Background: Linear scleroderma, otherwise known as encoup de sabre (ECDS), is a form of scleroderma that affects the face and scalp and typically presents with unilateral streaks of induration with pigment changes of the skin which can involve the underlying dermis, soft tissue, and bone. In cases where there is progression to unilateral facial atrophy, this is known as parry-romberg syndrome (PRS). There are several case reports in the literature of ECDS/PRS with neurologic involvement including seizures, headache, vascular malformation, and abnormalities on neuroimaging. We present a case with intraparenchymal hemorrhage as a complication of ECDS.
Clinical presentation: An 11-year-old Hispanic female with a history of a midline cutaneous lesion of the forehead since age 2 and seizures since age 7 presented to the emergency department with left hemibody weakness and numbness. Head CT indicated right parietal intraparenchymal hemorrhage. Subsequent MRI indicated multifocal areas of right frontal, parietal, and temporal parenchymal calcifications. Selective catheterization and angiography of the cerebral vessels was performed twice with no evidence of vascular malformations.
Conclusion: Previously, cases of linear scleroderma have been reported with seizures and calcifications on neuroimaging. However, this presentation of a ECDS patient with hemorrhage into the cerebral parenchyma without a correlated vascular malformation is highly unusual and to our knowledge has never been reported.
Case report, Cerebral hemorrhage, En coup de sabre, Pediatric
AVM: Arterio-venous malformation; CNS: Central nervous system; CT: Computed tomography scan, ED: Emergency department; ECDS: Linear scleroderma en coup de sabre; MRI: Magnetic resonance imaging; PRS: Parry-Romberg syndrome
Scleroderma represents a spectrum of clinical entities which can be systemic or localized. En coup de sabre (ECDS) refers to a form of localized scleroderma affecting the face and scalp. Its name is derived from the characteristic linear indurated lesion with pigment changes resembling the cut of a sword. As with other forms of localized scleroderma, ECDS can involve the underlying dermis, soft tissue, bone, and intracranial structures [1,2]. Parry-romberg syndrome (PRS) refers to unilateral facial atrophy which can occur simultaneously or as a sequela of ECDS [2]. ECDS has been reported with neurologic involvement including seizures, headache, vascular malformation, and abnormalities on neuroimaging [3-5]. We present a unique case of ECDS where intraparenchymal hemorrhage occurred in the absence of an identifiable vascular malformation.
The patient's mother provided written consent for publication of her image.
We report an 11-year-old Hispanic female with a history of a midline cutaneous lesion of the forehead since age 2 and seizures since age 7. These symptoms began while the family lived in Central America, where she was diagnosed with a fungal infection and treated ineffectively with antimicrobial and antiepileptic drugs. After immigration to the United States, the patient was started on oral levetiracetam, valproate, and oxcarbazepine which reduced the frequency and duration of her seizures.
In the 2 weeks prior to her presentation to our ED, she had increased frequency of generalized seizures. Seizures lasted 1-2 minutes with horizontal gaze deviation and generalized convulsions. She presented to the ED with left hemibody weakness and numbness. Physical exam showed paralysis, hypotonia, and sensory deficit of the left side of the body. Exam also showed a hyperpigmented indurated plaque beginning at the nasal bridge, slightly to the right of midline, which extended towards the vertex past the hairline (Figure 1). Head CT (Figure 2) showed a 2.3 × 2.3 × 2.3 cm area of hemorrhage and surrounding vasogenic edema in right parietal lobe, which prompted a workup for vascular cause. Differential diagnoses included mycotic aneurysm, AVM, or cavernoma. CTA Head was negative for vascular malformations. MRI indicated multifocal areas of right frontal, parietal, and temporal parenchymal calcifications. Endovascular catheterization and angiography of the cerebral vessels was performed twice without showing evidence of vascular malformations.
 Figure 1: Photograph of the patient showing a linear, hyperpigmented, indurated plaque characteristic of ECDS.
View Figure 1
Figure 1: Photograph of the patient showing a linear, hyperpigmented, indurated plaque characteristic of ECDS.
View Figure 1
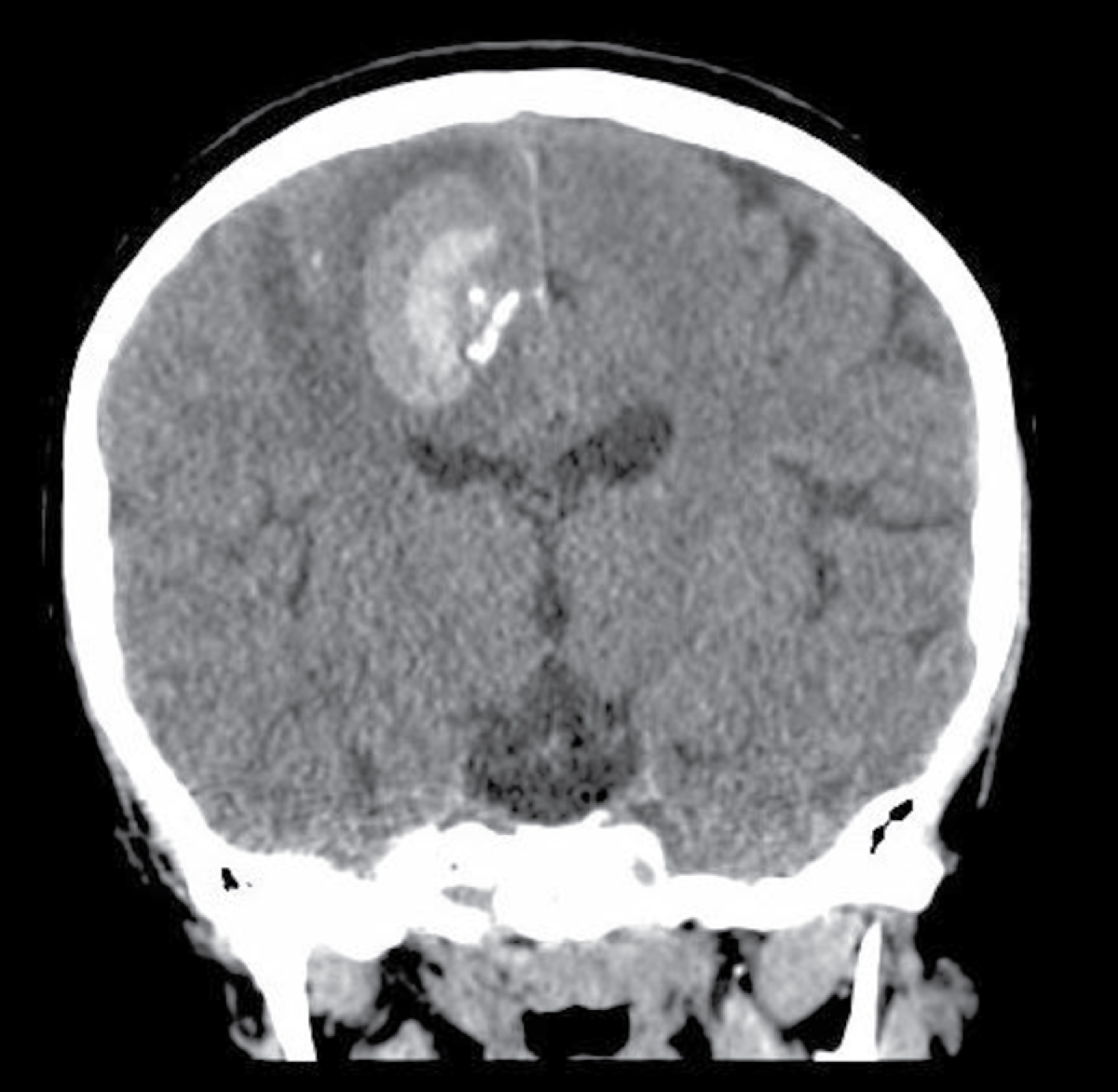 Figure 2: Coronal slice from head CT showing intraparenchymal hemorrhage in the right parietal lobe of a patient with ECDS.
View Figure 2
Figure 2: Coronal slice from head CT showing intraparenchymal hemorrhage in the right parietal lobe of a patient with ECDS.
View Figure 2
The diagnosis of ECDS was made based on clinical findings and history of neurologic symptoms. Methotrexate and methylprednisolone were initiated during hospitalization, and these therapies were continued after discharge along with her antiepileptic medications. At follow-up, the patient showed remission of seizure activity but still had residual left body weakness.
ECDS is a rare entity which is mostly described in case reports. Neuroimaging abnormalities found in these patients include calcifications, atrophy, vascular malformations and white matter lesions in the cerebral hemisphere ipsilateral to the side of the skin lesion. The relationship of these findings and neurological involvement in ECDS is poorly understood.
Multiple cases have been reported of hemorrhage into cavernomas in pediatric ECDS patients. A 13-year-old male with active ECDS on escalating immuno suppressants was reported to have a large frontoparietal hemorrhage, and MRI showed multiple cavernomas in the ipsilateral hemisphere [6]. The same authors reported a 9-year-old female with inactive ECDS on a methotrexate wean who had right-side parietal hemorrhage with MRI imaging also consistent with ipsilateral cavernomas [6]. An 18-month-old boy with ECDS was reported to have multiple cavernomas and a subacute occipital hemorrhagic change on MRI during workup. He did not have correlating neurological symptoms of ECDS. At age 4, he presented with generalized seizures and the occipital intraparenchymal lesion was found to have increased in size [7].
In the ECDS case that we describe, multiple imaging modalities, including endovascular selective catheterization and angiography, failed to identify a vascular lesion to correlate with the hemorrhage. We believe that this represents a novel presentation of ECDS in a pediatric patient. A weakness of this case is the lack of records on the patient's diagnostic testing and treatment performed outside the United States. While imaging performed at our center did not show cavernomas or other vascular malformations, there were no prior scans available for comparison. A potential confounder is that up to 50% of cavernomas in Hispanic patients can be attributed to inherited familial disease, compared to 20% in the general population [8]. It is possible that a solitary cavernoma developed in this patient independently of ECDS, or in correlation with ECDS. However, progression of ECDS in this manner would also be highly unusual, as previous reports found multiple cavernomas ipsilateral to the hemorrhage on imaging.
In conclusion, our case of intraparenchymal hemorrhage in ECDS without a correlating vascular lesion is highly unusual and the first reported in the literature to our knowledge. This report adds to the body of knowledge of the neurological phenomenon of ECDS. It also highlights the importance of effective collaboration between pediatric neurosurgery, rheumatology, and neuroradiology to identify ECDS patients at risk for cerebral hemorrhage. In our case, the hemorrhage presented before the diagnosis of ECDS was made, and endovascular procedures done by neurosurgery contributed to the workup.
The authors thank the patient and their family for participation in the expansion of medical knowledge.
The authors have no personal, financial, or institutional interest in any of the drugs, materials, or devices described in this article.
Draft manuscript preparation: Benjamin Ramsey, BS.
Image selection: Chelsea Reynolds, DO.
Conception for case report: Catherine McClung Smith, MD.
All authors reviewed the manuscript and approved it for submission.