Introduction: Posterior cerebral artery (ACP) aneurysms account for less than 2% of all aneurysms. The fronto-temporo-zygomatic approach allows access to the cranial base with less parenchymal damage. Endoscopy allows you to visualize deep structures. Fluorescein allows to verify the permeability after clipping.
Clinical case: A 44-year-old woman with subarachnoid hemorrhage (SAH), CT angiography shows an aneurysm of the right posterior cerebral artery segment P1/P2. A fronto-temporo-zygomatic craniotomy was performed for the clipping of the aneurysm. Permeability was confirmed with fluorescein and verified with endoscopic review. It was presented with alteration of the III pair that progressively.
Conclusion: P1/P2 segment aneurysm surgery, associated with video angiography and endoscopy, ensured correct clipping and permeability of the posterior brain and collaterals. We corroborated with the literature, regarding a lower rate of complications through a fronto-temporo-zygomatic approach, endoscopic assistance and intraoperative video angiography.
Intracranial aneurysm, Posterior cerebral artery, Fluorescein angiography, Endoscopy
Posterior cerebral artery (PCA) aneurysms are rare lesions [1-4], accounting for between 0.7 and 2.2% of all intracranial aneurysms [2,3,5], between 7-15% of posterior circulation aneurysms occur at junction P1/P2 [2-4]. The ACP is divided into segments P1, P2, P3 and P4. Different types of sacular, fusiform, dissecting, and serpentine aneurysms can develop from the basilar artery to the cortical branches [6].
The fronto-temporo-zygomatic approach is used to treat tumors and vascular lesions located deep in the middle fossa, the cavernous sinus, and the upper part of the clivus [6]. It allows a wider surgical vision, safe manipulation of the optic nerve [7], better exposure with less brain retraction through the resection of the edge of the orbital roof, orbital lateral wall, and zygomatic arch [6]. It is the gold standard in skull base surgeries with simple execution, versatility, and low morbidity [8].
Videoangiography (AV) with sodium fluorescein (NaF) is used in cerebrovascular surgery for a better visualization of patency after microsurgical clipping [9-11]; endoscopic help corroborates the correct clipping in areas not visible under the microscope, contributing to the safety and efficacy of surgery [12].
A 44-year-old woman with sudden and intense headache attended the emergency room, received analgesics and the tomography showed subarachnoid hemorrhage so she was referred to a higher resolution Hospital, studies were completed with cerebral angiography and the rupture of a saccular aneurysm in the right posterior cerebral artery of segment P1/P2 was confirmed (Figure 1). On examination we found a patient with headache of intensity 7/10, Glasgow: 15, without motor or sensory deficit, preserved cranial nerves, reactive isochoric pupils and neck stiffness (++/+++).
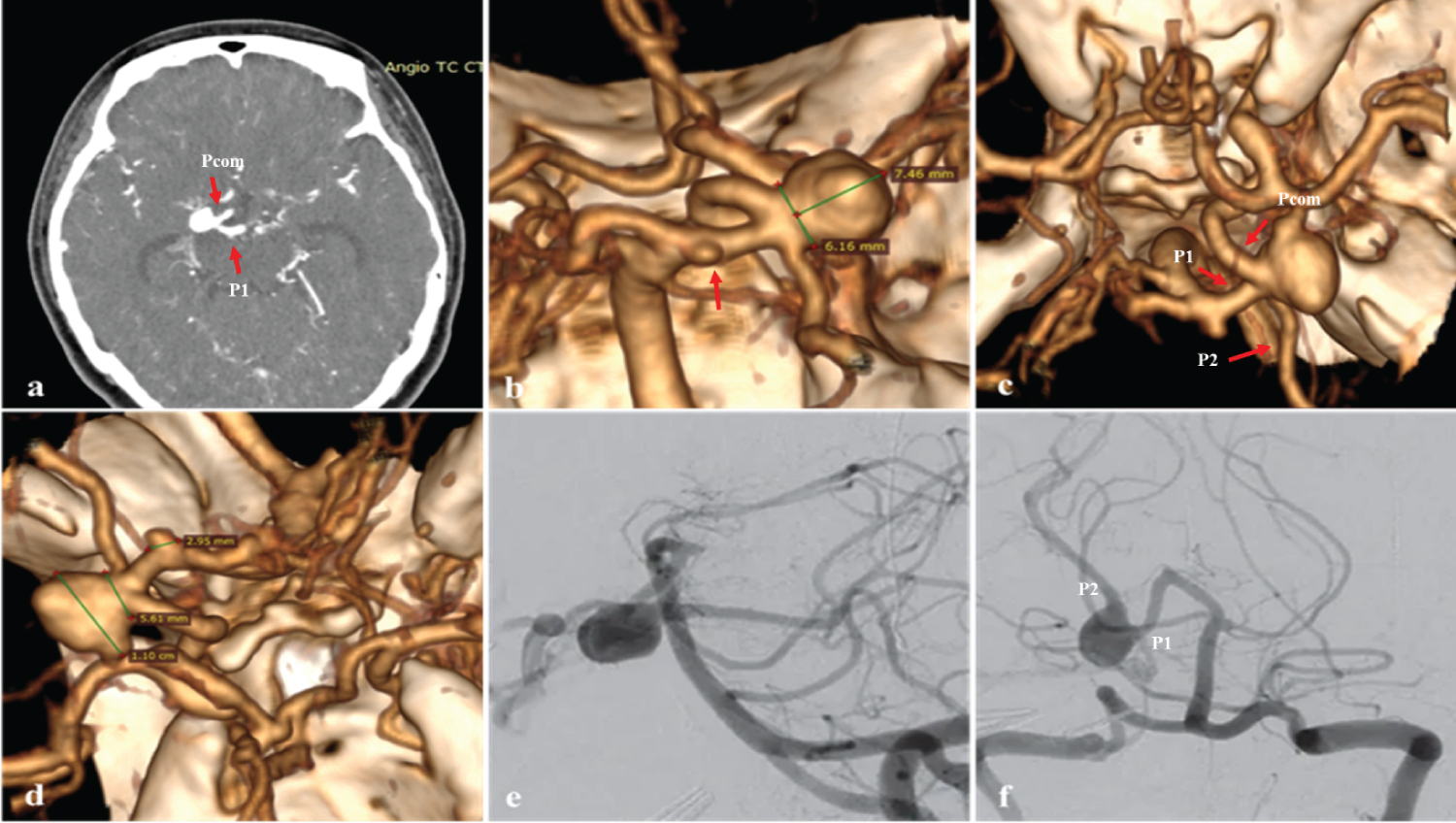 Figure 1: (a, b, c and d) 3D CT angiography of the arteries at the base of the skull to observe the aneurysm in the posterior cerebral artery. a) Axial section shows aneurysm at the P1/Pcom junction (red arrow);b) Posterior view, microaneurysm at the top of the basilar artery (arrow); c) Superior view, aneurysm at the P1/P2/Pcom junction, fetal posterior communicating artery (arrow); d) Right lateral view, dimensions of the aneurysm in the PCA; e, f) Digital subtraction angiography, right P1/P2 segment aneurysm.
View Figure 1
Figure 1: (a, b, c and d) 3D CT angiography of the arteries at the base of the skull to observe the aneurysm in the posterior cerebral artery. a) Axial section shows aneurysm at the P1/Pcom junction (red arrow);b) Posterior view, microaneurysm at the top of the basilar artery (arrow); c) Superior view, aneurysm at the P1/P2/Pcom junction, fetal posterior communicating artery (arrow); d) Right lateral view, dimensions of the aneurysm in the PCA; e, f) Digital subtraction angiography, right P1/P2 segment aneurysm.
View Figure 1
A right fronto-temporo-zygomatic craniotomy was performed (Figure 2), wide dissection of the Silvian fissure, proximal control with temporal clipping of the basilar artery, and identification and clipping of the aneurysm. We corroborated the permeability of the posterior brain and collaterals with fluorescein and reviewed with the endoscope the area that did not allow us to observe the microscope and rule out the possibility of an inadvertent clipping of collaterals (Figure 3).
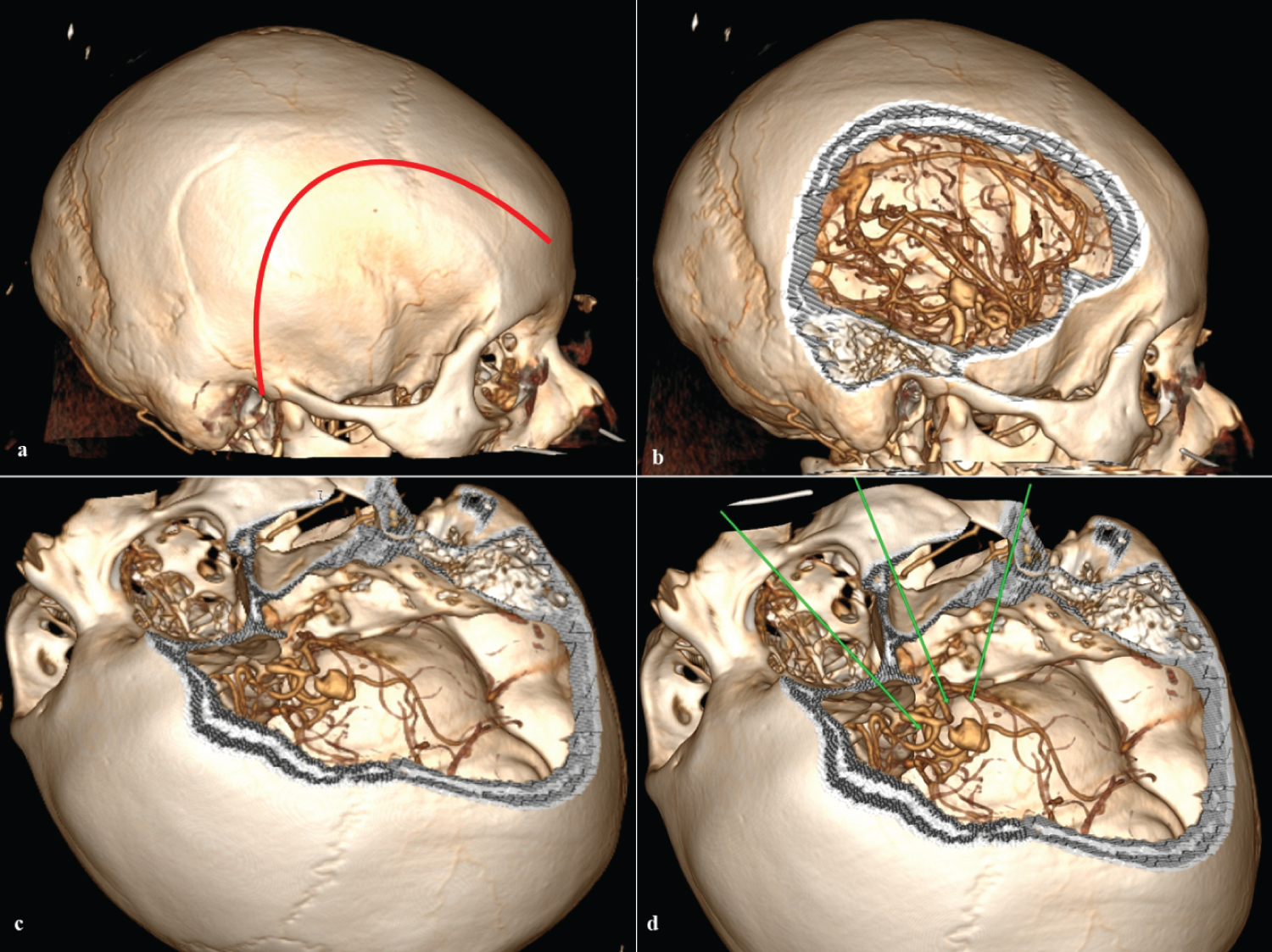 Figure 2: 3D tomography. a) Frontotemporal skin incision (red line); b) Right lateral view of right frontotemporal craniotomy; c) Surgical position and craniotomy with zygomatic frontotemporal enlargement; d) Surgical position and access corridors to the aneurysm (green line).
View Figure 2
Figure 2: 3D tomography. a) Frontotemporal skin incision (red line); b) Right lateral view of right frontotemporal craniotomy; c) Surgical position and craniotomy with zygomatic frontotemporal enlargement; d) Surgical position and access corridors to the aneurysm (green line).
View Figure 2
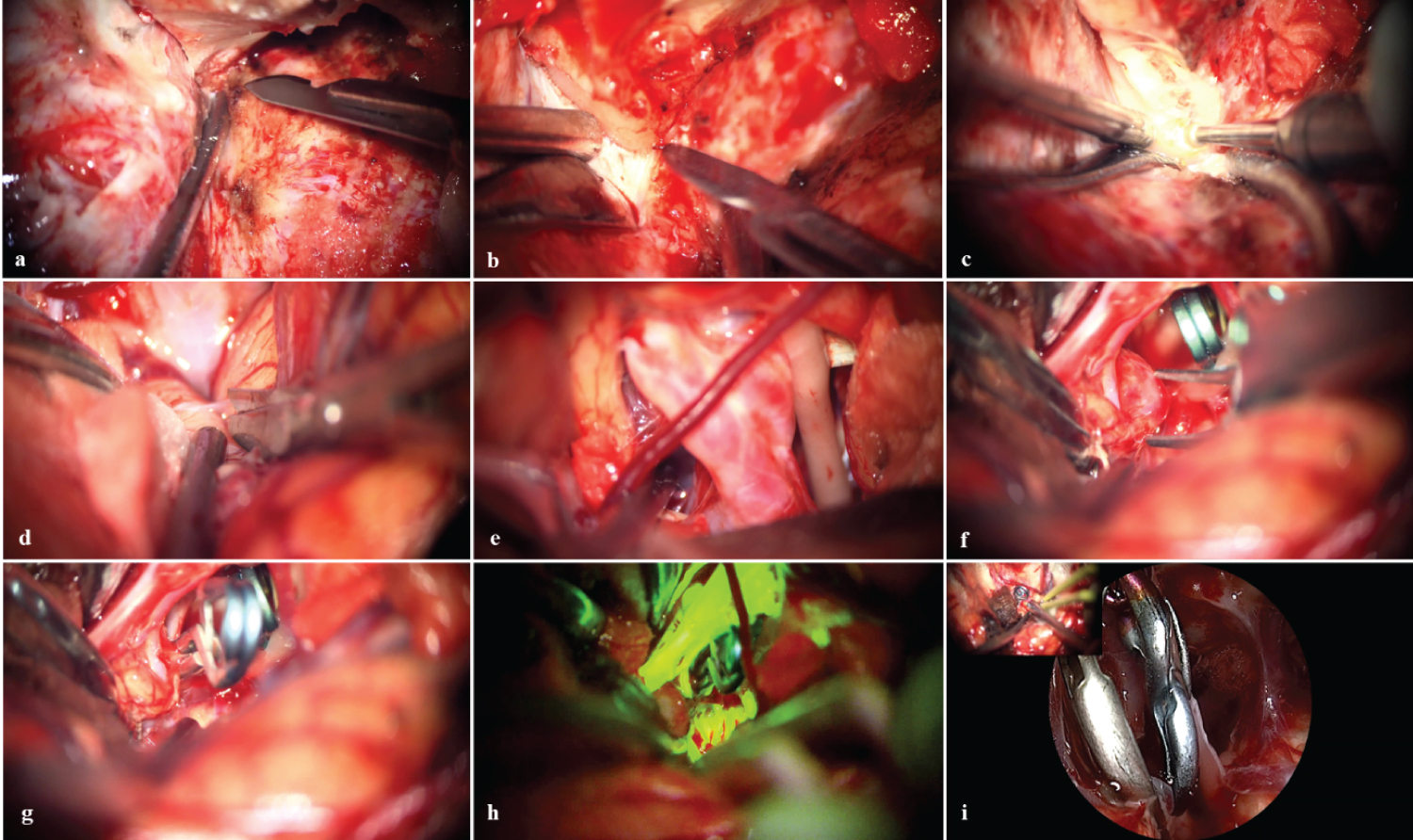 Figure 3: Microsurgical vision. a) Exposure of the sphenoid wing and posterior drilling; b) Mini-peeling of the middle fossa; c) Anterior extradural clinoidectomy; d) Wide opening of the Silviano valley; e) ACI-III bifurcation nc; f) Temporary clipping in basilar artery; g) Clipping and exclusion of P1 aneurysm; h) Fluorescein videoangiography corroborates P1-P2 exclusion and patency; i) Endoscopic visualization confirms patent branches adjacent to the neck.
View Figure 3
Figure 3: Microsurgical vision. a) Exposure of the sphenoid wing and posterior drilling; b) Mini-peeling of the middle fossa; c) Anterior extradural clinoidectomy; d) Wide opening of the Silviano valley; e) ACI-III bifurcation nc; f) Temporary clipping in basilar artery; g) Clipping and exclusion of P1 aneurysm; h) Fluorescein videoangiography corroborates P1-P2 exclusion and patency; i) Endoscopic visualization confirms patent branches adjacent to the neck.
View Figure 3
In the postoperative period in the intensive care unit we observed paresis of the right cranial nerve III, remains 3 days and with good evolution passes to hospitalization. After 7 days she was discharged, with favorable neurological evolution, Glasgow: 15; paresis of the right pair III, wound without complications with modified Rankin scale (SRm: 1). In the control at 2 weeks there was evidence of improvement of the nerve III pair and in the control at 3 months a clear improvement in the function of the III cranial nerve and with SRm: 0 (Figure 4).
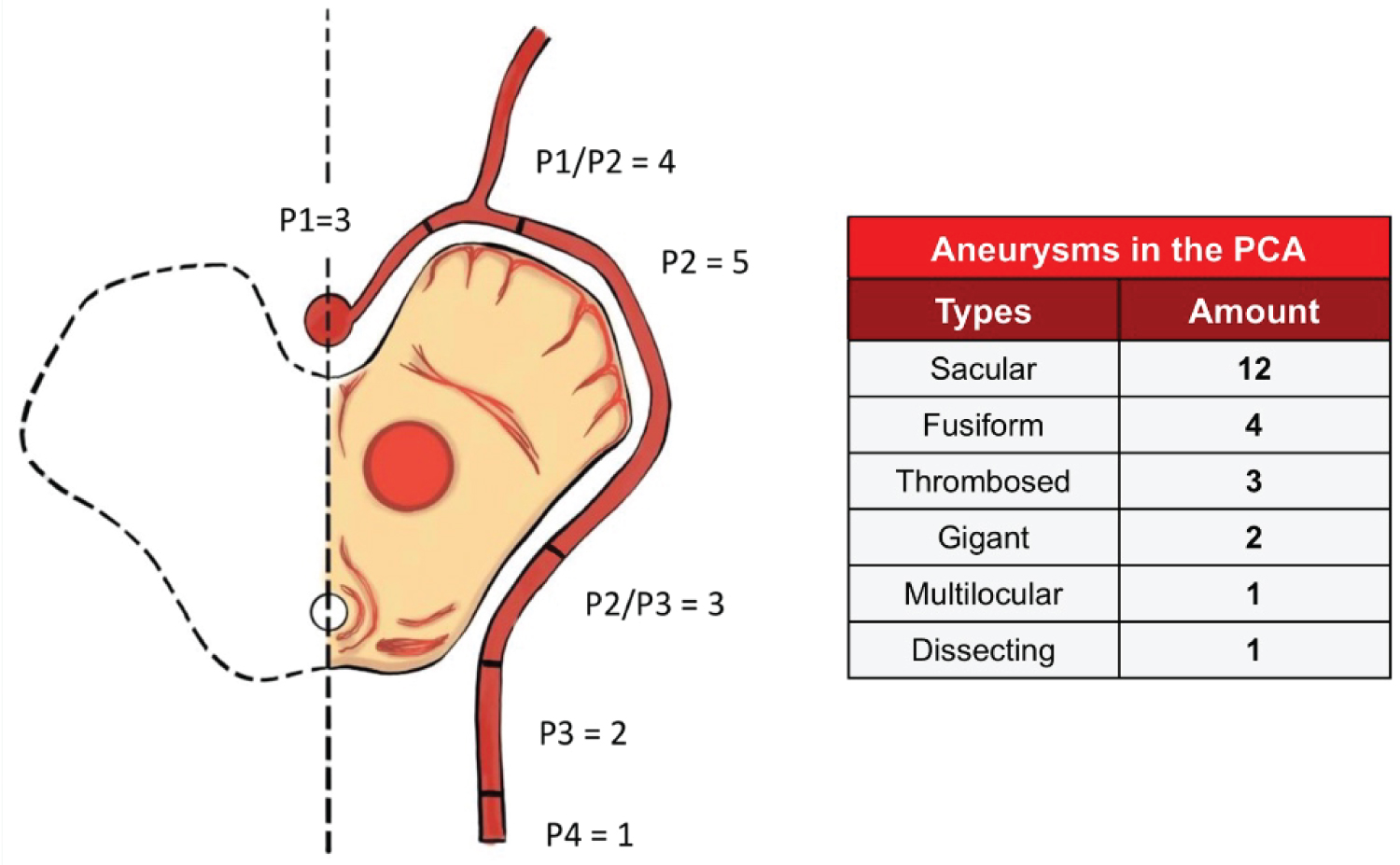 Figure 4: Scheme on the distribution of aneurysms in the posterior cerebral artery according to the review of the literature, classified into segments and types of aneurysms. Adaptaded from: Ros J, Cuartero B. Completely thrombosed aneurysms of the posterior cerebral artery: A comprehensive review.
View Figure 4
Figure 4: Scheme on the distribution of aneurysms in the posterior cerebral artery according to the review of the literature, classified into segments and types of aneurysms. Adaptaded from: Ros J, Cuartero B. Completely thrombosed aneurysms of the posterior cerebral artery: A comprehensive review.
View Figure 4
Between 2018 and 2021, at the Hospital Nacional Dos de Mayo we operated on 3 cases of aneurysms in the posterior circulation, out of 236 patients operated on for aneurysms [13]. Corroborated by the literature indicating a prevalence of less than 2.2% of aneurysms in the posterior cerebral artery of all intracranial aneurysms [2-4] (Table 1).
Table 1: Literature review of case reports and case series on posterior cerebral artery aneurysms. View Table 1
The evolution of posterior cerebral artery aneurysms may present variable hemodynamic characteristics, one of the main factors for their growth being the energy transferred from the bloodstream to the arterial wall [14]. Prevocating its growth even to sizes greater than 30 mm with a 6% risk of rupture in the first year [14,15].
The clinical picture varies according to the affected segment and the neighboring structures involved; The most common symptoms are: headache, decreased visual acuity, ptosis, dizziness, diplopia and hemiparesis [16,17].
The surgery options require a wide field of work for deep access to the posterior circulation, being relevant the variants of the pterional technique [18]. Subtemporal and transylvic approaches are widely used in aneurysms from P1 to P3, as Drake reports on the advantages of securing the blood vessels surrounding the aneurysm during the subtemporal approach [19]. However, from P2 it is already difficult to reach the most distal parts of the posterior brain and requires an excessive retraction of the temporal [20,21]. These techniques are associated with involvement of the III and/or IV cranial nerve and thalamic infarction [19-22]. Uygur already highlighted the importance of the fronto-temporo-zygomatic approach, basic in skull base surgery to improve the exposure of deep structures to minimize brain retraction. However, there were insufficient data on functional and aesthetic outcomes [23]. Boari in 2018 reported 169 patients who underwent this type of approach, evaluating precisely the functional and aesthetic results, including subjective satisfaction in 90% of patients without affecting their quality of life [8].
We measure our result compared with the results of other reviews conducted on the surgical treatment of posterior cerebral artery aneurysms, where cases of cranial nerve III palsy, quadrantanopsia and other alterations of the visual field, hemiplegia, hemiparesis and diplopia are presented [19,24-26].
The use of fluorescein video angiography showed a direct relationship with a decrease in postoperative complications and higher success rates in surgeries [9,11]. In our case we allowed to verify the definitive clip je of the aneurysm, avoiding the adjacent vascular damage. Endoscopy allowed us to observe structures that are not accessible through the field of view offered by the surgical microscope [12].
In this case, we seek to enhance the benefits of these techniques towards a better visualization of the anatomical structures around the aneurysm, for a better dissection and clipping, minimizing the retraction of the structures and reducing morbidity; Therefore, endoscope-assisted microsurgery is complemented in deep lesions, especially those in which the microscope does not allow adequate visualization of structures, such as aneurysms of the posterior circulation [27].
Fischer, et al. found that, without endoscopy, the rates of incomplete clipping and perforator occlusion were 18.9% and 8.3%, respectively, in a series of 180 cases [28]. However, disadvantages in its use are also described: constant introduction and removal of the endoscope from the surgical field (by change of modality between the endoscope and the microscope). Therefore, to maintain endoscopic and microscopic vision simultaneously, it is necessary to incorporate imaging functions by intraoperative video angiography [29].
Our patient in the postoperative period presented as a complication paresis of the right cranial III nerve which shows a clear improvement at 3 months.
Posterior cerebral artery aneurysms are rare and challenge the abilities of neurosurgeons due to anatomical nuances, large number of perforants and risk of bleeding. However, surgery for these aneurysms is technically feasible, safe and effective when performed respecting microsurgical principles.
This aneurysm represented a challenge for us due to its deep location, difficult exposure, limited surgical field, adjacent cranial and perforating nerves. A safe clipping was achieved but we present a transient paresis of the III pair crane by manipulation, without long-term sequelae. Neuroendoscope (Kevo) and fluorescein video angiography were important during surgery for clipping safety.
The presentation of the case allows us to corroborate what was found in the literature review, mainly regarding the lower rate of complications in patients with aneurysm in the posterior cerebral artery who underwent clipping using a fronto-temporo-zygomatic approach complemented by the use of video angiography with sodium fluorescein and intraoperative endoscopy.