Background: Hirayama disease is a rare disorder seen in young patients in their second or third decade of life with slowly progressive self-limiting distal upper limb muscle weakness with seldom symmetrical involvement. It is a peculiar anterior horn cell disease that is managed conservatively with limited surgical options available as per literature.
Case description: Our patient was a twenty-one-year-old male who developed insidious onset, non-progressive asymmetrical weakness in both hands (right > left) with wasting of all intrinsic muscles. After electromyography and MRI confirmed the diagnosis of Hirayama disease, he was managed conservatively with a cervical collar and there was a significant improvement in symptoms.
Conclusion: Hirayama disease being a benign and self-limiting disorder requires early diagnosis following which conservative management using a cervical collar can aid in the early control of the progress of disease which is usually seen in the first few years of onset.
Hirayama disease, Intrinsic muscles of the hand, Cervical collar
Hirayama disease, first reported by Hirayama et al. in 1959, is a rare disorder usually seen in Asian males in the second or third decade of their life, with asymmetrical involvement of distal upper limb causing weakness and atrophy with insidious onset and self-limiting benign course [1-3]. An abnormal compression or flattening of the anterior cord against the vertebral bodies during neck flexion, causing compression of the cervical cord, and resulting in atrophic and ischaemic changes in the anterior horn is considered to be the principal causative mechanism [4]. Conservative management with cervical collars and physiotherapy is usually sufficient to relieve symptoms in early disease but in advanced and severe cases surgical intervention is found to be useful [5-9].
A twenty-one-year-old male right-handed came to us with a chief complaint of weakness in the grip of both hands (right > left) which was noticed by him in August 2020 when he was gathering clay with his bare hands to make a Ganesha idol. He experienced that this weakness was static and non-progressive and was not related to any aggravating or relieving factors. The patient also had a history of occasional tingling in both of his hands since childhood which was left unattended. The patient started noticing the loss of the bulk of his bilateral hand muscles. The patient did not have weakness in proximal upper limbs or any of the lower limbs. He did not have any complaints regarding bowel and bladder habits. On examination, we found wasting of thenar as well as hypothenar muscles (Figure 1 and Figure 2). The patient had asymmetric weakness in all his intrinsic muscles (3/5) of both hands. All the sensations were well preserved and deep tendon reflexes were normal. The nerve conduction studies, and EMG findings were suggestive of bilateral C8-T1>>C7>>C5-C6 very chronic motor axon degeneration with the site of involvement likely to be at anterior horn cell or cord level. His MRI of the cervical spine (Figure 3, Figure 4 and Figure 5) was showing focal atrophy of the lower cervical spinal cord from C5-C6 to C6-C7 disc levels with mild prominence of the central canal and on flexion, there was the ventral movement of posterior dura with the prominence of the posterior epidural venous plexi extending from C3 to upper dorsal levels. All these findings were suggestive of Hirayama disease. The patient was advised to wear a cervical collar and on follow up after two months he had relief from his tingling and there was an improvement in power (4/5) of intrinsic muscles of both hands. He was able to write in reasonably good handwriting and was able to perform all his routine activities without any disturbances.
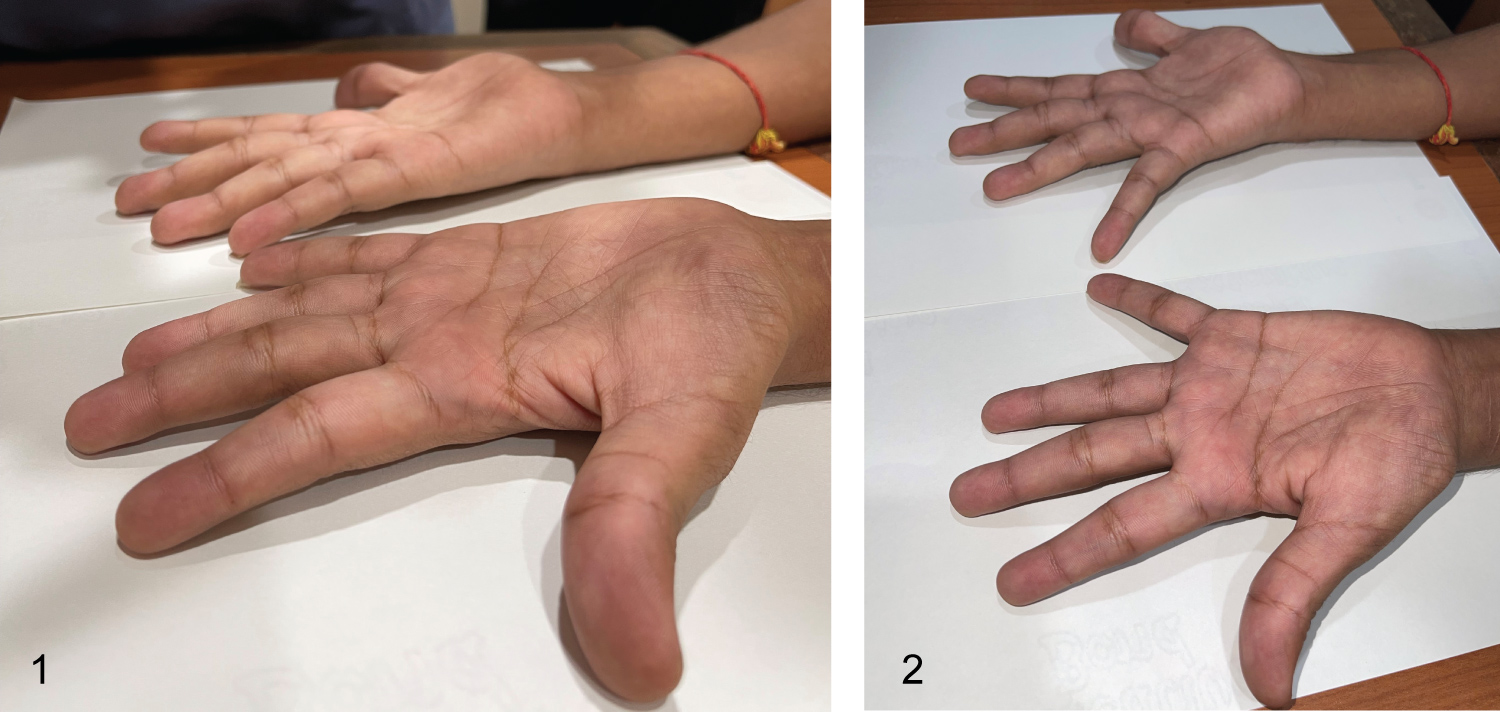 Figure 1 and Figure 2: Clinical picture showing wasting of intrinsic muscles of both hands.
View Figure 1&2
Figure 1 and Figure 2: Clinical picture showing wasting of intrinsic muscles of both hands.
View Figure 1&2
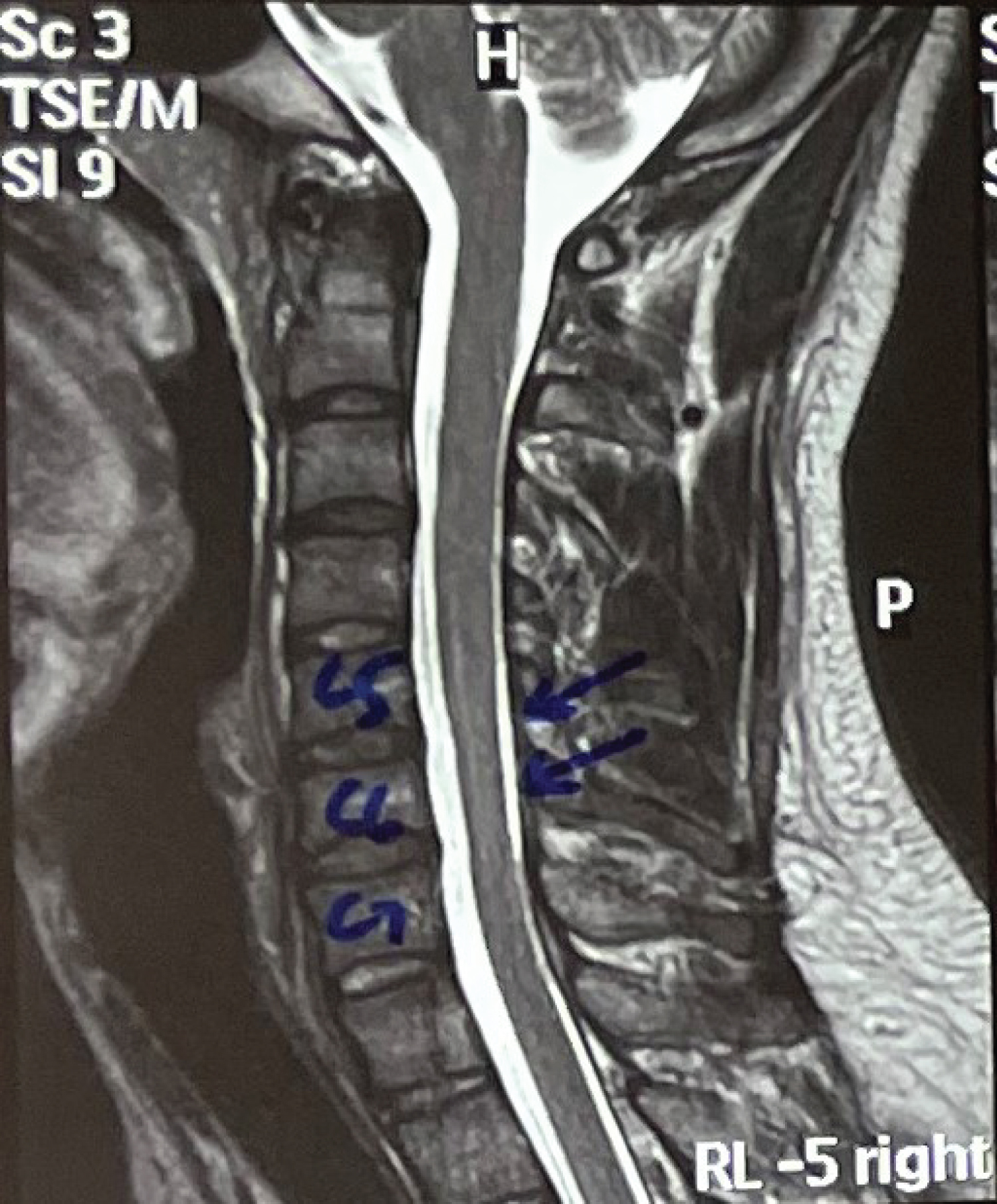 Figure 3: Sagittal T2 image in neutral position showing cord atrophy at C5, C6, C7 level with mild prominence of the central canal.
View Figure 3
Figure 3: Sagittal T2 image in neutral position showing cord atrophy at C5, C6, C7 level with mild prominence of the central canal.
View Figure 3
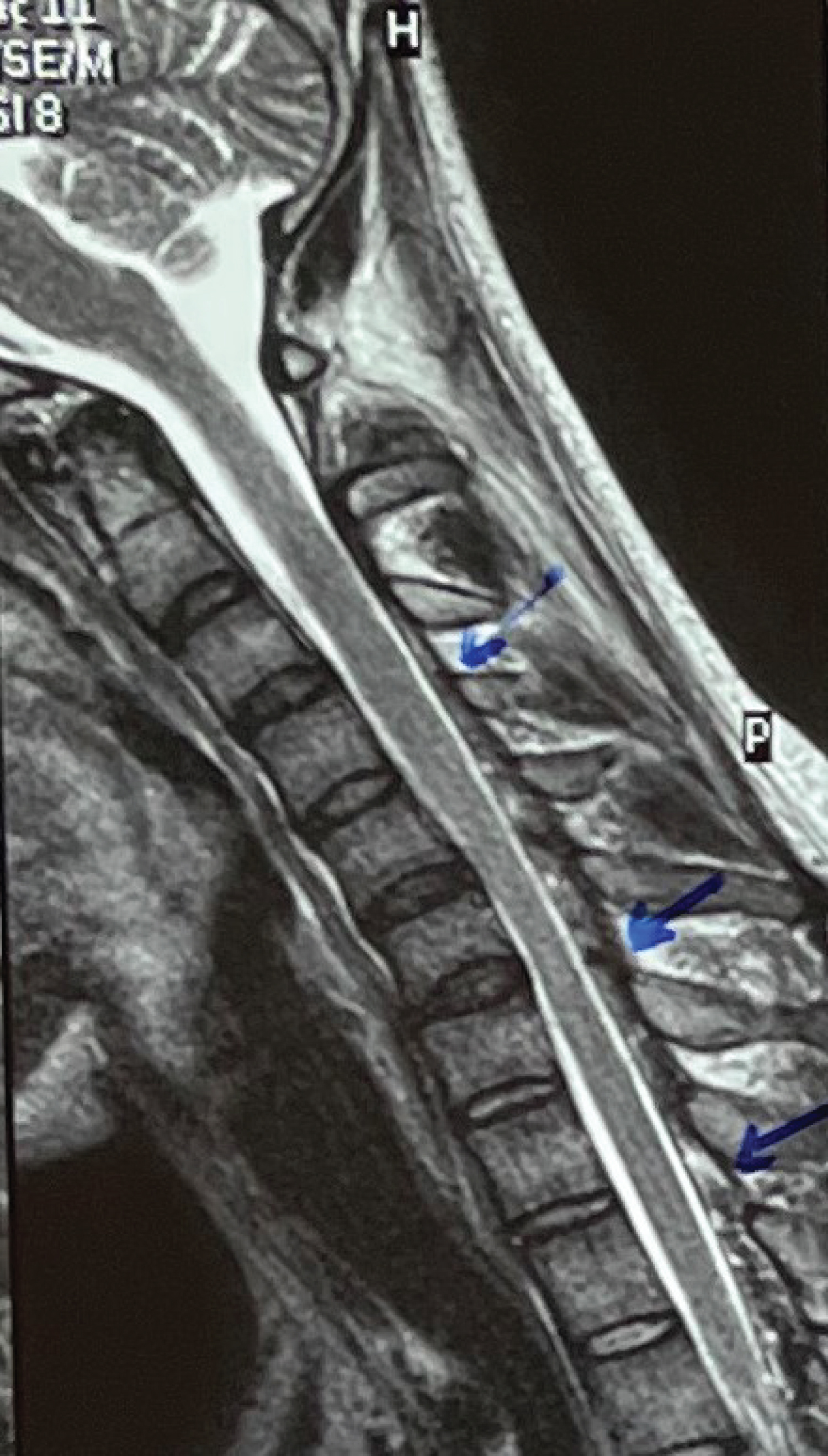 Figure 4: Sagittal T2 image after neck flexion showing the ventral movement of the posterior dura with the prominence of the posterior epidural venous plexi extending from C3 to upper dorsal levels (Shown with blue arrows).
View Figure 4
Figure 4: Sagittal T2 image after neck flexion showing the ventral movement of the posterior dura with the prominence of the posterior epidural venous plexi extending from C3 to upper dorsal levels (Shown with blue arrows).
View Figure 4
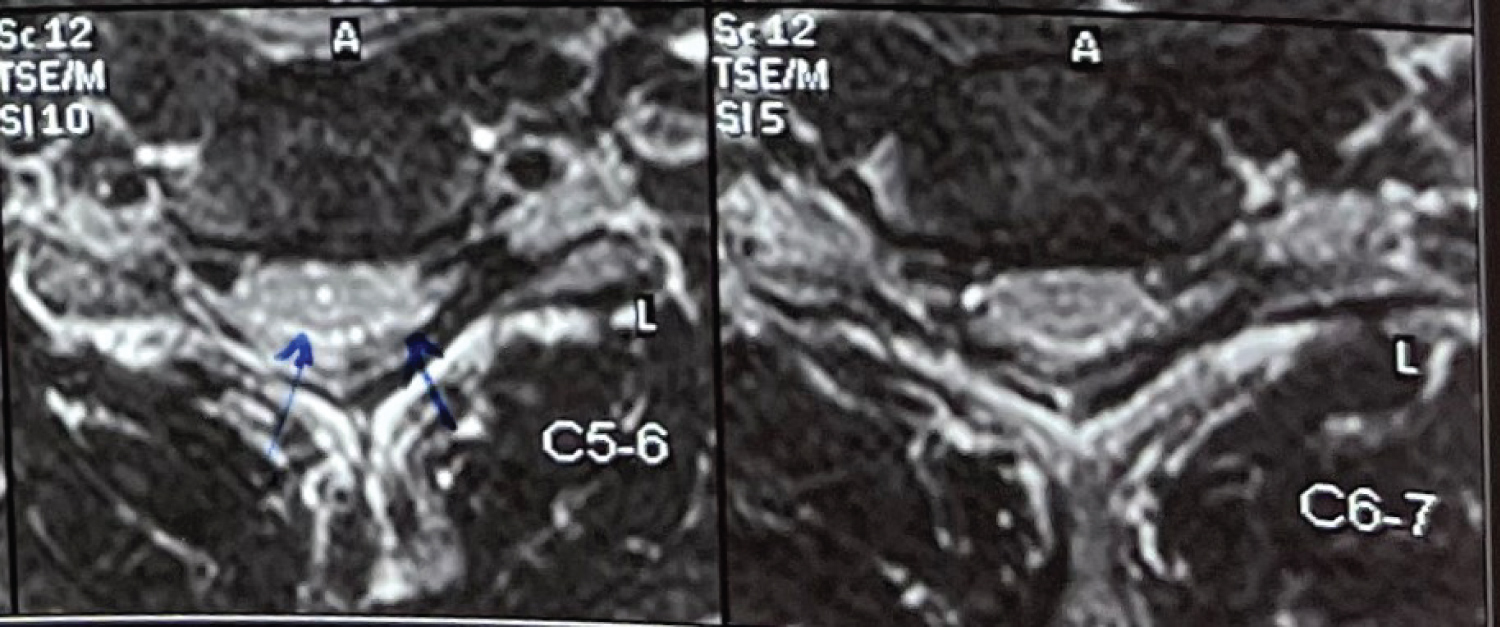 Figure 5: Axial T2 images showing asymmetric cord atrophy and hyperintense signal in the anterior horn cell region.
View Figure 5
Figure 5: Axial T2 images showing asymmetric cord atrophy and hyperintense signal in the anterior horn cell region.
View Figure 5
Hirayama disease is characterized by asymmetrical distal upper limb weakness and atrophy with insidious onset, usually self-limiting nature with patients typically being Asian males in their second decade of life [1-3]. As far as the pathophysiology is concerned it is believed that a malfunction of the anterior horn cell at the cervical level is the reason for the signs and symptoms [10]. This malfunction could be the result of circulatory changes in the lower cervical cord, which causes ischemic changes in the anterior horn due to congestion of the venous plexus, abnormal drainage in the vertebral venous plexus, or malformation of the epidural vessels and these changes are thought to be due to spinal cord compression and cervical the cal sac compressive flattening during cervical flexion [11,12]. Hirayama disease has characteristic clinical features that include progressive muscular weakness of one or both hands and forearms without compromise of brachioradialis muscles and for this reason, it is also called oblique amyotrophy [13]. MRI in the routine supine position and mandatory flexion MRI shows atrophy of the lower cervical cord which could be asymmetric corresponding to the more atrophied side [14]. Flexion MRI shows anterior displacement of the posterior dura with an enlarged epidural space seen as a crescent high T1 and T2 intensity posteriorly on axial images containing flow voids and prominent enhancement on postcontrast images within these spaces which correspond to enlarged posterior veins. The electromyography results in Hirayama disease show denervation of atrophied muscles with occasional contra-lateral denervation of the same muscles, along with evidence of denervation in triceps brachii and less than a quarter of patients in biceps brachii, deltoid, and brachioradialis, even though there is no clinically visible wasting [11,15]. Application of a cervical collar to minimize neck flexion can achieve satisfactory results for some patients [16]. However, for patients with advanced disease and severe deficits and for patients whose condition continues to progress despite conservative treatment or patients who are not compliant with a cervical collar, surgical intervention could be helpful to provide stability by fixation [17]. Our patient was treated with a cervical collar following which he showed improvement in his symptoms and was more comfortable and confident in doing all his daily routine activities.
Hirayama disease being a benign and self-limiting disorder requires early diagnosis following which conservative management using a cervical collar can aid in the early control of the progress of the disease which is usually seen in the first few years of onset.