Background: Cervical spondylotic myelopathy can mimic an intramedullary tumor.
Case presentation: We report a case of a young male who presented with gradually progressive myelopathy. MRI cervical spine with contrast revealed a contrast enhancing lesion. Anterior cervical discectomy with fusion was done.
Conclusion: In case of a progressive cervical myelopathy with atypical radiographic appearance initial decompression and follow-up with an MRI might be the procedure of choice, if a clear diagnosis for a causative treatment cannot be made.
Myelopathy, Intramedullary tumour, Spinal cord edema
We report a case of 54-year-old male who presented with gradually progressive loss of dexterity, leg weakness, gait disturbance and urinary problems for last 3 months. There was no relevant past medical history. MRI cervical spine showed T2 hyperintense signal at C4/C5 with cord expansion (Figure 1A). Post contrast MRI revealed an area of enhancement in the cord at C5 (Figure 1B and Figure 1C). As cervical cord is a dynamic structure, a flexion-extension MRI revealed a disc at C4/C5 level (Figure 1D).
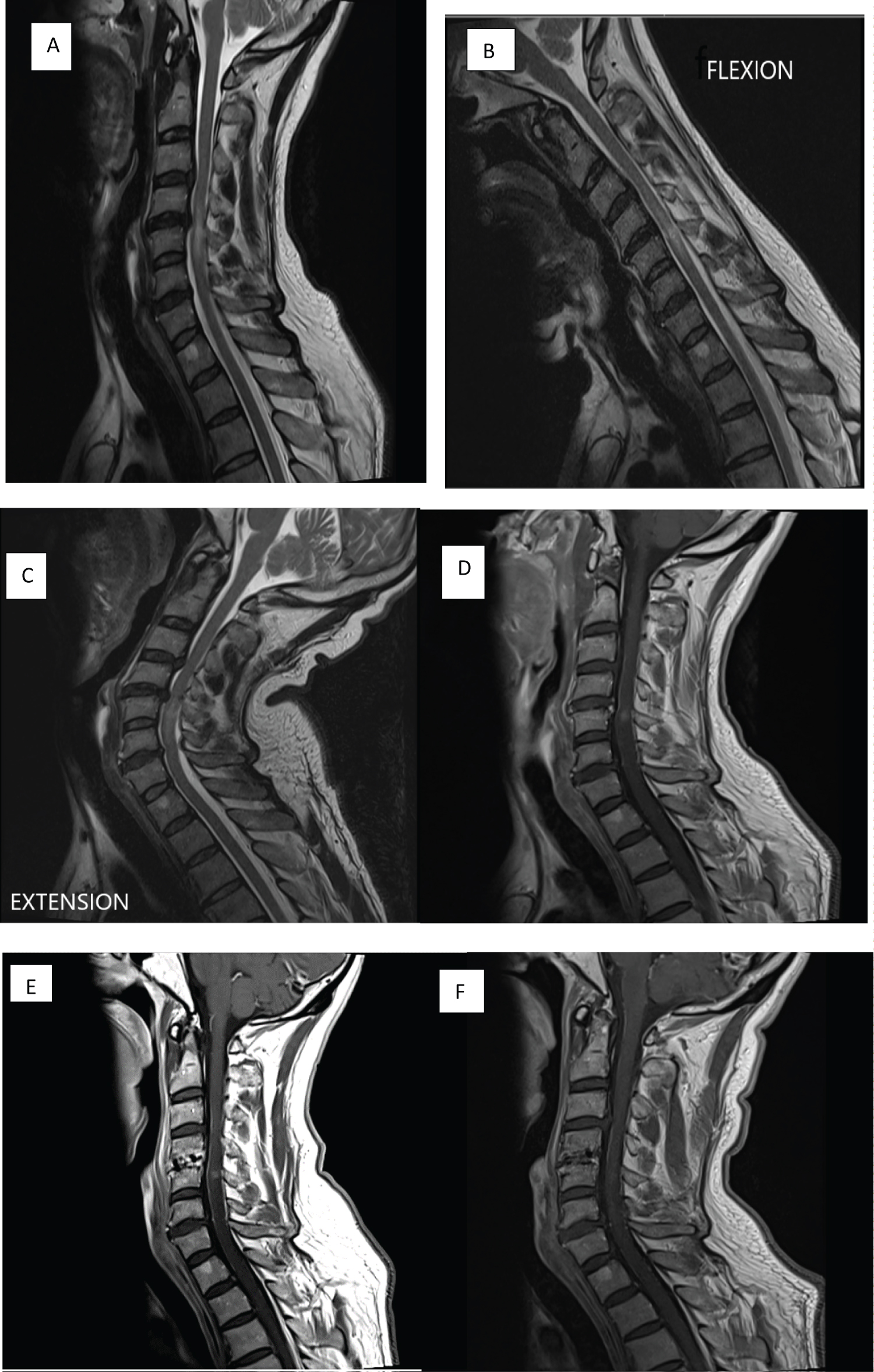 Figure 1: (A) Preoperative MRI cervical spine T2W1 shows hyperintensity in the region of C4/C5 with cord swelling and disc osteophyte complex; (B & C) Preoperative MRI cervical spine T2W1 flexion and extension views shows compression of spinal cord at C4/C5 during extension only; (D) Preoperative MRI cervical spine T1W1 with contrast shows contrast enhancement at C4/C5 level; (E) Postoperative MRI cervical spine T1W1 with contrast at 6 months shows slight reduction in enhancement at C4/C5 level; (F) Postoperative MRI cervical spine T1W1 with contrast at 12 months shows almost complete resolution of enhancement at C4/C5 level.
View Figure 1
Figure 1: (A) Preoperative MRI cervical spine T2W1 shows hyperintensity in the region of C4/C5 with cord swelling and disc osteophyte complex; (B & C) Preoperative MRI cervical spine T2W1 flexion and extension views shows compression of spinal cord at C4/C5 during extension only; (D) Preoperative MRI cervical spine T1W1 with contrast shows contrast enhancement at C4/C5 level; (E) Postoperative MRI cervical spine T1W1 with contrast at 6 months shows slight reduction in enhancement at C4/C5 level; (F) Postoperative MRI cervical spine T1W1 with contrast at 12 months shows almost complete resolution of enhancement at C4/C5 level.
View Figure 1
A differential diagnosis of intramedullary tumour or myelopathy due to disc degeneration was made. The diagnosis of inflammatory lesion was ruled out as workup of inflammatory marker and CSF examination was clear. The case was discussed in spinal multidisciplinary team (MDT) and it was agreed to do anterior cervical discectomy with standalone cage at C4/C5.
Post-operative follow up surveillance MRI done in the immediate post-operative period did not show any change. A 6-month post-operative MRI showed a reduction in the contrast enhancement (Figure 1E). A 12-month post-operative MRI showed complete resolution of contrast enhancement and cord edema (Figure 1F). Patient improved neurologically and his gait became better.
Many non-neoplastic intramedullary pathologies can mimic intramedullary tumours. These include edema due to myelopathy, demyelination, granulomatous disease, infections, radiation myelopathy, vascular lesions, and syringomyelia [1]. Hyperintense T2-weighted lesions may reflect focal spinal cord edema and may enhance with gadolinium at the site of maximal cord compression (e.g., chronic cervical compression and spondylotic changes) [1,2]. However, intramedullary contrast enhancement of the spinal cord may also indicate the presence of an infectious or neoplastic process [3].
Sasamori, et al. reported 3 cases of non-neoplastic lesions mimicking intramedullary tumour on T2-weighted MRI and cord swelling and gadolinium enhancement [2]. Takahashi, et al. studied MRI scans of 668 patients with spondylotic cervical myelopathy (CM) and found only 1 patient displayed contrast enhancement due to cervical herniated disc and spondylosis at C3-C4 level [3]. Lee, et al. presented 6 patients with spondylotic CM whose postoperative MRI revealed spinal cord swelling with abnormal gadolinium enhancement. The authors suggested that spinal cord edema was possibly induced by venous- and cerebrospinal fluid (CSF) circulation disturbance due to spinal cord compression [4]. Boet, et al. suggested that the presence of spinal cord enhancement was consistent with cord substance disruption or reorganization, resulting in a blood-brain barrier breakdown and contrast uptake [5]. Cabraja, et al. also reported a similar case in which the lesion was felt to be neoplastic and was biopsied [6].
In our case, there was no spinal cord compression in flexion MRI and minimal compression in neutral position MRI. Only on extension MRI, spinal cord compression was seen, revealing the dynamic nature of the compression. This dynamic MRI findings suggest that transient but repetitive cord compression is associated with spinal cord swelling and Gd enhancement. Terae, et al. speculated that the enhancement reflects vascularized granulation in a reparative phase [7].
Spinal cord edema is a rare condition in patients with cervical spondylosis and an accurate diagnosis and timely surgery are necessary for cure. It must be considered in spondylosis patient manifesting as intramedullary lesion on MRI of cervical spinal cord. Initial decompression and radiological surveillance might be the procedure of choice in these cases if a clear diagnosis cannot be made.
Not applicable.
Obtained from the patient.
Not applicable.
None.
None.
Atul vats - Conceptualization, writing of case report, editing, proof reading; Shahid khan - Conceptualization, Proof reading; Farooq Aziz - Final editing and proof reading.
None.
None.