Pineal region tumors are classically presented with vertical gaze palsy, hypothalamic symptoms, or, more often, hydrocephalus, by obstructing the aqueduct. This case report describes a patient with obstructive hydrocephalus and a hearing loss as an initial complaint of pineal region tumor. The patient started to behave aggressively after falling and stopped hearing what his family was saying. Although he could read and speak, most of the time he was not able to understand where he is and attempted multiple times to escape from the hospital. Detailed neurological examination was significant only for slight horizontal nystagmus. The first operation was the placement of external ventricular drainage and the second one was tumor removal. Aggressive behavior stopped after the first operation and hearing loss completely resolved after tumor removal.
Pineal region, Hearing loss, Solitary fibrous tumor/haemangiopericytoma (SFT/HPC)
To our knowledge, no case reports described solitary fibrous tumor/haemangiopericytoma in the pineal region with an initial complaint of hearing loss and complete recovery after the operation in an adult patient.
Pineal region tumors are classically presented with vertical gaze palsy, so-called Parinaud syndrome, or, more often, the hydrocephalus, by obstructing the aqueduct [1]. The hearing loss in the pineal region is usually described as "pure tone and speech hearing impairment" and in previous publications; the rate of bilateral hearing loss in the case of pineal region tumor was only 22% among all reported cases [2]. Only 4 cases were identified in the PubMed search of solitary fibrous tumor/haemangiopericytoma in the pineal region [3-6]. However, none of them described hearing loss as the main complaint. The case report represents the anatomical importance of the pineal region as a potential cause of hearing loss, which can be regained.
In this case report, we would like to present to you a 44-years-old man, with an initial complaint of hearing loss and inadequate behavior. According to his wife, he fell in April 2021 and afterward became strange and lost his ability to hear, he was emergently hospitalized in the district hospital, where he underwent magnetic resonance imaging (MRI), which showed a tentorial tumor with subtentorial growth, compressing the quadrigeminal plate and causing obstructive hydrocephalus by compressing aqueductus (Figure 1).
After transferring to 'National Center for Neurosurgery' in August 2021, he was gone through a detailed neurological examination. He was unable to perceive speech but could speak and read. No limitation of upward gaze was noted, but only slight horizontal nystagmus. Sensory deficits were difficult to assess because his uncooperative behavior and motor function were intact. Unfortunately, no audiogram could be possibly performed in our hospital. The patient's wife got the consent for the operation and detailed anamnesis.
He was prepared for surgery on the following day. Preoperative preparation included intravenous steroid injection two times per day, mannitol and furosemide once daily for three days. The decision was made to divide the operation into two steps: Firstly, to solve his obstructive hydrocephalus, it was necessary to perform external ventricular drainage (EVD) and 2 days later perform resection of the tumor.
EVD was performed through right Kocher's point. The pressure was set at 15 cmH2O. CT scan after external ventricular drainage placement is shown in Figure 1C. To note he became less inadequate and aggressive after the first operation.
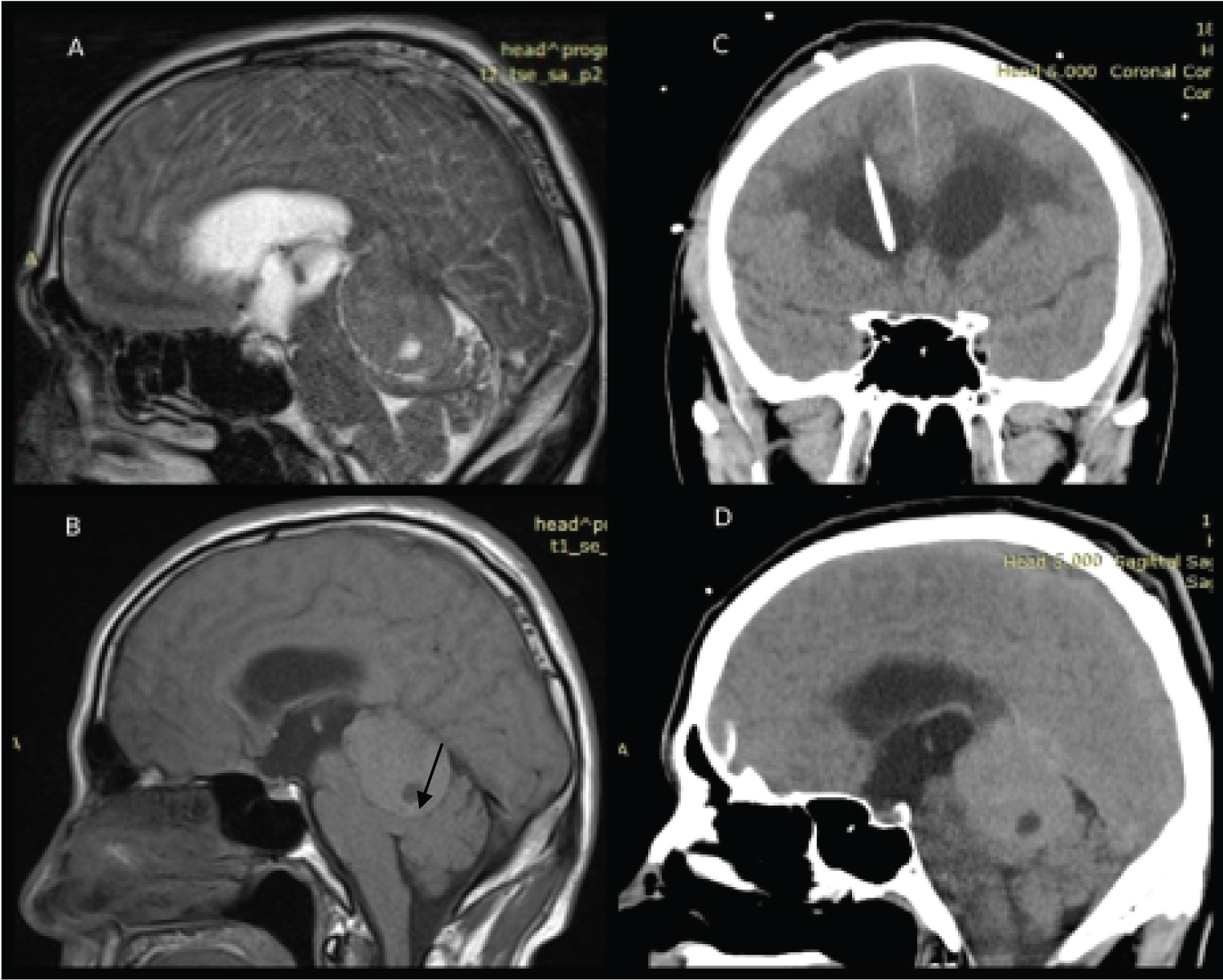 Figure 1: A) MRI shows encapsulated 4.25 × 3.15 × 2.89-cm in size tumor with hyper-signal intensity on T2WI, and heterogeneous slightly long/short signal on T1WI; B) The area of necrosis is also shown (arrow); C) Coronal CT scan of the patient after the placement of external ventricular drainage; D) Sagittal CT scan of the head showing solitary, irregularly contoured mass. To note, these CT scans were made 10 days later after the initial MRI scanning with signs of slight tumor increase.
View Figure 1
Figure 1: A) MRI shows encapsulated 4.25 × 3.15 × 2.89-cm in size tumor with hyper-signal intensity on T2WI, and heterogeneous slightly long/short signal on T1WI; B) The area of necrosis is also shown (arrow); C) Coronal CT scan of the patient after the placement of external ventricular drainage; D) Sagittal CT scan of the head showing solitary, irregularly contoured mass. To note, these CT scans were made 10 days later after the initial MRI scanning with signs of slight tumor increase.
View Figure 1
The decision was made to perform a midline supracerebellar infratentorial approach with the patient in a modified park-bench position (Figure 2A and Figure 2B). We prefer not to use a sitting position, instead, we place the patient in a modified park-bench position so the traction will help to open the quadrigeminal cistern. Two burr holes were made over the transverse sinus, afterward, a craniotome was used to connect the burr holes, and the bone flap was elevated. Dura was incised in a curvilinear fashion and opened to the top. The tenting sutures over the tentorium were placed to expand the operative corridor. After the tentorium was released, the operative corridor was gone through incisures, where the tumor was founded. It is important that the midline vermian bridging vein was saved, which is seen in the video. External detachment of the tumor was performed with the combination of the suction tube and bipolar forceps to safely unplug the tumor from vascular structures. En bloc complete tumor removal with the capsule was achieved. The final steps were aimed at complete hemostasis with bipolar coagulation. The postoperative field was draped by Surgicel to provide hemostasis. Total blood loss was approximately 300 ml. The pericranial autograft was used for a watertight dural closure. The patient was observed in the intensive care unit for 1 day and the postoperative course included steroids, mannitol, and furosemide once daily. He also received one liter of isotonic NaCl solution for three days to prevent any electrolyte complications.
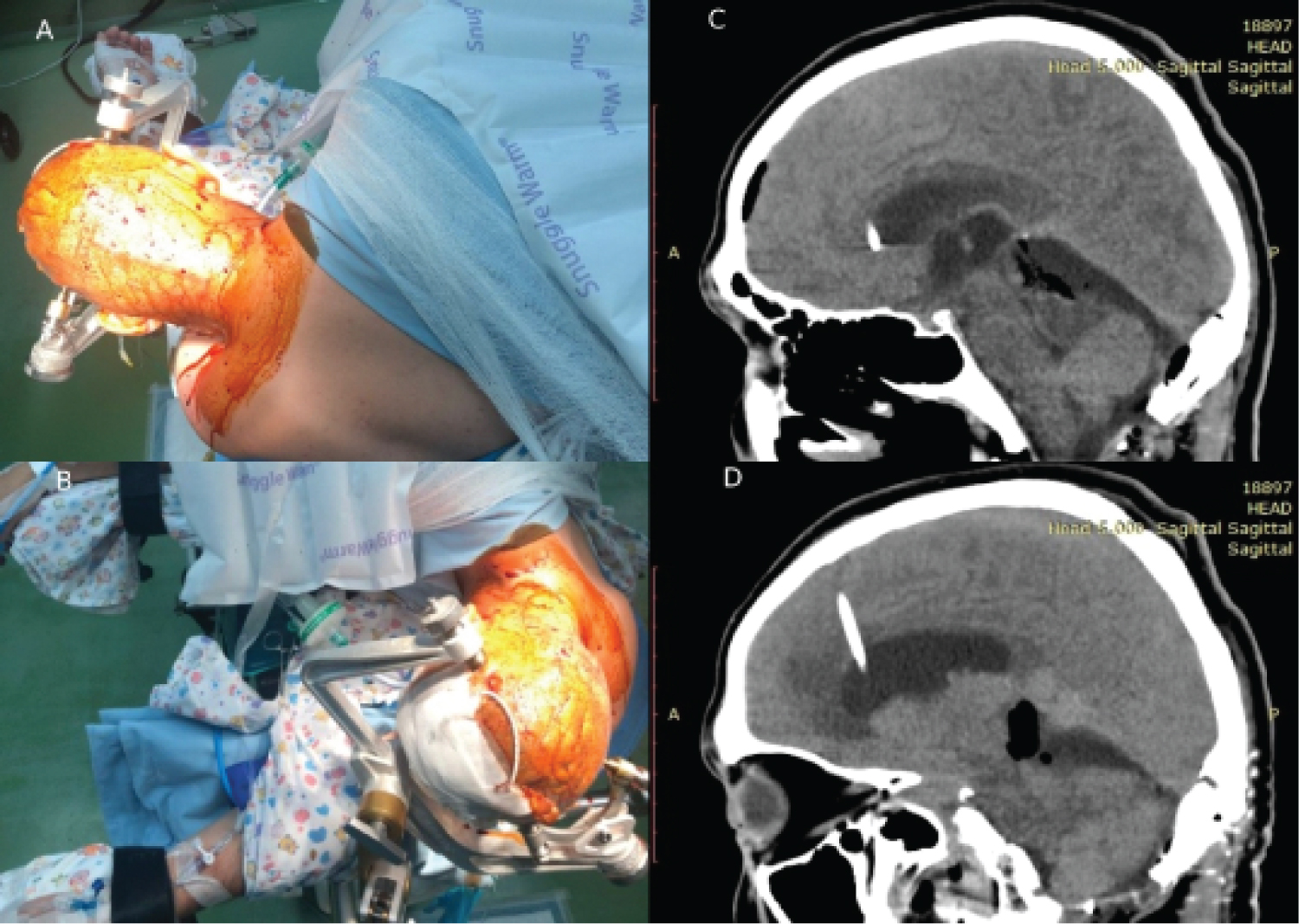 Figure 2: A,B) Patient position and the incision line are shown; C,D) Sagittal CT scans after gross total resection. The operative route is seen. No signs of complications.
View Figure 2
Figure 2: A,B) Patient position and the incision line are shown; C,D) Sagittal CT scans after gross total resection. The operative route is seen. No signs of complications.
View Figure 2
The video of the operation is acceptable by the link.
CT-control after the operation is shown in Figure 2C and Figure 2D. After the operation patient's hearing loss is completely resolved. The external ventricular drainage was removed three days later. He was discharged home on day eight after the second operation.
Tumor tissue was represented by rather dense sprawls rounded, oval, less often spindle-shaped cells, with dark hyperchromic cores. The cytoplasm was eosinophilic, and nuclei contained signs of pathological mitosis. There were numerous sinusoidal slits, capillaries, vessels, and vascular slits like "staghorn" lined with endothelium between cells. Large-scale hemorrhages and foci of necrosis were also seen (Figure 3A).
For differential diagnosis with anaplastic meningioma, the immunohistochemical study was conducted on a standard protocol, using the company's visualization system «Dako». Tumor cells were diffusely positive for STAT6 and vimentin, focal-positive to CD34 (Figure 3B and Figure 3C), and negative for EMA and progesterone. The index of proliferative activity Ki67 was not more than 10%.
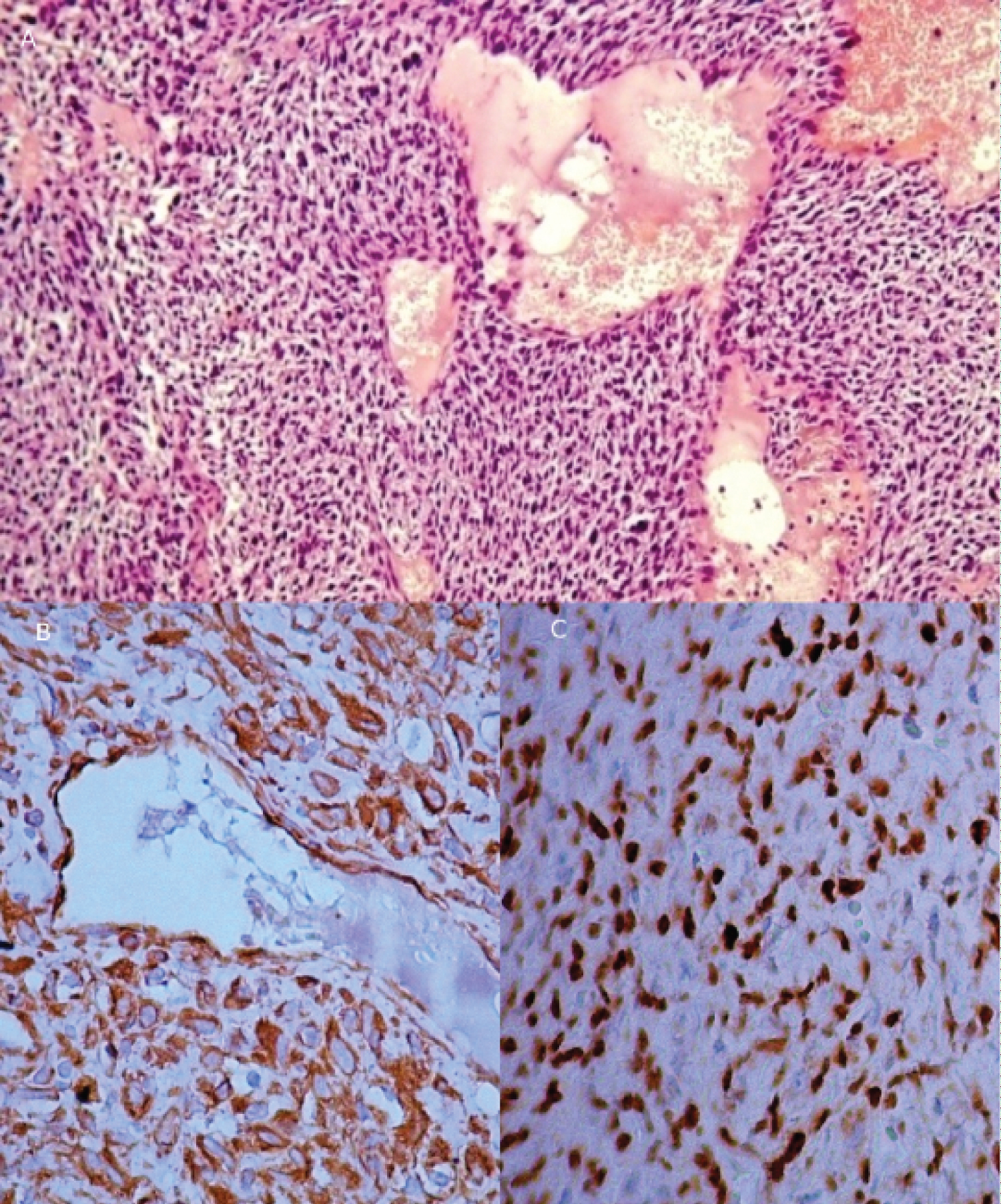 Figure 3: A) Solitary fibrous tumor/haemangiopericytoma, WHO grade II; B) The positive reaction of tumor cells to CD34; C) Nuclear localization of STAT6 protein.
View Figure 3
Figure 3: A) Solitary fibrous tumor/haemangiopericytoma, WHO grade II; B) The positive reaction of tumor cells to CD34; C) Nuclear localization of STAT6 protein.
View Figure 3
Based on pathohistological and immunohistochemical studies of solitary fibrous tumor/haemangiopericytoma diagnosis, WHO grade II, ICD-O code 8815/3 was established.
The patient had radiotherapy 3 months after the operation and had a postoperative MRI control 3 months after radiotherapy. The patient can hear and his behavior is adequate. There are sometimes problems with walking, which are becoming better in time. MRI shows that the postoperative corridor has no complications; there are no signs of tumor growth in the previous place, but there are supratentorial signs of tumor growth (Figure 4). The latest might be considered for Gamma Knife Radiosurgery at our hospital.
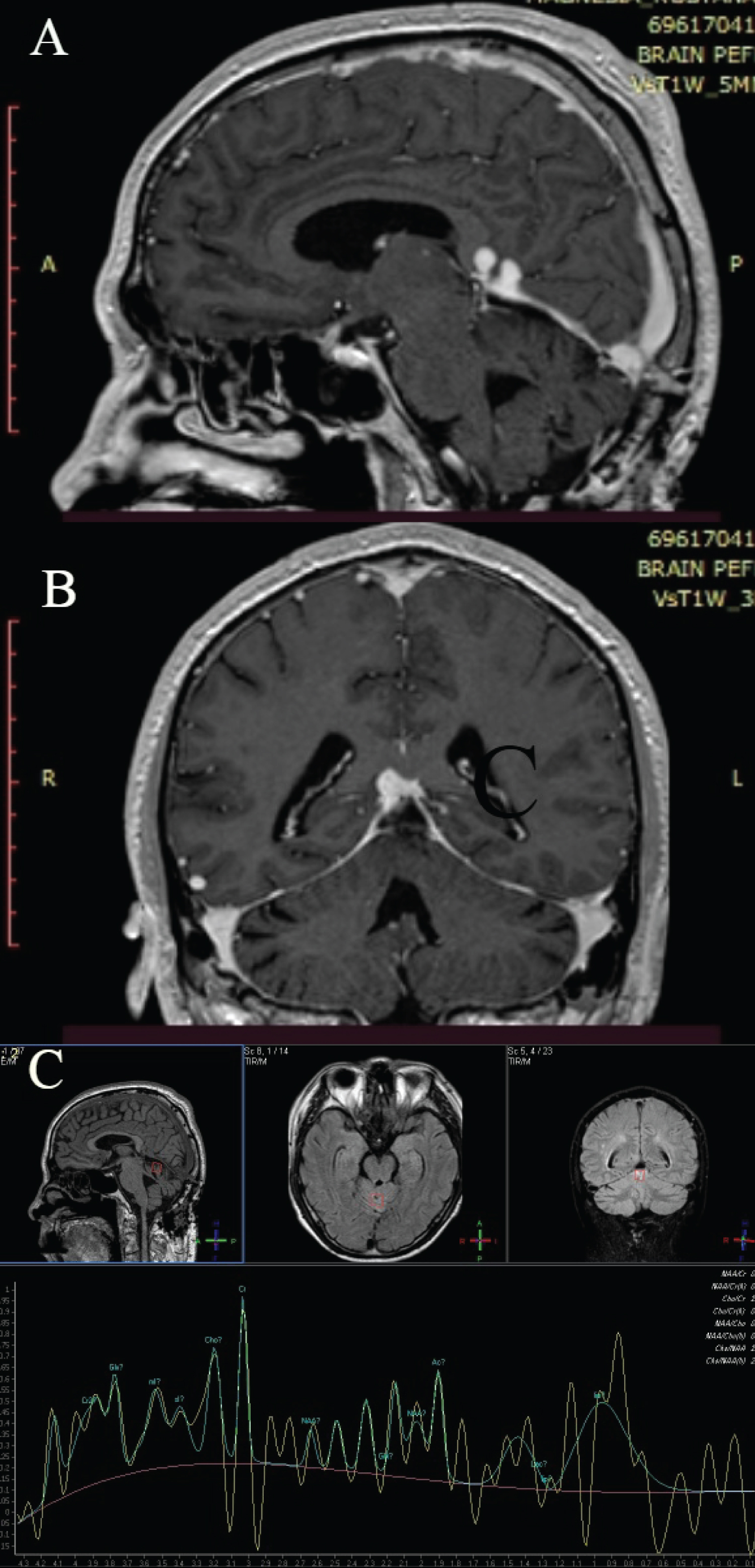 Figure 4: Postoperative follow-up. A) Sagittal T2WI image that shows supratentorial part; B) Coronal T2WI image; C) Conventional MR spectroscopy that shows increased creatinine.
View Figure 4
Figure 4: Postoperative follow-up. A) Sagittal T2WI image that shows supratentorial part; B) Coronal T2WI image; C) Conventional MR spectroscopy that shows increased creatinine.
View Figure 4
Rene Descartes described the pineal gland in his last book in the 17th century, 'The Passions of Soul', where he regarded it as "the principal seat of the soul and the place in which all our thoughts are formed" [7]. Two centuries later the pineal gland is believed to be the third eye or Ajna chakra by Madame Blavatsky [8]. Nowadays, the pineal gland and its surrounding region are still full of mystery. Hearing loss caused by compression of the inferior colliculus represents an interesting anatomic case.
The inferior colliculus (IC) is responsible for integrated sound localization, as it is the first site in which the influx of cells carrying horizontal and vertical sound localization data from each ear converges. The central nucleus of the IC is an important site of an auditory input [9]. Glutamatergic cells project from the V and VI layers of the auditory cortex, mainly to the ipsilateral IC, with most of the cortical input coming from the V layer. This cortical input allows for downward modulation of the frequency, intensity, duration, and response of the IC. The location of auditory stimuli, and the discrimination of several different sound sources, may play a significant role [10]. The main outflow of the IC passes through the brachium of the inferior colliculus to stimulate the medial geniculate nucleus of the thalamus [11].
Solitary fibrous tumor/haemangiopericytoma (SFT/HPC) accounts for < 1% of all primary CNS tumors and most commonly affects people in the fourth to sixth decade of life [12].
HPC was described in 1942 by Stout and Murray, and the first mention of CNS HPC was done by Begg and Garret in 1954 [13,14]. HPC is a highly vascularized mesenchymal tumor that develops from pericytes that comprise the walls of capillaries and postcapillary venules with aggressive behavior [13,15]. Aggressive behavior of SFT/HPC includes a high local recurrence rate and distant or so-called "drop" metastases [14,16,17].
MRI findings usually include heterogeneous signal intensity, intense enhancement of T2 signal, low signal intensity lines within the tumor on T2 images, heterogeneous signal intensity, and a ring-like band around the tumor on DWI [18]. According to different authors [18,19], hypointense lines inside the tumor on T2W1 images might be a helpful differentiating tool as they represent collagenous and fibrotic components of solitary fibrous tumor/haemangiopericytoma. Histopathological analysis helps in the diagnostic establishment. Higher histological grade and subtotal resection were associated with recurrence, while higher histological grade and recurrence were associated with metastases formation [19]. It is also noticed, that the relative ratios of myo-inositol, glucose, and glutathione concerning glutamate are higher in HPC compared to meningioma; whereas the relative ratios of creatine, glutamine, alanine, glycine, and choline-containing compounds concerning glutamate are lower in HPC compared to meningioma [20]. The grading system defines further therapy [21]. The underlying molecular biological mechanisms are still needed to be further explored [22]. The role of radiotherapy is still unclear [17].
Oppenheim and Krause reported the first successful resection of a pineal tumor in 1913 [23]. Krause described the infratentorial supracerebellar technique for the first time in the early twentieth century [24]. Because of limits in microsurgical technology, the technique was lost for many years until Stein [25] rediscovered it in 1971. The sitting position is not considered safe because of the risk of air embolism [26].
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
All authors contributed to the study's conception and design. All authors read and approved the final manuscript.