. Herein, we present a fourth patient demonstrating this rare phenomenon.
Cerebral metastasis, Immunosuppression, Lymphadenopathy, Skin cancer, Squamous cell carcinoma
Cutaneous squamous cell carcinoma (CSCC) is a common non-melanoma skin cancer (NMSC) and is curable with locally destructive techniques, including topical chemotherapy, cryotherapy, photodynamic therapy, and surgical excision [1]. Their incidence is associated with increasing age, male gender, fair skin pigmentation, and excessive sun (ultraviolet radiation [UVR]) exposure. They develop insidiously and have a propensity for local invasion. A small proportion incur locoregional lymph node metastases and more rarely, distant metastases [2].
NMSC includes basal cell carcinoma (BCC) and CSCC, and BCC represents a larger proportion of NMSC overall, as compared with CSCC [3]. Between 2011 and 2014, CSCC was being diagnosed at a rate of almost 1,000 cases per 100,000 persons in Australia, with a preponderance of those residing in geographical locations closer to the equatorial line with a tropical climate, and greater UVR exposure. CSCC has a much lower incidence in European countries [4]. Advanced disease (patients with locally invasive disease unamenable to resection, or those with locoregional and/or distant metastases) is far rarer than non-advanced (localised) CSCC [4]. The exact incidence of advanced CSCC is unclear due to variation in the recording practices of keratinocyte cancer registries [4]. In some jurisdictions, patients are only recorded in the first instance of CSCC despite having multiple lesions, or a registry may only take account of them should they require surgery. Survival worsens depending on the degree of progression. Different authors use different definitions of advanced disease further mystifying rates of survival in these groups. Venables, et al. [5] retrospectively analysed a cohort of over 70,000 from the United Kingdom national cancer registry from 2013-2015, of which 2.1% had metastatic disease. In those with metastatic CSCC, 3-year relative survival rates were 0.46 in men and 0.29 in women. Robsahm, et al. [6] retrospectively audited over 30,000 cases of CSCC from the Norwegian cancer registry documented over a 48-year period. Advanced disease in this study was defined to include local infiltration into adjacent structures, as well as metastatic disease. Relative 5-year survival rates for localised disease were 0.82 in men, and 0.88 in women, while for advanced disease these rates were 0.51 in men, and 0.64 in women.
Tumour characteristics that increase the likelihood of metastasis include: tumour location (lip, ear, face, genitalia, hands or feet); horizontal tumour size (greater than 2 cm); depth of invasion (greater than 2 mm); tumour multiplicity; histological subtype, specifically the desmoplastic, acantholytic and de novo variants; differentiation (anaplastic lesions confer higher risk); perineural invasion; lymphovascular invasion; local recurrence following excision; and emergence in areas of chronic inflammation, scarring or previous burns [7-9]. Perineural invasion occurs by direct tumour invasion of nerves and is thought to involve complex interactions mediated by a variety of neurotrophic factors. It associates with more aggressive tumour behaviour and may be a low-resistance pathway of dissemination of tumour cells [10]. Lesions that develop in an immunosuppressed individual may be prone to more malignant behaviour. The immune system plays a vital role in preventing oncogenesis, and immunosuppression is associated with increased rates of metastasis [11]. Degree of immunosuppression, duration, and immunosuppressant medication regimens with more agents and higher doses, associate with tumours that display more aggressive biological behaviours [2,12].
Cerebral metastases from a primary CSCC are exceptionally rare and are considered a grim prognostic development [13,14]. Metastasis is thought to occur by migration via haematogenous, lymphovascular and perineural routes, and in non-cutaneous head and neck squamous cell carcinoma (SCC), by direct invasion of tumours through the skull base. To our knowledge, only three cases have been reported in the medical literature previously. In the present study, we report a patient with a high-grade cerebral metastasis, originating from a CSCC primary lesion. This study highlights patient and tumour characteristics associated with this malignant phenotype and is written to expand the literature concerning this rare sequela.
A 70-year-old Caucasian male patient presented to our tertiary centre with a subacute change in his cognition and behaviour. He had a past medical history significant for long-standing Crohn's disease, childhood burns across his chest, and immunosuppression-related NMSC of his limbs, torso, and scalp. He had previously worked as a draftsman and was a lifelong non-smoker and teetotaller. In his thirties, a series of Crohn's flares led to three small bowel resections, and a longstanding regimen of immunosuppressive medications (prednisone and azathioprine). These were discontinued in 2015 after 30 years, due to recent progression of multiple NMSC lesions. In 2016, a large left-sided chest wall CSCC with associated axillary lymphadenopathy had developed, prompting surgical treatment with wide local excision and axillary lymph node dissection, followed by adjuvant radiotherapy. This lesion had multiple high-risk characteristics including that it had occurred over a pre-existing scar and had a deep tumour thickness (17 mm). There was evidence of vascular invasion, but no perineural invasion. The tumour invaded the subcuticular tissue, and 2/27 lymph nodes excised had metastatic deposits. Histopathology demonstrated anaplastic differentiation.
Our patient initially presented to his local medical officer with a 3-week history of vagueness, worsening memory, personality changes and confusion. His neurological examination was otherwise unremarkable. Magnetic resonance imaging (MRI) demonstrated a left frontal cerebral lesion involving the cortex and subcortical white matter. It had a lobulated appearance with multiple foci of intralesional petechial haemorrhage, central necrosis, and surrounding vasogenic oedema. It enhanced heterogeneously with gadolinium contrast. Regular oral dexamethasone was commenced to attenuate the local oedema. Computed tomography (CT) of the chest, abdomen and pelvis was performed to discern a primary cancer. The only finding was that of a right-sided lateral perifissural pulmonary nodule, 7 mm in diameter. This was further characterised with positron emission tomography (PET)/CT which demonstrated trace fluorodeoxyglucose (FDG)-avidity favouring a benign aetiology. Serial CT imaging demonstrated this lesion's morphological stability over an 18-month period. The radiology of this case is depicted in Figure 1.
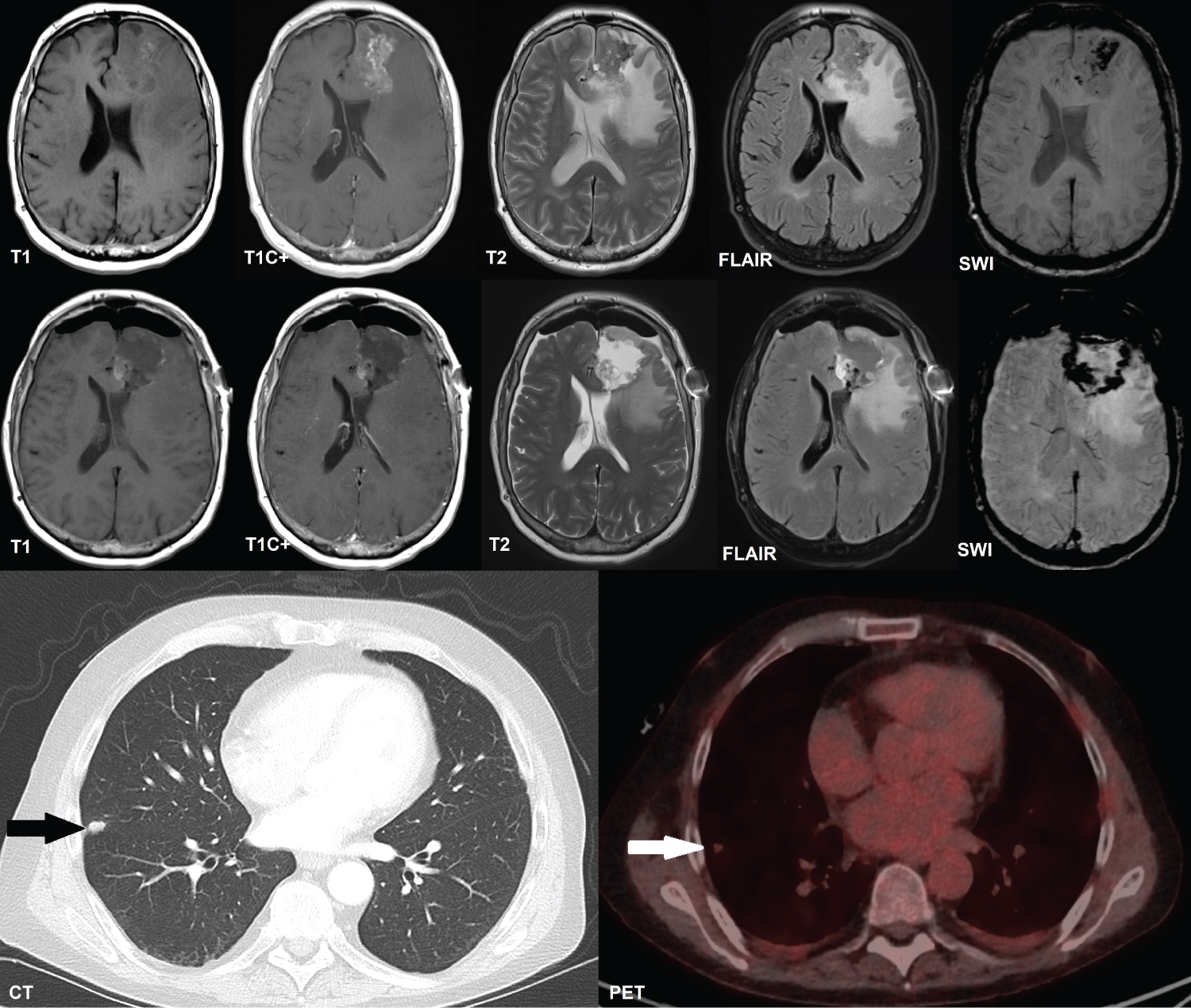 Figure 1: Axial cerebral MRI and thoracic contrast-enhanced CT and PET/CT. Top row: MRI demonstrating our patient's left frontal cerebral metastatic lesion prior to surgery; Middle row: Post-operative imaging demonstrating the extent of resection and residual tumour. There is pneumocephalus present, and haemorrhage into the surgical cavity; Left bottom panel: Thoracic CT with a black arrow indicating the right middle lobe lateral perifissural nodule observed; Right bottom panel: Thoracic PET/CT showing the trace FDG-avidity of this nodule, indicated by a white arrow.
Figure 1: Axial cerebral MRI and thoracic contrast-enhanced CT and PET/CT. Top row: MRI demonstrating our patient's left frontal cerebral metastatic lesion prior to surgery; Middle row: Post-operative imaging demonstrating the extent of resection and residual tumour. There is pneumocephalus present, and haemorrhage into the surgical cavity; Left bottom panel: Thoracic CT with a black arrow indicating the right middle lobe lateral perifissural nodule observed; Right bottom panel: Thoracic PET/CT showing the trace FDG-avidity of this nodule, indicated by a white arrow.
CT: Computed Tomography; PET: Positron Emission Tomography; MRI: Magnetic Resonance Imaging; T1: T1-Weighted Imaging; T1C+: T1-Weighted Imaging With Gadolinium Contrast; T2: T2-Weighted Imaging; FLAIR: Fluid-Attenuated Inversion Recovery; SWI: Susceptibility-Weighted Imaging; FDG: Fluorodeoxyglucose
View Figure 1
A primary glial tumour was suspected, and glioblastoma was thought likely. Metastatic disease was deemed improbable. Stereotactic pterional craniotomy was performed to resect the left frontal lesion. Histopathology and immunohistochemical staining demonstrated positive staining for cytokeratin 5/6 (Ck5/6) and subunit beta of interleukin 12 protein subunit 40 (P40), consistent with a diagnosis of metastatic anaplastic SCC. Staining for pulmonary malignancy markers thyroid transcription factor-1 (Ttf-1) and Napsin A was negative. Staining for GATA binding protein 3 (Gata-3) which marks differentiated SCC of cutaneous origin was negative. Histopathological comparisons of the cerebral lesion and several of the cutaneous lesions were made. The 2016 chest wall lesion and the 2020 cerebral lesion were similar in terms of histopathological morphology and cytology (they showed similar cytological atypia and amorphous architecture), and they shared the immunohistochemical profile outlined above. There were no other likely candidate lesions of origin. The histopathology of this case is depicted in Figure 2.
 Figure 2: Histopathological comparison of tumour specimens from various sites of resection. Top left panel: Chest wall lesion resected in 2016 at 50× magnification; Top right panel: Cerebral metastasis and adjacent neural tissue resected in 2020, from the left frontal lobe at 100× magnification; Bottom left panel: Chest wall lesion resected in 2016, showing extensive invasion of a blood vessel by tumour with tumour thrombus at 50× magnification; Bottom right panel: Metastatic deposit in an axillary lymph node resected in 2016 at 50× magnification. Note the central necrotic material and surrounding lymphoid tissue. The tumour cells in all panels demonstrate marked cytological and nuclear atypia, absent intercellular bridges, and minimal/absent keratinisation, characteristic of anaplastic squamous cell carcinoma.
View Figure 2
Figure 2: Histopathological comparison of tumour specimens from various sites of resection. Top left panel: Chest wall lesion resected in 2016 at 50× magnification; Top right panel: Cerebral metastasis and adjacent neural tissue resected in 2020, from the left frontal lobe at 100× magnification; Bottom left panel: Chest wall lesion resected in 2016, showing extensive invasion of a blood vessel by tumour with tumour thrombus at 50× magnification; Bottom right panel: Metastatic deposit in an axillary lymph node resected in 2016 at 50× magnification. Note the central necrotic material and surrounding lymphoid tissue. The tumour cells in all panels demonstrate marked cytological and nuclear atypia, absent intercellular bridges, and minimal/absent keratinisation, characteristic of anaplastic squamous cell carcinoma.
View Figure 2
Our patient's post-operative course was complicated by the development of a multi-resistant polymicrobial infection of the surgical site and bone flap, necessitating its removal. The following 2 months were punctuated by episodes of recurrent nosocomial sepsis, blood dyscrasias, seizures and various biochemical abnormalities requiring a lengthy hospital admission. Post-operative radiotherapy was initially planned, however due to concerns of possible wound breakdown in the context of recent multiple surgeries, substantive infection, and previous radiotherapy to an adjacent scalp lesion, this was reconsidered and abandoned. His post-operative condition was tenuous and his cognition frail. He was deemed an inappropriate candidate for systemic therapy. Despite several torrid months, our patient recovered from his infection, underwent cranioplasty, and was eventually discharged to the care of his family and his own home. In the community, he was blighted by cognitive and behavioural issues. His tumour recurred less than 12 months after his initial surgery, and he underwent repeat craniotomy. His post-operative recovery was again complicated by nosocomial infection, and he was palliated. He died in-hospital 13 months following his initial surgery.
We have reported the case of a chronically immunosuppressed male patient with biologically aggressive left frontal cerebrally metastatic anaplastic CSCC, treated with surgery. Initial pan CT and PET/CT imaging were unremarkable, except for a small pulmonary nodule which for reasons described previously, was unlikely to represent the lesion of origin. No further investigations of this nodule were pursued. Ahn, et al. [15] performed a retrospective audit of 128 high-risk patients (long-term cigarette smokers) with perifissural pulmonary nodules discerned following thoracic CT. They concluded that almost all of these nodules, even those in patients with significant risk factors, were lymph nodes. No subjects within that study developed lung cancer from these lesions within a 7.5-year follow-up period. Anaplastic SCC is typically FDG-avid [16]; our patient's pulmonary nodule was not. There are immunohistochemical markers that have utility in determining the tissue origin of SCC. Gata-3 is a transcription factor commonly expressed in differentiated CSCC, and rarely in pulmonary SCC. Gata-3 expression is downregulated or absent in anaplastic CSCC and is thus limited in its utility to identify the tissue origin of poorly differentiated lesions [17]. Our patient's cerebral lesion stained negatively for Gata-3; an inconclusive finding. The cerebrum and chest wall CSCC were similar lesions with respect to their histopathology and immunohistochemistry. There was no likely alternative lesion of origin detected radiologically, and all prospective skin lesions were CSCC.
The same factors that presuppose an aggressive CSCC phenotype associate with poor prognoses. Our patient is notable for an almost perfect constellation of all known high-risk factors that predispose to more aggressive disease. Immunosuppression, lesion multiplicity, deep tumour thickness, large horizontal tumour size, underlying scar, lymphadenopathy, perineural and vascular invasion, and anaplastic differentiation, predicted or associate with aggressive tumour behaviour and our patient's poor outcome [2]. Burton, et al. [9] reviewed the factors underpinning adverse outcomes in CSCC, the most important of which was depth of invasion (sometimes called Breslow thickness, despite the eponym's primary use in melanoma). The absolute numerical measurement of depth of invasion is thought less important than the presence of invasion beyond the subcutis (despite the assertion that depths of invasion greater than 2 mm are riskier). Particular CSCC subtypes are associated with a worse prognosis, while conversely, some subtypes are considered especially indolent and unlikely to metastasise. The verrucous variant, and most that develop from actinic keratoses are the best examples of lesions with a favourable prognosis. Tumours with more dedifferentiation and those forming nests, strands and demonstrating desmoplasia, are thought to confer a worse prognosis. Immunosuppressed patients are known to have higher rates of CSCC metastasis (ranging from 7-29% depending on the context in which they are immunocompromised) [9,18]. Immunosuppressed patients with a worse "tumour, nodes, metastasis" (TNM) classification were found to have disproportionately higher rates of metastasis when compared with immunocompetent ones, while those with a more favourable classification demonstrated rates that were comparable to their immunocompetent counterparts.
There are few cases of cerebrally metastatic CSCC in the medical literature. Kitano, et al. [1] reported the case of an 84-year-old man with a pedunculated erythematous scrotal mass that under histopathological examination was revealed to be CSCC with adjacent extramammary Paget's disease. He had incurred inguinal lymph node and cerebral metastases and was treated with whole brain irradiation. Scrotal CSCC is more commonly metastatic than other anatomical locations [2]. It is the most common scrotal malignancy and differs from non-scrotogenital CSCC in the factors that predispose to it. Human papillomavirus (HPV) infection, psoralens, and ultraviolet light treatment of scrotal psoriasis, or trapping of carcinogens in scrotal rugae due to occupational behaviours, are linked to its pathogenesis [19]. Salvati, et al. [20] reported a 54-year-old man with a lower dorsal moderately differentiated CSCC with inguinal and para-aortic lymph node and cerebellar metastases, treated with surgery, then cisplatin and whole brain irradiation. Vu, et al. [21] reported a 48-year-old male patient with locally recurrent right scapular HPV-associated basaloid CSCC that metastasised to axillary lymph nodes and his right occipital lobe, and was treated with surgery followed by stereotactic radiosurgery.
Ours is only the fourth case of distant CSCC with cerebral metastases described in the medical literature. The blood brain barrier functions to prevent metastatic cells from migrating into the central nervous system, yet some cancers preferentially migrate to the brain, overcoming this [22]. Salvati, et al. [20] posited that organ/site specific metastases occur when an appropriate milieu of growth and inhibitory factors at those sites, favours metastatic migration and implantation of cancer cells. Melanoma commonly metastasises to the brain because of the tissues' shared origin in the neural crest. This has been shown to occur through oncogenic reactivation of transcription of dormant genes involved in embryological migration [23]. A similar process may explain the observation of a cerebral metastasis as in our case although clearly this is uncommon. If so, it occurs only stochastically and rarely, and probably requires very specific circumstances.
The gold standard of diagnosis of cerebral lesions is histopathological assessment with immunohistochemistry, while the radiological modality of choice is gadolinium contrast-enhanced MRI [24]. Contextual information such as a known primary cancer, or a pan CT scan that detects a primary lesion, are useful, and may provide alternative biopsy targets if neurosurgery is impractical. Treatment may consist of surgery, chemotherapy, immunotherapy and/or radiation. Treatment choices require consideration of a patient's individual circumstances in terms of their function and comorbidities, and these patients are best managed cooperatively by radiologists, neurosurgeons, and medical and radiation oncologists [25].
Multiple risk factors and features contribute to more aggressive CSCC behaviour in terms of local invasion and metastases. Immunosuppression is a significant risk factor, especially of lesions that are more advanced at diagnosis. Immunosuppressed patients should be monitored closely for the emergence and progression of NMSC. High-risk lesions should be resected or ablated, given the dangers of local invasion and metastatic spread. While exceptionally rare, physicians should be aware of the possibility of distantly metastatic CSCC in the differential diagnosis of a cerebral lesion, in patients with a positive history. Best outcomes require multidisciplinary management including dermatology expertise.