Background: Pilocytic astrocytoma (PA) is classified as a benign tumor, which is rarely reported in adults. We present two case reports of adult PAs (APAs) and a literature review.
Case descriptions: In Case 1, a 25-year-old man presented with progressive right parieto-temporal head puffing. Head computed tomography (CT) revealed multiple large cystic tumors with a midline shift. Gross total removal (GTR) was performed. No recurrence was observed in 3 months. In Case 2, a 38-year-old man presented with cerebellar symptoms. His head CT and brain magnetic resonance imaging revealed a cystic tumor in the cerebellar region. Surgical GTR was performed. No recurrence was observed in 3 months. An examination of previous reports of supratentorial or cerebellar APAs in the PubMed database suggested recurrence only in subtotal rection cases.
Discussion: GTR or radiation therapy, if GTR is not achieved, is the most important factor for minimizing recurrence after removing the tumor.
Pilocytic astrocytoma, Adult, Brain
Pilocytic astrocytomas (PAs) are classified as grade l brain tumors by the World Health Organization. PAs account for approximately 25% of pediatric brain tumors and 1.5% of adult brain tumors [1]. As diagnosing PAs during adulthood is rare, there are few reports in the literature. Here, we present two case reports of adult PAs (APAs) and a literature review that examined the clinical presentation, extent of resection, and outcomes of APAs.
A 25-year-old man with intellectual disabilities and left-sided hemiparesis presented to our department with progressive right parieto-temporal head puffing. On examination, he also showed communication disability and left hemi-spatial neglect. Head computed tomography (CT) and brain magnetic resonance imaging (MRI) revealed multiple cystic solid tumors in the right temporal, parietal, and occipital regions with a midline shift (Figure 1A and Figure 1B). A carotid angiogram of the right side revealed multiple arterial feedings from the right middle cerebral artery, right tentorial artery, and branches of the middle meningeal artery (Figure 1C, Figure 1D and Figure 1E). Neuronavigation-guided gross total resection (GTR) was performed (Figure 1F, Figure 1G and Figure 1H). Histopathological examination revealed an APA with varying proportions of compacted bipolar cells and loose microcystic areas (Figure 2A, Figure 2B and Figure 2C). We observed numerous eosinophilic granular bodies and rare mitotic figures. The tumor cells were positive for GFAP (Figure 2D) and negative for CD34, p53, and IDH-1. ATRX was absent in the tumor cell nuclei. The Ki-67 index was approximately 1%, and the modified Rankin Scale (mRS) score was comparable before and after the operation.
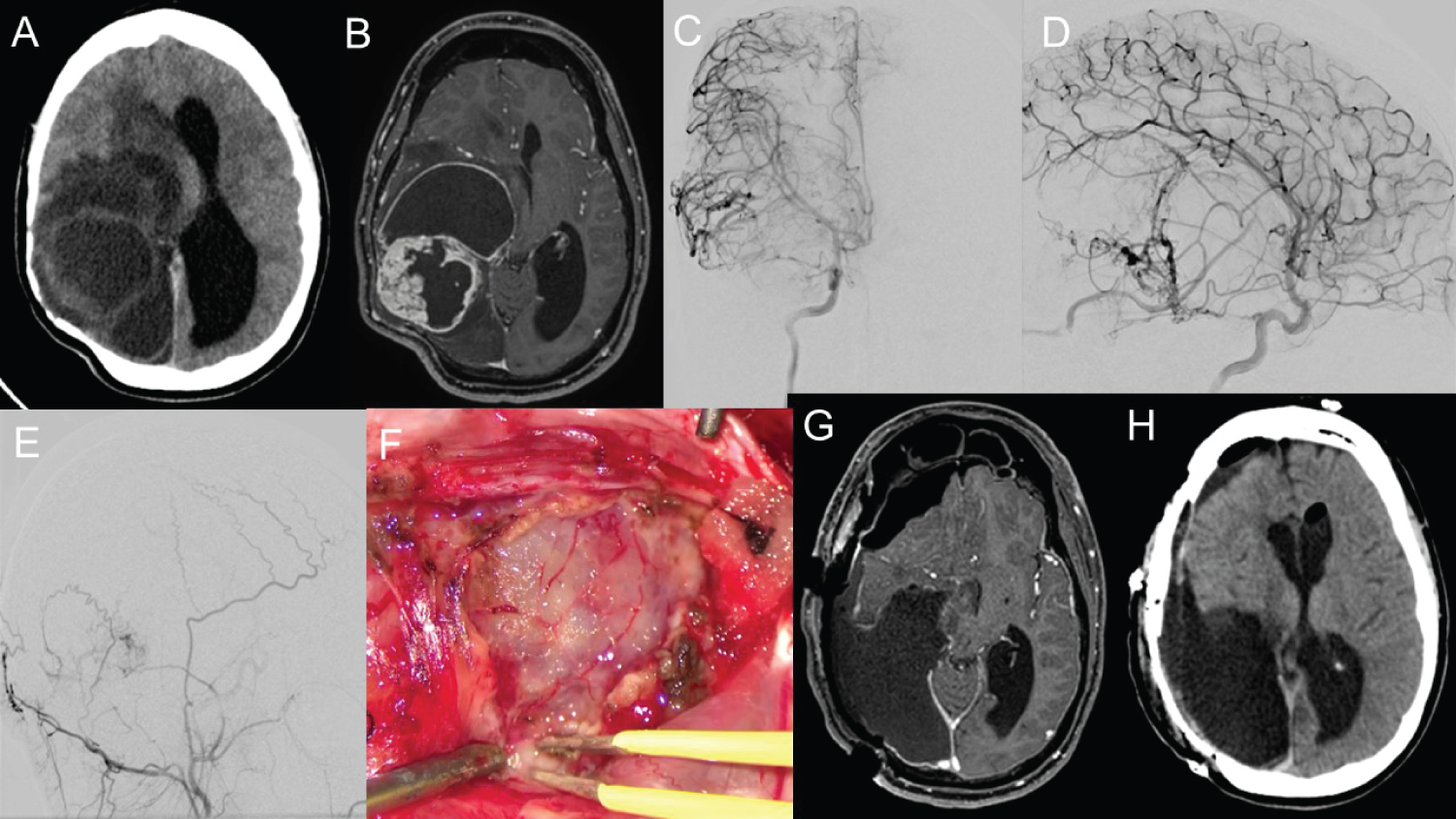 Figure 1: Images and intraoperative findings of Case 1.
Figure 1: Images and intraoperative findings of Case 1.
Initial head computed tomography (CT) (A) and brain magnetic resonance imaging (MRI) (B) show multiple cystic solid tumors in the right temporal, parietal, and occipital regions with midline shift. A carotid angiogram of the right side (C: Anterior-posterior view, D: Lateral view) reveals multiple arterial feedings from the right middle cerebral artery and right tentorial artery. The right external carotid angiogram (E) shows tumoral feeding from the branches of the middle meningeal artery. Intraoperative findings show a thick, vascular-rich tumor wall and cyst (F). Neuronavigation-guided surgical gross total resection postoperative images (G: MRI; H: Head CT).
View Figure 1
 Figure 2: Pathological findings of Case 1.
Figure 2: Pathological findings of Case 1.
Histopathological examination in Case 1 revealed a pilocytic astrocytoma with varying proportions of microcystic areas (A), compacted bipolar cells, and loose microcystic areas (B). There are numerous eosinophilic granular bodies and rare mitotic figures (C). The tumor cells are positive for GFAP (D).
View Figure 2
A 38-year-old man presented with ataxia, vertigo, and vomiting in our department. His head CT and brain MRI revealed multiple cystic solid tumors in the cerebellar region (Figure 3A and Figure 3B). An angiogram of the right vertebral artery revealed no apparent feeding arteries (Figure 3C). Surgical GTR was performed (Figure 3D), and a histopathological examination revealed a PA with varying proportions of compacted bipolar cells and loose microcystic areas. We observed numerous eosinophilic granular bodies (Figure 3E) and rare mitotic figures. The tumor cells were positive for GFAP (Figure 3F) and negative for CD34, p53, and IDH-1. ATRX was absent in the tumor cell nuclei. The Ki-67 index was approximately 1%, and the mRS score was comparable before and after the operation. No recurrence was observed for 10 years after tumor removal.
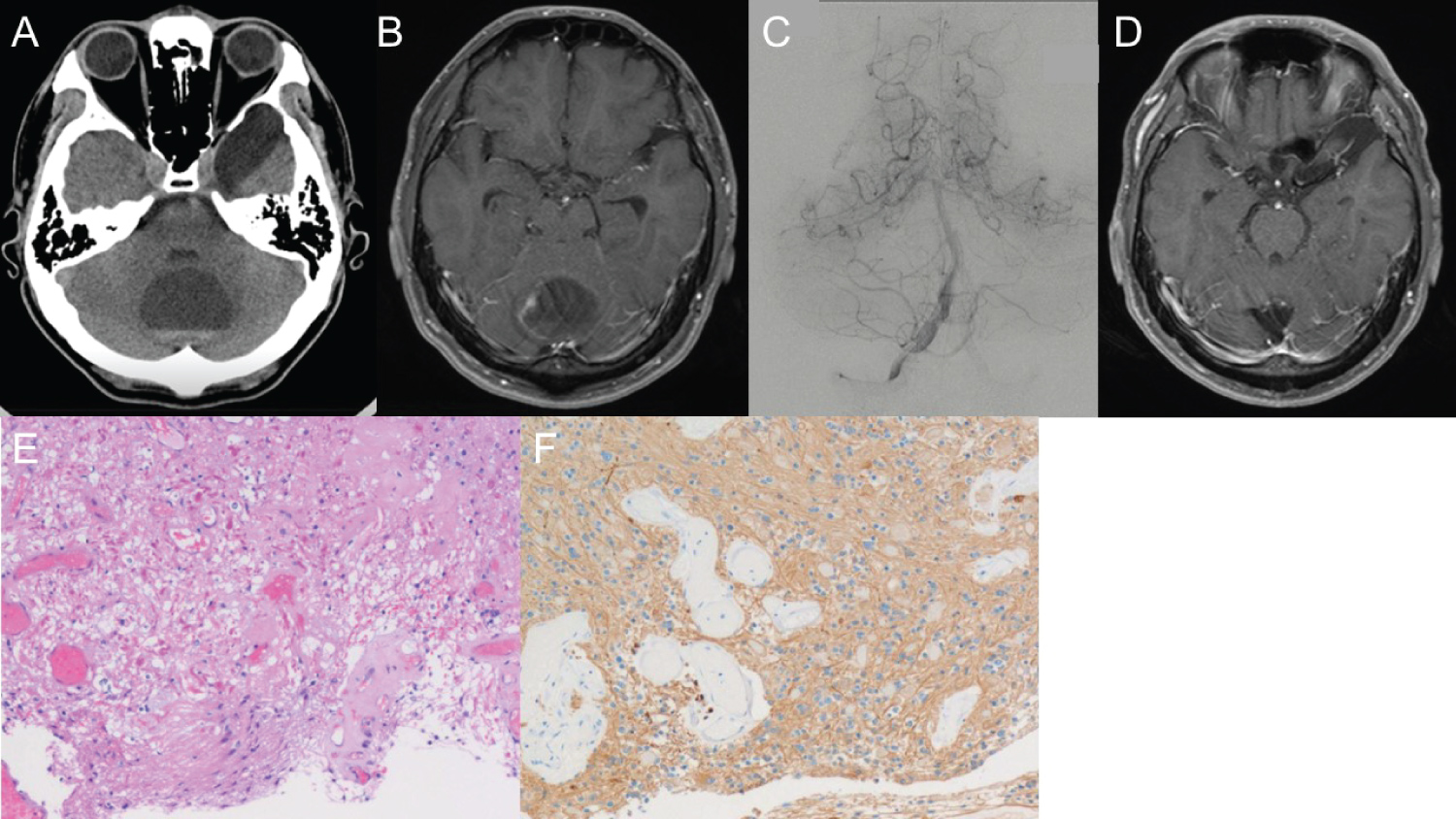 Figure 3: Images and pathological findings of Case 2.
Figure 3: Images and pathological findings of Case 2.
Head computed tomography (CT) (A) and brain magnetic resonance imaging (MRI) (B) in Case 2 revealed multiple cystic solid tumors in the cerebellar region. An angiogram of the right vertebral artery revealed no apparent feeding arteries (C). Surgical gross total resection was confirmed in postoperative MRI (D), and a histopathological examination revealed a pilocytic astrocytoma with varying proportions of compacted bipolar cells and loose microcystic areas. Numerous eosinophilic granular bodies (E) and rare mitotic figures are present. The tumor cells are positive for GFAP (F).
View Figure 3
We examined previous reviews or case reports of supratentorial or cerebellar APAs in the PubMed database. Fourteen articles were collected [1-13], including our own (Table 1 and Table 2). Thirty-five supratentorial and thirty-three cerebellar APAs have been reported. Of the supratentorial APA patients, 51% were male, the average age was 32 years (range 18-76 years), and 12% of cases were asymptomatic. The recurrence rate was 15%, and all were subtotal rection (STR) cases. Of the cerebellar APA patients, 57% were male, the average age was 36 years (range 18-83 years), and 26% of cases were asymptomatic. The recurrence rate was 12%, and all cases were STR.
Table 1: Supratentorial adult pilocytic astrocytoma case series. View Table 1
Table 2: Cerebellar adult pilocytic astrocytoma case series. View Table 2
Yang, et al. established a cohort study that included 3014 (69.2%) pediatric and 1343 (30.8%) adult PA patients using the Surveillance, Epidemiology, and End Results Program database [1]. In this study, 43.5% of pediatric tumors were in the cerebellar region compared to 35.3% in adult patients. Patients with APA tend to have more frontal, temporal, parietal, occipital, and ventricular or paraventricular tumors compared to pediatric patients with PA. The distribution of tumor location could be related to the age of pediatric patients. In contrast, in adults, the tumor location is primarily supratentorial. We detected a similar trend in our review. APAs usually manifest with a space-occupying lesion affecting both the supratentorial and the posterior fossa. As the mass affects or obstructs the hydrocephalus, the clinical symptoms are headache, vomiting, nausea, and papilledema [1]. In some cases, including the two cases we described here, a preoperative diagnosis is challenging as gadolinium-based MRI shows only large tumoral lesions, and enhanced cystic lesions.
Johnson, et al. reviewed APA outcomes in 865 patients older than 19 years and found that GTR was a significant predictor of survival compared with STR or biopsy analysis [14]. Surgical excision of the tumor is the treatment of choice, aiming at tumor-free margins and minimal neurological insults. Recurring tumors are often removed by additional surgical resection [14,15]. In both cases described here, the tumors were rich in vascular vessels and relatively large. The removal of tumors requires a prolonged operative time and blood transfusion to perform GTR, making tumor removal difficult. However, GTR is necessary to prevent the recurrence of this pathologically benign tumor.
Here, we report two rare cases of APAs and review previous reports of APAs. GTR or radiation therapy, if GTR is not achieved, is the most important factor for minimizing recurrence after the removal of the tumor despite its pathologically benign characteristics.
Our institution does not require ethical approval for reporting individual cases or case series.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
All authors contributed to the submitted manuscript.