Background: Anterior lumbar interbody fusion (ALIF) has become widely accepted for the treatment of discogenic low back pain, achieving similar radiological and clinical treatments to other techniques. To describe sigma perforation and septic peritonitis as a potentially fatal complication after an anterior interbody fusion.
Case report: A 63-year-old women consulted to the emergency room for diffuse abdominal pain and nausea after a L5-S1 ALIF 5 days prior. Blood tests and X-Rays showed no alterations. A CT scan showed intraabdominal liquid and a pneumoperitoneum, later evolving to septic shock. An emergent laparotomy was performed to repair a 1 cm-long perforation of the minor sigma. One year later, patient was with no pain neither X-ray alteration.
Conclusion: Potential complications of an anterior lumbar approach include iliac vein injury, thrombosis, or retrograde ejaculation. However, bowel injuries are uncommon, and a case of septic peritonitis after a sigma perforation, with high morbidity, has never been described before.
Anterior lumbar, Sigma, Perforation, Septic, Peritonitis
The gold-standard surgical treatment for low back pain due to degenerative disk disease (DDD) is the fusion of the affected level [1]. Although Posterior fusion techniques such as transforaminal or posterior lumbar interbody fusion (TLIF and PLIF) are performed more often worldwide, anterior lumbar interbody fusion (ALIF) techniques are also common, and have been described to achieve comparable clinical and radiological results [2]. Recent literature states that ALIF surgeries might be superior to posterior fusions when it comes to better restoration of the lumbar lordosis or lower rates of dural tear. Also, many authors claim that patients who undergo anterior lumbar fusion have a better postoperative recovery when compared to posterior lumbar fusion, mainly due to the sparing of the posterior lumbar musculature [3-6].
However, the anterior lumbar approach is not without risk. It involves dissection of structures as the peritoneum, ureters, and iliac vessels [7]. Uncareful dissection or misplacement of retractors can lead to the injury of one of these structures, with an important associated morbidity. Knowledge of the anatomy and careful blunt dissection are paramount in order to prevent unwanted damage. We present a case of a patient who underwent an ALIF with an A2L (Eurospine®) cage and suffered an injury to the sigma. We carried out a literature review and found that this has not yet been reported. This case highlights the importance of knowing and preserving the anatomic landmarks in the anterior lumbar approach.
A 63-year-old woman consulted to the emergency room for abdominal pain and nausea. She had undergone an L5-S1 ALIF surgery via an anterior lumbar approach 5 days prior in another hospital. Blood tests showed no alterations and Plain X-Rays showed feces in the descending colon, without loosening of the implant. A CT scan was performed, which showed abundant intraabdominal liquid and a pneumoperitoneum (Figure 1 and Figure 2).
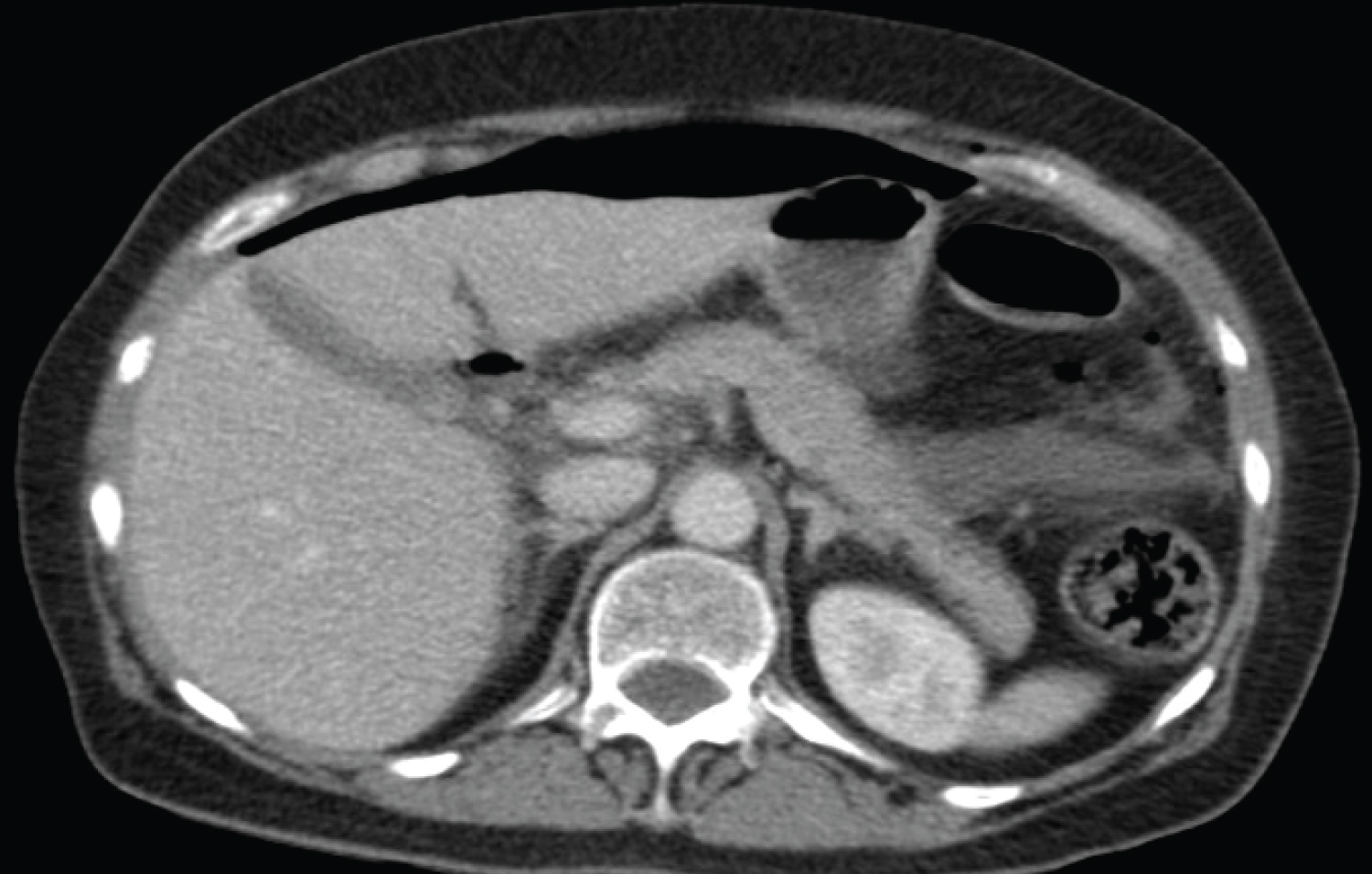 Figure 1: Preoperative abdominal CT scan with diffuse pneumoperitoneum.
View Figure 1
Figure 1: Preoperative abdominal CT scan with diffuse pneumoperitoneum.
View Figure 1
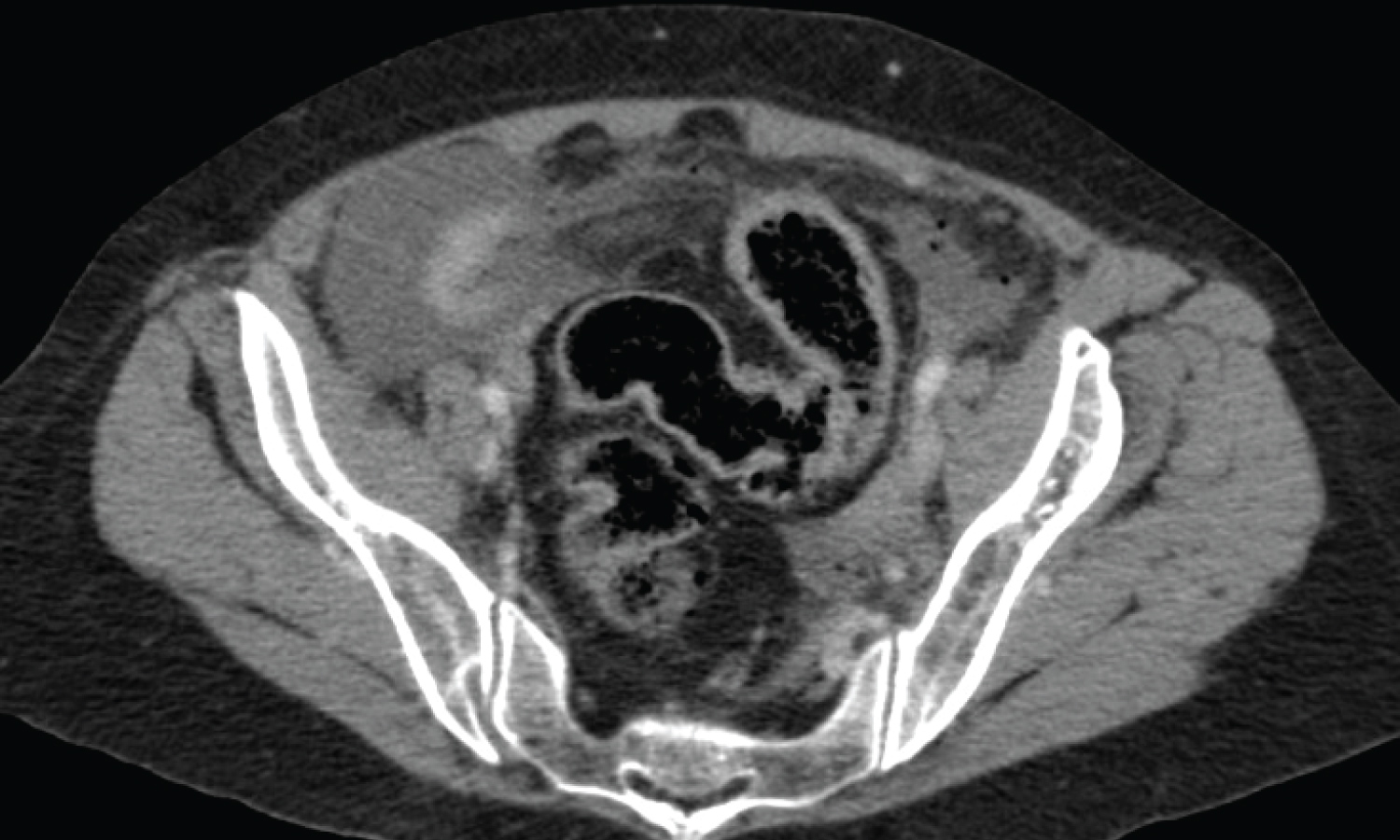 Figure 2: Preoperative abdominal CT scan with free liquid inside the pelvis as well as oedema and pneumatosis in the walls of the sigma.
View Figure 2
Figure 2: Preoperative abdominal CT scan with free liquid inside the pelvis as well as oedema and pneumatosis in the walls of the sigma.
View Figure 2
The patient evolved to septic shock state, and so an emergent laparotomy was performed, showing a fecaloid peritonitis with a 1 cm-long perforation of the minor sigma, which was successfully repaired. There was no retroperitoneal extension, so the ALIF cage was not compromised. After the surgery, intravenous antibiotics were initiated.
Initially, she was transferred to the intensive care unit and, since the evolution was satisfactory, she was transferred to hospitalization. There, she presented an infection of the wound, so in addition to the antibiotics, she was treated by negative-pressure therapy with resolution of the infection.
One year later, although lumbar X-Rays show a partial loosening of the ALIF cage, she is without abdominal or lumbar pain upon gait. The surgical wound has a good macroscopical aspect and control CT scan shows no intraabdominal collections (Figure 3).
 Figure 3: Control CT scan. There are no intraabdominal collections, and the ALIF cage shows a partial loosening.
View Figure 3
Figure 3: Control CT scan. There are no intraabdominal collections, and the ALIF cage shows a partial loosening.
View Figure 3
When surgically treating DDD, ALIF has become increasingly popular and is widely performed nowadays [3,8]. It has proven to have advantages over posterior techniques, such as better restoration of disk height or lower rates of dural injury [2,9]. However, the anterior approach is not without its risks, since it jeopardizes abdominal structures such as bowels, the ureters, and the iliac vessels. Moreover, it has a long learning curve.
In this case, it is unclear when the perforation of the sigma took place, but there are two critical moments during a retroperitoneal anterior lumbar approach when the bowels are at high risk of being injured. These moments would be during the dissection of these structures and during the placement of the retractors prior to the diskectomy. Specifically, retractor placement must be performed with care not to damage the iliac vessels and avoiding excessive retraction of the bowels or the ureters [3,5,7,9,10]. One way to avoid these complications is with the help of an access surgeon such as a vascular or a general surgeon, who would be more familiarized with abdominal dissection.
Bowel injuries are relatively uncommon during anterior lumbar approaches. They are estimated to take place in less than 0.5% of all cases [11]. However, they pose a serious complication, and can easily go unnoticed during the surgery, leading to a late diagnosis and high morbidity and mortality [12]. In this case, the sigma lesion was not noticed and repaired during the ALIF surgery, and that was the trigger for the peritonitis and septic shock that occurred later.
Mahoney, et al. [13] described a case of a 72-year-old male who, 5 days after an ALIF surgery, developed an acute colonic pseudo-obstruction which later led to a colonic perforation that had to be surgically repaired. In this case however, the colonic injury did not take place during the surgery. Bianchi, et al. [14] reviewed 72 patients who underwent lumbar surgery via an anterior lumbar approach. They described one case of small bowel perforation, although the follow-up of that case is not documented.
What stands out about this case is not only the perforation of the sigma, which has never been described before during an anterior lumbar approach, but the peritonitis and septic shock which derived from it. Peritonitis after gastrointestinal tract perforation is a severe complication with mortality rates ranging between 17 and 63% [15]. In this case, both in the CT scan and during the laparotomy, we could observe that the ALIF material was not compromised by the peritonitis, since the sigma is a peritoneal structure whereas the lumbar spine is retroperitoneal. For that, after the surgical debridement had been performed, the cage could be preserved. It is clear however that, when performing an anterior lumbar approach, careful and blunt dissection of the structures lying superficial to the spine is paramount to avoid iatrogenic lesions which could have fatal consequences.
Although ALIF techniques are increasingly popular, the anterior lumbar approach is a challenging approach with a long learning curve. It poses danger to the abdominal structures, and iatrogenic bowel injuries may cause high morbidity and mortality so careful blunt dissection is vital to avoid damaging them.