Objective: Trigeminal neuralgia, hemifacial spasm, and glossopharyngeal neuralgia are defined as neurovascular syndromes and are conditions of compression of the cranial nerves by vascular structures. The aim of this study is to make the surgical approach safer by providing aggregate data on vascular structures and their aspects that cause compression in neurovascular syndromes.
Methods: We performed a retrospective analysis of 338 cases who had MVD surgery between the years 2009-2019 in our center. In this study we determine the position and anatomy of the neurovascular conflict and try to classify the vascular relation with the nerve according to operative anatomy.
Results: SCA is the most common artery compressing the trigeminal nerve mostly superior, whereas AICA most commonly compress the facial nerve from the inferior of the nerve. PICA is the most common artery compressing the inferior cranial nerves from superior. We identified most of SCA compression from superior, most of AICA from inferior. We observed that compression of the inferior cranial nerves was caused by PICA, VA, and BA.
Conclusions: To know the most common neurovascular compression patterns in neurovascular syndromes provide confidence and improve success in MVD surgery.
Trigeminal neuralgia, Hemifacial spasm, Glossopharyngeal neuralgia, Vascular compression, Arteries, Vessels
AICA: Anterior Inferior Cerebellar Artery; GPN: Glossopharyngeal Neuralgia; HFS: Hemifacial Spasm; MVD: Microvascular Decompression; NVSC: Neurovascular Syndromes; PICA: Posterior Inferior Cerebellar Artery; REZ: Root Entrance Zone; SCA: Superior Cerebellar Artery; TN: Trigeminal Neuralgia
Trigeminal neuralgia (TN), Hemifacial spasm (HFS), Glossopharyngeal neuralgia (GPN), and Geniculate neuralgia are neurovascular syndromes (NVSC) characterized by the compression of cranial nerves by vascular structures. The cranial nerves are surrounded by a myelin sheath, which is necessary for axonal conduction. NVSC mostly originates in the transition zone or root entrance zone (REZ), which is used to define the portion of the nerve that includes the central and peripheral myelin.
Despite its unclear pathophysiology, NVSC is caused by compressions of the main arteries: the superior cerebellar artery (SCA) in TN, the anterior inferior cerebellar artery (AICA) in HFS, and the posterior inferior cerebellar artery (PICA) in GPN. Moreover, very few studies to date have evaluated the anatomical relationship of the arterial compression and the affected nerve.
This study was aimed at anatomically evaluating these compressions and classifying the types of compression of the nerve by the artery, in order to develop a more effective and reliable surgical treatment.
We retrospectively reviewed 338 patients who underwent microvascular decompression (MVD) surgery between 2009 and 2019 in our center. Those suffering from NVCS were preoperatively examined by magnetic resonance imaging including TOF and CISS.
Suboccipital retrosigmoid approach was performed by the deceased senior author of the present study, as described in the literature [1,2]. Briefly after a lateral suboccipital craniotomy, cerebrospinal fluid was drained from the cerebellopontine cistern. The cerebellum was dynamically and intermittently retracted using a piece of cotton sponge placed along the petrosal surface of the simple lobule. This allowed reach toward the lateral cerebellopontine cistern without using brain retractors. A targeted microsurgical dissection of the entire affected nerve was performed to determine the offending vessel. A 360° dissection of the nerve is meticulous, as any other vascular compression or arachnoid tethering of the nerve must not be overlooked. In our studys' most cases, decompression was performed with the interposition of the offending artery by small pieces of Teflon.
Of the 338 patients with NSVC, 162 (47.9%) had arterial compression, 83 (24.5%) had vein compression, and 52 (15.3%) had both compressions, while 8 (2.3%) did not have any pressure and 3 (9.7%) had thick arachnoid membrane (Table 1). Of the 201 (59.4%) had compression on the CN V -CN VII-CN VIII patients, 151 (75.1%) were able to preserve their petrous veins during surgery. Of all the patients a piece of Teflon was placed in 162 (47.9%) patients. Of the patient that we operated on, 161 (48.3%) patients had compression on the cranial nerve (CN) V, 41 (12.2%) had compression on the CN VII-CN VIII, and 2 (0.5%) had compression on the CN XI.
Table 1: Nerve compression. View Table 1
Arterial compression was noted in 195 patients: SCA compression (114/175) (Figure 1), AICA compression (39/175) (Figure 2), vertebral artery (VA) compression (19/175), PICA compression (n = 2/175) (Figure 3), and basilar artery (BA) compression (n = 1/175).
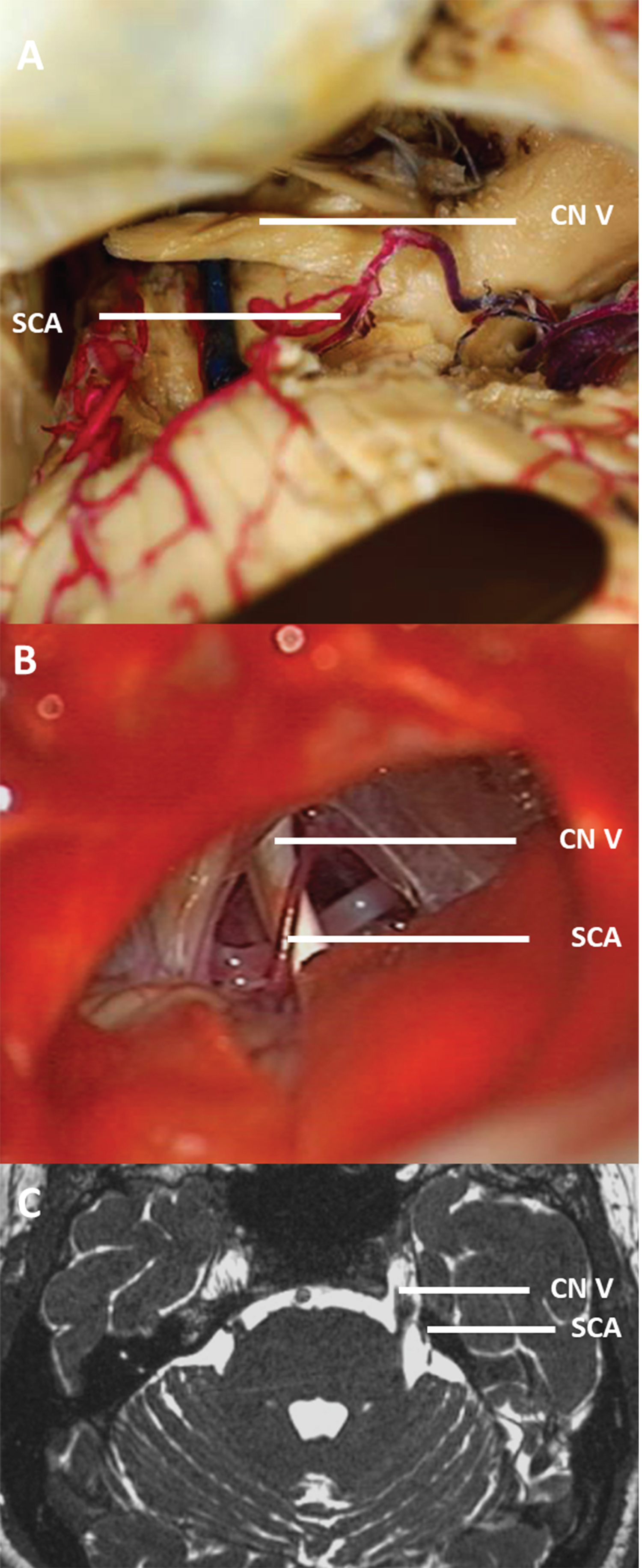 Figure 1: SCA is the most common artery compressing the trigeminal nerve (A) Anatomical relationship between CN V and SCA is shown in the cadaver dissection images; (B) SCA compression from the superior part of the nerve is visible in the intraoperative image; (C) Preoperative CN V and SCA compression image in axial T2 MRI sequence is shown.
Figure 1: SCA is the most common artery compressing the trigeminal nerve (A) Anatomical relationship between CN V and SCA is shown in the cadaver dissection images; (B) SCA compression from the superior part of the nerve is visible in the intraoperative image; (C) Preoperative CN V and SCA compression image in axial T2 MRI sequence is shown.
SCA: Superior Cerebellar Artery; CN: Cranial Nerve; MRI: Magnetic Resonance Imaging
View Figure 1
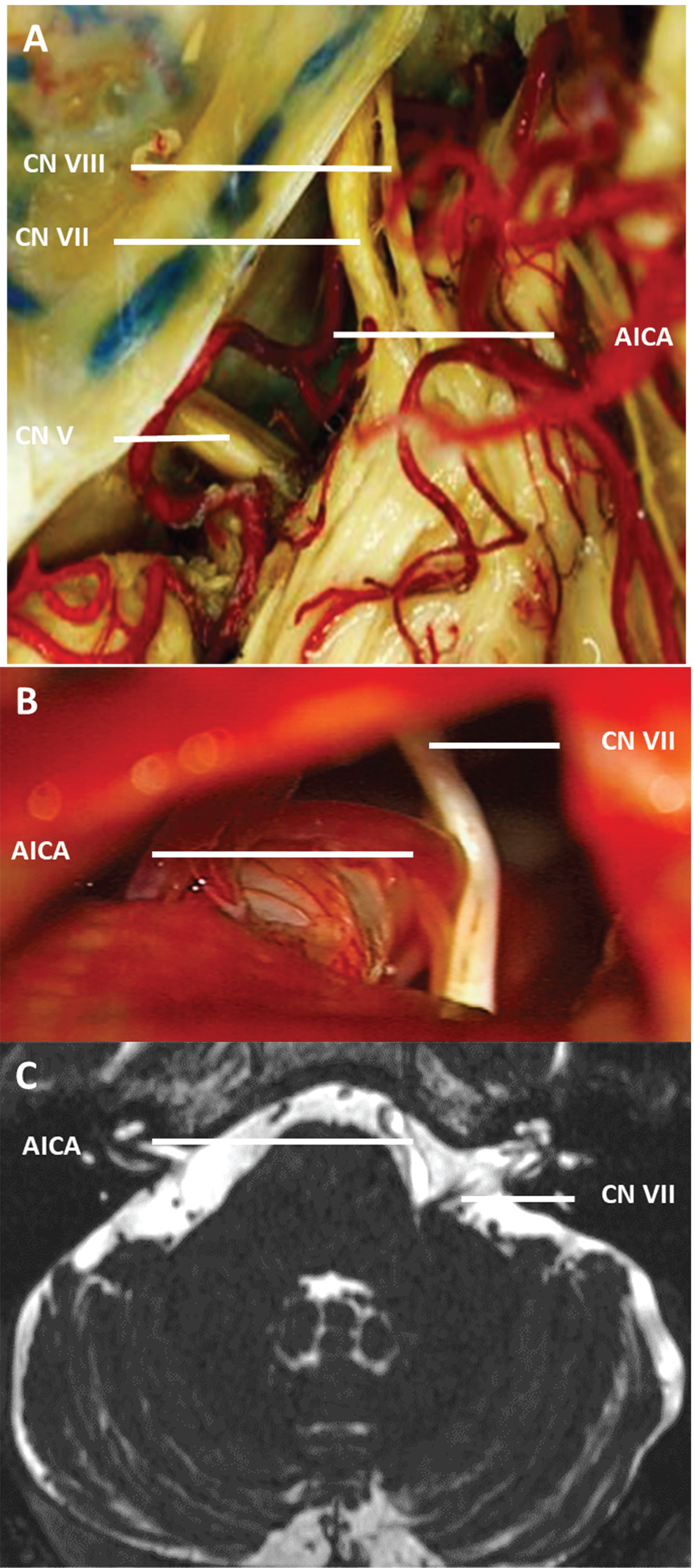 Figure 2: AICA is the most common compression on the facial nerve (A) Anatomical relationship between CN VII and AICA is shown in the cadaver dissection images; (B) Compression by AICA from the inferior part of the nerve is visible in the intraoperative image; (C) Preoperative CN VII and AICA compression image in axial T2 MRI sequence is shown.
Figure 2: AICA is the most common compression on the facial nerve (A) Anatomical relationship between CN VII and AICA is shown in the cadaver dissection images; (B) Compression by AICA from the inferior part of the nerve is visible in the intraoperative image; (C) Preoperative CN VII and AICA compression image in axial T2 MRI sequence is shown.
AICA: Anterior inferior cerebellar artery; CN: Cranial nerve; MRI: Magnetic resonance imaging.
View Figure 2
 Figure 3: PICA is the most common artery compressing inferior CNs (A) Anatomical relationship between CN IX-X-XII-XII and PICA is visible in the cadaver dissection images; (B) In the intraoperative image, inferior CN compression is caused by PICA; (C) Preoperative inferior CN and VA compression image in axial T2 MRI sequence are shown.
Figure 3: PICA is the most common artery compressing inferior CNs (A) Anatomical relationship between CN IX-X-XII-XII and PICA is visible in the cadaver dissection images; (B) In the intraoperative image, inferior CN compression is caused by PICA; (C) Preoperative inferior CN and VA compression image in axial T2 MRI sequence are shown.
PICA: Posterior inferior cerebellar artery; CN: Cranial nerve; MRI: Magnetic resonance imaging; VA: Vertabral artery.
View Figure 3
In 114 patients, compression by SCA were from the superior part of the nerve (n = 45, 40.7%), anterosuperior compression (n = 25, 21.9%), anterior compression (n = 24, 21.9%), inferior compression (n = 12, 11.4%), anteroinferior compression (n = 5, 5.2%), medial compression (n = 1, 0.8%), posteroinferior compression (n = 1, 0.8%), and posterior compression (n = 1, 0.8%); no compression was detected from the posterosuperior part of the nerve. The results indicate that SCA compressions were easier to identify than compressions observed during the operation. SCA compressions were classified into five types, except for the types that appear one which medial, posteroinferior, and posterior compression (Figure 4). Superior compression was defined as Type 1 (n = 45, 39.4%), which was further divided into three different subgroups: Type 1a (most common and classic form of superior compression, n = 24, 52.1%), Type 1b (anterior vein compression, n = 14, 30.4%), and Type 1c (inferior vein compression, n = 7, 15.5%). Anterosuperior compressions were classified as Type 2 (n = 25, 21.9%) and subdivided as Type 2a (most common type with only anterosuperior compression, n = 13, 52%), Type 2b (simultaneous arterial pressure is present in the compression was from the superior part of the nerve, n = 5, 20%), Type 2c (accompanied by vein compression from the posterior compression, n = 4, 16%), and Type 2d (compression by the vein from the anterior compression, n = 3, 12%). Anterior compression was defined as Type 3 (n = 24, 21%) and subdivided as Type 3a (the classic type and has only anterior compression, n = 17, 70.8%), Type 3b (accompanied by the posterior vein compression, n = 4, 16.6%), Type 3c (accompanied by the anterosuperior vein compression, n = 2, 8.3%), and Type 3d (accompanied by anterior artery compression, n = 1, 4.1%). Inferior compression was defined as Type 4 (n = 12, 10.5%) and divided into three subgroups: Type 4a (the classic type, n = 8, 66.5%), Type 4b (accompanied by inferior vein compression, n = 3, 25%), and Type 4c (accompanied by anterosuperior vein compression, n = 1, 8.3%). In patients with anteroinferior compression (4.3%), we found that there was only compression from the same way in one aspect and we called it Type 5.
 Figure 4: Illustrative images of the positions of SCA compression and cranial nerves. Except for the types with medial, posteroinferior, and posterior compression, SCA compression was classified into five types (A) Superior compression was defined as Type 1, which was further divided into three subgroups: Type 1a (the most common and classic form of superior compression), Type 1b (anterior vein compression), and Type 1c (inferior vein compression); (B) An illustration of the anterior SCA compression, which is common in 21% of cases (Type 3). Type 3a is the classic type and has only anterior compression, Type 3b is accompanied by posterior vein compression, Type 3c is accompanied by anterosuperior vein compression, and Type 3d is accompanied by anterior artery compression; (C) Inferior compression was classified as Type 4 and divided into three subgroups: Type 4a, the classic type; Type 4b, which is accompanied by inferior vein compression; and Type 4c, which is accompanied by anterosuperior vein.
Figure 4: Illustrative images of the positions of SCA compression and cranial nerves. Except for the types with medial, posteroinferior, and posterior compression, SCA compression was classified into five types (A) Superior compression was defined as Type 1, which was further divided into three subgroups: Type 1a (the most common and classic form of superior compression), Type 1b (anterior vein compression), and Type 1c (inferior vein compression); (B) An illustration of the anterior SCA compression, which is common in 21% of cases (Type 3). Type 3a is the classic type and has only anterior compression, Type 3b is accompanied by posterior vein compression, Type 3c is accompanied by anterosuperior vein compression, and Type 3d is accompanied by anterior artery compression; (C) Inferior compression was classified as Type 4 and divided into three subgroups: Type 4a, the classic type; Type 4b, which is accompanied by inferior vein compression; and Type 4c, which is accompanied by anterosuperior vein.
SCA, superior cerebellar artery.
View Figure 4
A total of 39 patients had AICA compression involving the following compression: inferior compression in 24 (61.5%) patients, anterior compression in 7 (17.9%) patients, anteroinferior compression in 4 (10.2%) patients, anterosuperior compression in 1 (2.5%) patient, medial compression in 1 (2.5%) patient, posteroinferior compression in 1 (2.5%) patient, and posterior compression in 1 (2.5%) patient; no compression was noted from the superior and posterosuperior the part of the nerves (Figure 5). These AICA compressions were subdivided into three types, excluding those involving the anterosuperior, medial, posteroinferior, and posterior compression: Type 1 (inferior compression, 61.5%), which was further classified as Type 1a (the most common and classic form, n = 18, 75%) and Type 1b (accompanied by the superior artery compression, n = 6, 25%); Type 2 (anterior AICA compression, n = 7) with Type 2a (unilateral compression, n = 5, 71.4%), and Type 2b (bilateral compression, n = 2, 28.5%); and Type 3 (anteroinferior compressions, n = 4, 10.2%).
 Figure 5: AICA compression involves the following compression types: inferior, anterior, anteroinferior, anterosuperior, medial, posteroinferior, and posterior compression. No compression was noted from the superior and posterosuperior parts of the nerves (A) Visual form of the inferior compression of AICA on CN VII. This position of compression is the most common. Type 1 was further classified as Type 1a and Type 1b. Type 1a is the most common and classic form, and Type 1b is accompanied by superior artery compression; (B) Illustration of compression by AICA from the anterior part of the nerve is shown. In terms of anterior compression, Type 2 was further classified as Type 2a and Type 2b. Type 2a unilateral compression was 71.4%, and Type 2b bilateral compression was 28.5%; (C) Image of the compression by AICA from the anteroinferior part of the nerve is shown.
Figure 5: AICA compression involves the following compression types: inferior, anterior, anteroinferior, anterosuperior, medial, posteroinferior, and posterior compression. No compression was noted from the superior and posterosuperior parts of the nerves (A) Visual form of the inferior compression of AICA on CN VII. This position of compression is the most common. Type 1 was further classified as Type 1a and Type 1b. Type 1a is the most common and classic form, and Type 1b is accompanied by superior artery compression; (B) Illustration of compression by AICA from the anterior part of the nerve is shown. In terms of anterior compression, Type 2 was further classified as Type 2a and Type 2b. Type 2a unilateral compression was 71.4%, and Type 2b bilateral compression was 28.5%; (C) Image of the compression by AICA from the anteroinferior part of the nerve is shown.
AICA: Anterior Inferior Cerebellar Artery; CN: Cranial Nerve.
View Figure 5
VA compressions were noted in 19 patients: Compression was from the inferior part of the nerve in 11 (57.8%) patients, compression was from the anteroinferior part of the nerve in 3 (15.7%) patients, anterior compressionin 2 (10.5%) patients, anterosuperior compressionnerve in 1 (11.1%) patient, medial compressionin 1 (11.1%) patient, and superior compressionin 1 (11.1%) patient; no compression was noted from the posterior, posteroinferior, and posterosuperiorpart of the nerves (Figure 6). These VA compressions were divided it into 4 types, excluding the anterosuperior and medial compressions: Type 1 (inferior compression), Type 2 (anteroinferior compressions) with Type 2a (only anterior VA compression, n = 2, 66.6%) and Type 2b (posterior vein compression, n = 1, 33.3%), and Type 3 (anterior compression).
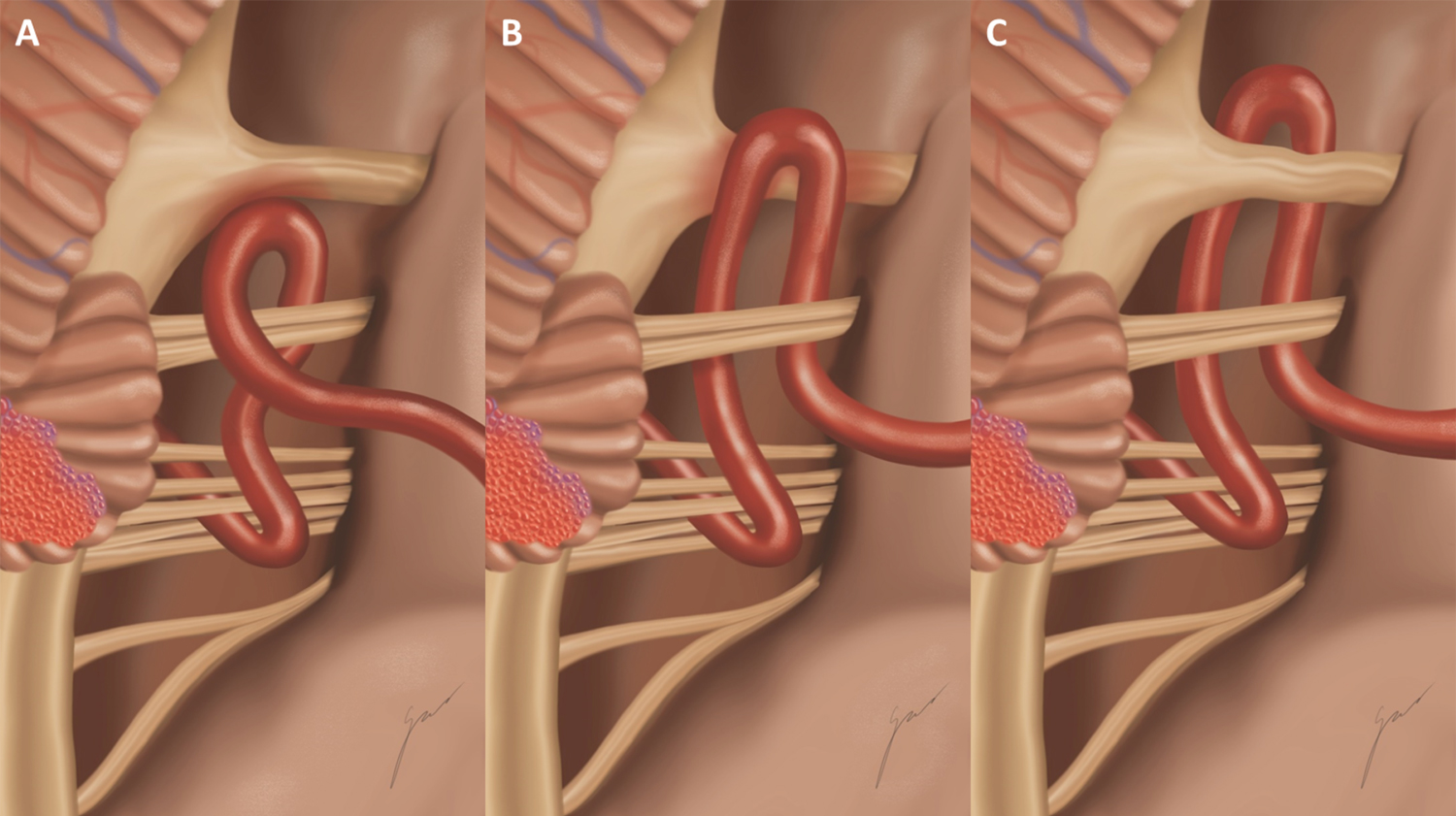 Figure 6: Compression of the inferior cranial nerves was caused by PICA, VA, and BA (A) Illustration of VA compression from the inferior part of the nerve. This position of compression is the most common (Type 1); (B) Illustration of VA anteroinferior compression, also known as Type 2 compression, which is the second most common. Type 2a affects only anterior VA compression, whereas Type 2b affects posterior vein compression; (C) Image of VA compression from the anterior part of the nerve, which we call Type 3.
Figure 6: Compression of the inferior cranial nerves was caused by PICA, VA, and BA (A) Illustration of VA compression from the inferior part of the nerve. This position of compression is the most common (Type 1); (B) Illustration of VA anteroinferior compression, also known as Type 2 compression, which is the second most common. Type 2a affects only anterior VA compression, whereas Type 2b affects posterior vein compression; (C) Image of VA compression from the anterior part of the nerve, which we call Type 3.
PICA: Posterior inferior cerebellar artery; VA: Vertabral artery; BA: Basillar artery.
View Figure 6
Vein compressions were detected from inferior compression in 26 (31.3%) patients, anterior compression in 9 (10.8%) patients, anteroinferior compression in 3 (3.6%) patients, anterosuperior compression in 3 (3.6%) patients, posteroinferior compression in 3 (3.6%) patients, inferomedial compression in 1 (1.2%) patient, superior compression in 17 (20.4%) patients, and posterior compression in 16 (19.2%) patients; no compression from the superiorpart of the nerve was detected.
PICA compressions from the inferior and medial compression were noted in 2 (1.2%) patients and BA compression from the inferior part of nerves in 1 (0.6%) patient.
With respect to cranial nerves, most of CN V compressions were caused by SCA, CN VII compression by AICA, and inferior cranial nerve compression caused by PICA. Majority of the SCA compressions were from the superior part of nerves, while most of the AICA compressions were from the inferior part of nerves. Compression of the inferior cranial nerves was caused by PICA, VA, and BA.
Neurovascular syndromes refer to the compression of the cranial nerves by vascular structures, and NVSC is a syndrome involving TN, HFS, and GPN. These nerve compression syndromes are often compressed by the relevant nerve at the REZ [3,4].
CN V compression causes TN, previously called tic douloureux. CN V is a group of nerves responsible for the motor and sensory innervation of the face. The ophthalmic (V1), maxillary (V2), and mandibular (V3) nerves are the main branches of CN V and join the Gasserian ganglion from their cisternal portion. TN is a common NVSC defined as a vascular compression of any part of the nerve from Meckel's cave to the entrance to the brainstem (REZ). It has an approximate incidence of 4.7/100,000. It is a syndrome characterized with pain that is not only strongly painful but also similar to pain like an electrical shock, sudden, unexpected, paroxysmally, and short term. Patients usually report a stabbing sensation in the cheek, the area of the nostrils, teeth, or jaw, which is very characteristic symptomatology of TN. TN has three types; classic, secondary, and idiopathic TN. Classic TN originates from vascular compression by the root entry zone of the trigeminal nerve [5,6]. Secondary TN includes different diseases, such as demyelinating disease, neoplastic processes, and traumatic events [7,8]. Idiopathic TN is characterized by signs and symptoms compatible with TN but without other causes after detailed examinations.
CN VII is a mixed nerve like CN V that controls muscles. HFS occurs if CN VII is compressed by vascular structures, in facial REZ, in the pontomedullary sulcus. It is a syndrome characterized by paroxysmal involuntary muscle contractions on one side of the face and an uncontrolled contraction of the facial muscles and one of the most common hyperactive cranial rhizopathies.
GPN originates from compression at the level of the root exit zone of CN IX and X. CN IX includes sensory, motor, and parasympathetic nerves: Its sensory part is connected to the posterior tongue and oropharyngeal and ear region; the motor component is stimulated by the stylopharyngeal muscle and the parotid gland, and the parasympathetic part consists of the carotid body and carotid sinuses signals. GPN is a rare syndrome, with an incidence of only 0.2-1.3%. GPN is an uncommon pain characterized by a stabbing sensation at the back of the tongue, the pharynx, and the internal ear canal. It is triggered by swallowing, coughing, or sneezing.
MVD is the best and most effective treatment for TN, HFS, and GPN [9,10]. MVD was described by W. James Gardner in 1959 and has become popular over time as the gold standard for the treatment of vascular compression. Peter Jannetta in 1970 presented the modern MVD operation and then Jules Hardy followed them [11]. Thus, knowledge of the structures that cause vascular compression and their anatomical placement is crucial in treatment success.
Barker, et al. evaluated 1185 patients and found that the vascular structure that most often causes TN was SCA, followed by AICA and PICA [12], which was consistent with the findings of Bohman, et al. who assessed 47 patients [13]. Türkkan, et al. reported that in 197 cases of TN, 118 (60.82%) were detected to commonly originate from SCA [14], which was similar to the findings of Tanrikulu, et al. in 85 (59%) of 180 cases of TN [15]. In contrast, Xia, et al. showed that in their 228 cases of GPN, 165 (72.3%) were caused by PICA alone and 14 (6.1%) by VA alone [16]. Tanrıkulu, et al. reported that PICA was the most common causative vessel in 12 of 15 patients (80%) [17].
In other studies, HFS was most commonly caused by AICA. Reports from Huang, et al. [18], Shin, et al. [19], Ishikawa, et al. [20], Samii, et al. [21], Li, et al. [22], Yamashita, et al. [23], Yuan, et al. [24], Dannenbaum, et al. [25], Joo, et al. [26], Kim, et al. [27], Hyun, et al. [28], Wook Jo, et al. [29], Baron, et al. [30], Shimizu, et al. [31], Auger, et al. [32], Lee, et al. [33], Campos- Kaufmann, et al. [4], Park, et al. [34], and Naraghi, et al. [35] reported the following incidence: 39%, 51%, 49%, 55.2%, 39.8%, 51.7%, 42.6%, 43%, 44.4%, 53.9%, 53.2%, 54.2%, 75.8%, 23%, 37%, 63.6%, 43%, 74.2%, and 60%, respectively.
In our case series, most CN V compression was caused by SCA, most compression CN VII compression by AICA, and most inferior CN compression by PICA. Most SCA compressions were superior Type1a, and most AICA compressions were inferior Type1a. In addition, compression of the inferior CNs was caused by PICA, VA, and BA, and we identified the most common cause of compression was the VA from inferior part of nerves.
In the present study, the incidence of both arterial and vein compressions was 15.3%. For this reason, patients with vein compression during surgery should be awake during arterial compression after decompression (or vice versa). Possible and most frequent sites of pressure should be carefully examined.
In our literature review, the most common vessels that make compression with the series of cases reported for TN, HFS, and GPN are largely in line with the results of the present study. However, we could not find collective data in the literature regarding vascular structures that cause the most frequent compressions in which these neurovascular syndromes coexist, as well as their classification and their aspects. In the present study, we presented the ratio of vascular nerve packets that cause NVSC and the compression aspects of the most common vascular structures, as well as the related classification that have not been previously defined in the literature.
Sükrü Aykol hand-drawing techniques will help you to follow-up treatment and understand the future period after the surgeries as our mentor did (Figure 7). Although there is no new information in our article as a main line, the dominance of anatomy will be easier to understand with this classification. Because the way of compression that causes pain and the surgical procedure performed accordingly are very important in the follow-up and treatment of patients with the neurovascular syndrome. In order to make the correct diagnosis and treatment, it is necessary to have a good understanding of the anatomy and compression variations.
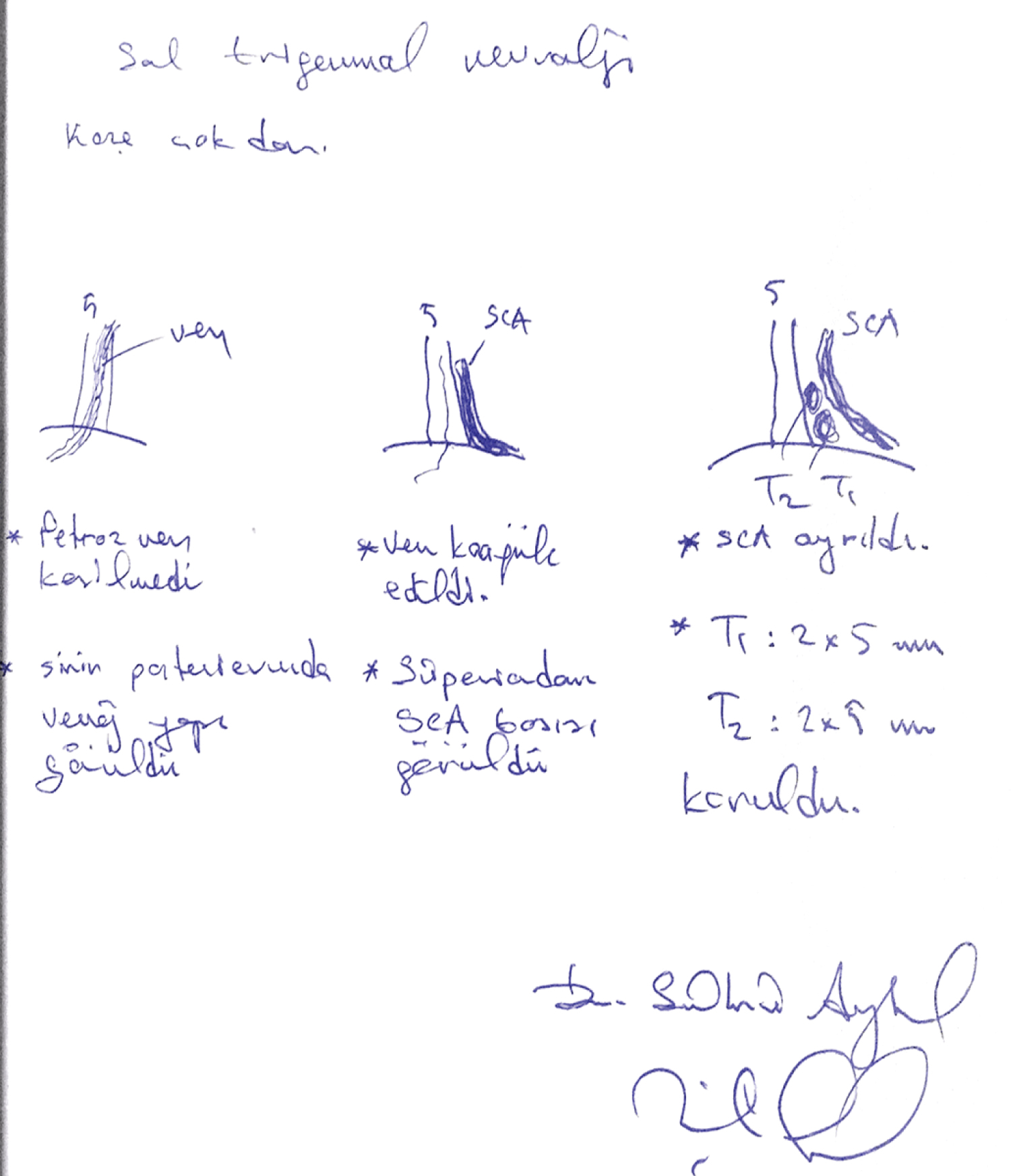 Figure 7: Hand-drawn image of cranial nerve and vascular compression after surgery by Prof. Dr. Şükrü Aykol.
View Figure 7
Figure 7: Hand-drawn image of cranial nerve and vascular compression after surgery by Prof. Dr. Şükrü Aykol.
View Figure 7
MVD is the best treatment method for CN compression caused by vascular structures among other options including stereotactic radiosurgery, radiofrequency rhizotomy, glycerol injections, and balloon compression. Especially in cases of multiple compressions, knowledge of the most common vascular compressions during MVD surgery is crucial in order to perform surgery with confidence.
We would like to express our gratitude to our very valuable, deceased mentor Prof. Şükrü Aykol, who did not withhold his support from us for this article and enriched our literature by sharing his surgery data with us.
We certify that the content of this manuscript, in part or in full, has not been submitted to any other journal in any form, and its publication has been approved by all co-authors.
The study does not require the approval of the ethics committee.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
The authors declare that they have no conflict of interest.